골반저 질환에서 회음부초음파 검사의 유용성 – 대장항문외과의 영역
서울 양병원 대장항문외과
신현근
Transperineal Ultrasonography for Pelvic Floor Disorders – in the Aspect of Colorectal Surgeon
Hyeon-Keun Shin
Division of Colorectal Surgery, Department of Surgery, Seoul Yang Hospital, Seoul, Korea
Received July 9, 2015 Revised October 23, 2015 Accepted October 27, 2015
Ultrasonography has recently been used in the diagnosis of pelvic floor disorders and is re- placing conventional radiological methods. Transperineal ultrasonography can be used as an important diagnostic method for pelvic floor disorders to demonstrate the anatomy of the pelvic floor. This is a minimally invasive procedure providing an extensive perineal view.
Pelvic floor organ (including the bladder, uterus, anus and rectum) position, movement, and prolapse can be observed as a real-time imaging and may be used in diagnosis of obstructive defecation syndrome including rectocele, rectal intussusception, enterocele, and NRPR.
Imaging of these real movements can lead to a better understanding of the disorders and fa- vorable results can be expected after treatment. Other advantages include low costs and high availability. Finally, transperineal ultrasonography can be helpful in the diagnosis of ano- rectal or pelvic floor disorders.
Keywords: Pelvic floor disorders, ODS, Transperineal ultrasonography Correspondence to:
Hyeon-Keun Shin
Division of Colorectal Surgery, Department of Surgery, Seoul Yang Hospital, Seoul, Korea
Tel: +82-2-480-8007 Fax: +82-2-480-8119 E-mail: [email protected]
서 론
대장항문외과에서 진료하게 되는 변비 등의 증상을 호 소하는 환자들 중에는 골반저 질환과 연관된 복잡한 경우 도 드물지 않고, 이러한 골반저 질환들은 임상적으로 진단 하기에 쉽지 않은 질환이며, 골반저 구조물에 대한 해부학 적, 생리학적 기능들도 아직 확실하게 이해되고 있지 않 다. 특히 골반저 질환으로 호소하는 환자들의 증상과 의사 의 임상적 진찰소견이 일치하지 않을 때도 있다.(1) 임상 적 진료 시 외래에서 직장수지검사 등을 시행하여 어느 정
도 필요한 정보를 얻을 수 있으나 충분하다고 할 수 없고, 이러한 이유로 방사선검사가 시행되고 있다. 골반저 질환 에 대한 방사선 검사로 배변조영술(defecography)과 MRI (dynamic MR imaging)검사가 있다. 이 중 배변조영술 (defecography)이 대표적이며 흔히 사용되는 검사이지만 직장 외 다른 골반구조물들을 모두 관찰하기 어렵고 특수 한 장비와 시설이 필요하며 검사 시 방사선에 노출될 가능 성 등의 여러 가지 한계점들을 가지고 있다.(2) MRI검사 는 검사의 편의성 부분이나 고가의 장비로 인한 문제 등으 로 인해 흔히 사용되고 있지는 않다.(3) 이러한 단점들을 극
REVIEW ARTICLE
J Surg Ultrasound 2015;2:59-64 JSUJournal of Surgical Ultrasound
Fig. 1. 2-dimensional Ultrasound Machine. 파(endovaginal ultrasonography, EVUS), 경항문초음
파(endoanal ultrasonography, EAUS)가 있다.(4,5) 사 실 회음부초음파검사(TPUS)는 1995년 요실금 환자에서 방광경부(bladder neck)를 관찰하는데 처음으로 사용되 었다.(6) 회음부 초음파검사의 장점으로는 검사가 쉽고, 방사선노출의 위험이 없으며 검사 시 골반구조물들의 움 직임을 직접 관찰할 수 있다는 것이다.(7) 특히 배변장애 를 호소하는 환자를 진료할 때 배변과 유사한 상황 - 안정 시 및 힘주기(straining)- 에서 골반 내 전, 중, 후방 구획 (anterior, middle, posterior pelvic compartment)을 각 각 관찰할 수 있다.(8) 이스라엘의 Beer-Gabel et al.(4), 브라질의 Kleinübing et al.(9), 스위스의 Roche et al.
(10), 그리고 이탈리아의 Piloni (11)는 각각 회음부 후방 과 골반저에 대한 회음부초음파를 이용한 효과적인 검사 법을 보고하였다. 이러한 장점들은 그동안 모호하게 받아 들여졌던 골반저 질환에 대한 진료를 좀더 구체적으로 진 행할 수 있게 되고 치료-특히 수술적-에 이르기까지 도움 이 될 수 있다고 생각된다. 물론 초음파검사 소견이 항상 임상소견이나 환자증상과 일치하지는 않으며, 해부학적 교정이 반드시 기능의 개선으로 연결되지는 않는다.(12) 하지만 골반수술의 목표는 가능한 환자의 증상을 해결하 고 해부학적 결함과 기능을 교정하는 것이므로 회음부초 음파 검사를 이용하여 골반저에 대한 통합적 진료를 하는 것이 도움이 될 것이다. 현재까지 고가의 장비를 이용한 3D 초음파 검사 등이 소개되고 좋은 반응을 얻고 있기도 하지만 일선 진료현장에서 이러한 장비를 모두 갖추기는 무리가 있을 수 있고 따라서 일반적인 2D 초음파장비를 이용한 회음부 초음파 검사에 대하여 설명하고자 한다.
본 론
1. 검사목적
회음부초음파 검사를 시행하면 방광, 요도, 질 및 자궁, 항 문과 직장에 대한 전체 모양을 관찰할수 있다. 또한 안정시, 발살바 동작(Valsalva maneuver) 혹은 힘쓰기(straining) 동작 중의 골반저 구조물의 역동적인(dynamic) 움직임이 나 변화를 실시간으로(real-time) 직접 관찰할 수 있다.
drome) 등의 이상소견을 관찰할 수 있다.
2. 장비
회음부초음파검사를 위해선 일반적인 2D 초음파 검사 장비로도 충분하다. 일반적으로 3.5-7 MHz의 curved transducer를 사용한다(Fig. 1).
3. 검사방법
검사 전에 관장이 반드시 필요하지는 않으며, 필요한 경우 방광은 적당히 차 있는 것이 다른 구조물과의 감별에 도움이 된다. 다만 방광이 너무 차 있으면 장기의 탈출 (prolapsed)이 방해되어 검사가 올바르지 않을 수도 있 다. 환자를 앙와위에서 양측 무릎을 약간 굽힌 쇄석위를 취하게 한다. Curved transducer를 사용하여 mid-sag- ittal view를 얻는다. Probe 표면에 초음파검사용 젤을 바 른 후 외과용 글러브(powderless)를 덧씌운 후 젤을 추가 로 덧바른다. 이렇게 함으로써 검사 시 보다 선명한 영상 을 얻을 수 있다(Fig. 2). 회음부에 probe를 가볍게 밀착 시키면서 골반구조물을 확인한다(Fig. 3). 전방, 중간, 후 방 구획의 구조물을 볼 때마다 약간씩 probe의 각도를 달 리하여 원하는 구조물의 이미지를 확인한다.
Fig. 2. Transducer preparing with gel and powderless glove.
Fig. 3. (A) Transducer placement on perineum, reprinted from Dietz.(13) (B) Transducer placement and imaging of pelvic floor organ.
4. 정상구조물
앞쪽으로 치골결합(symphysis pubis)이 관찰되며 차 례로 요도, 질, 항문관과 직장이 보이고 그 뒤로 항문거근 판(levator plate)이 관찰된다. 치골결합과 항문거근판이
하나의 화면에 보여야 올바른 검사이다(Fig. 4). 안정 (resting)시와 발살바 동작(Valsalva maneuver) 혹은 힘 쓰기(straining) 동작시 치골결합과 항문거근판 사이의 거리를 측정하여 거근틈(levatoe hiatus)의 전-후(AP) 거
Fig. 4. Normal sagittal view of pelvic floor.
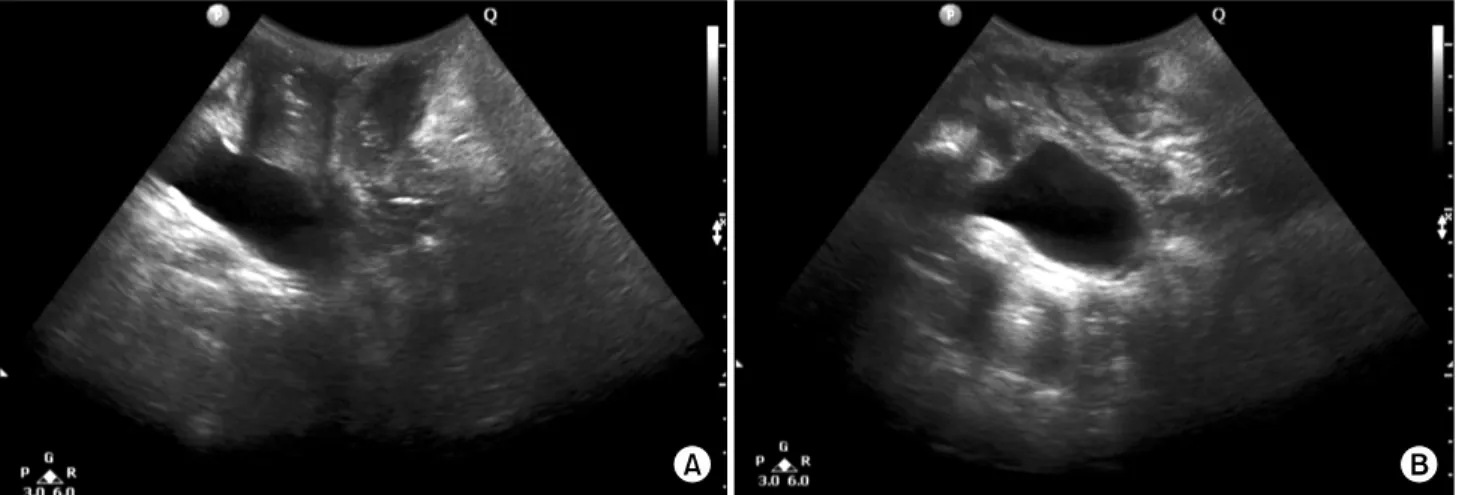
Fig. 5. Movement of anorectum, at rest& during straining. (A) At rest, (B) During straining.
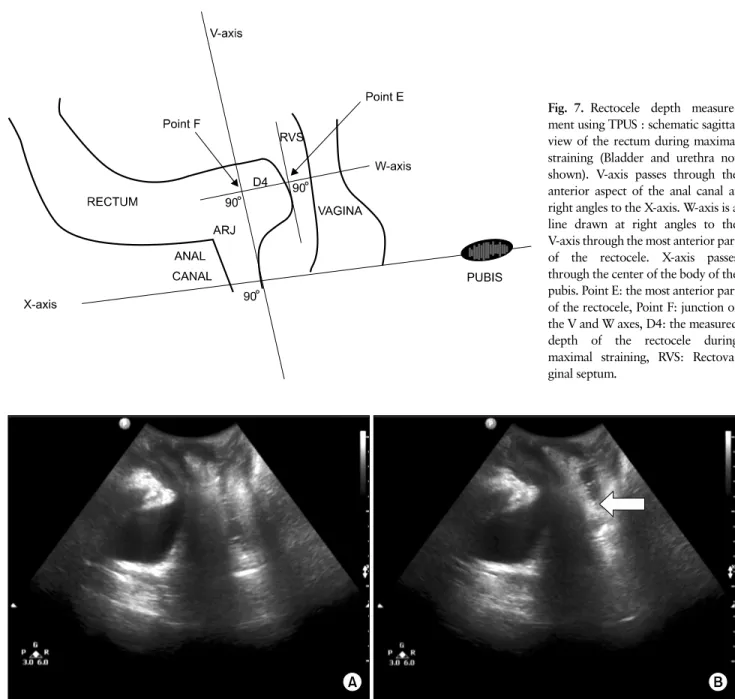
Fig. 6. Anterior rectocele in female patient. Anterior rectocele:
white arrow, R: rectum. 리를 알 수 있다(Fig. 5). 또한 이 둘의 연결선을 기준선으
로 하여 이보다 아래로 내려오는 경우를 탈출(prolapsed) 소견으로 판단할 수 있다.
5. 적응질환
직장류: 배변시 직장 전벽이 질쪽으로 돌출되는 것을 말하며, 돌출되는 정도가 10 mm 이상이면 초음파에서 직 장류로 진단할 수 있다(Fig. 6, 7). 하지만 현재까지 돌출 되는 정도와 증상이 일치하는지는 입증된 결과가 없다.
직장탈-직장중첩증: 직장벽이 직장관내로 밀려내려오 는 상태이며 폐쇄성 변비나 불완전 배변감등의 증상을 일 으키며, 경회음부 초음파에서 관찰할 수 있다(Fig. 8).
Fig. 7. Rectocele depth measure- ment using TPUS : schematic sagittal view of the rectum during maximal straining (Bladder and urethra not shown). V-axis passes through the anterior aspect of the anal canal at right angles to the X-axis. W-axis is a line drawn at right angles to the V-axis through the most anterior part of the rectocele. X-axis passes through the center of the body of the pubis. Point E: the most anterior part of the rectocele, Point F: junction of the V and W axes, D4: the measured depth of the rectocele during maximal straining, RVS: Rectova- ginal septum.
Fig. 8. Rectal intussusceptions (A) Resting, (B) Straining. White arrow: intussusception.
결 론
회음부초음파 검사를 시행함으로써 배변장애나 골반저 질환이 의심되는 환자에서 골반 구조물의 움직임이나 변 화를 직접 관찰하는 것이 가능하고, 이것을 환자에게 직접 보여주면서 질환에 대하여 설명할 수 있다는 점은, 모호한 증상의 호소 혹은 충분하지 못한 검사로 인해서 올바른 진 단에 적절히 이르지 못하는 문제점들을 해결할 수 있고, 진료 및 치료 시에 환자와의 관계에 큰 신뢰를 형성할 수
있으며 치료 시 환자의 적극적인 동참을 유도할 수 있고, 이는 치료 후의 결과 및 환자의 만족감에도 좋은 영향을 미칠 수 있다고 생각된다. 회음부초음파 검사는 검사방법 이 어렵지 않으며 방사선 노출의 위험이 없고 고가의 장비 나 시설이 필요하지도 않으며 일반적인 2D초음파 장비를 이용하기 때문에 비용적인 문제나 검사의 편의성에 있어 서도 장점이 있으므로 변실금이나 배변장애, 골반저 질환 에 대한 진료영역에서 적극적으로 시행해 볼 수 있는 검사 방법이라고 생각한다. 하지만 회음부 검사로 인해서 환자
명하고 동의를 얻어야 할 것이며, 검사 중 반드시 간호사 를 동반함으로써 만일에 생길 수 있는 불미스러운 문제점 들에 대한 주의도 필요하다.
REFERENCES
1. Maglinte DD, Kelvin FM, Fitzgerald K, Hale DS, Benson JT. Association of compartment defects in pelvic floor dysfunction. AJR Am J Roentgenol 1999;172:439-44.
2. Goei R, Kemerink G. Radiation dose in defecography.
Radiology 1990;176:137-9.
3. Kruger J, Heap X, Dietz HP. OC259: a comparison of magnetic resonance imaging and 4D ultrasound in the assessment of the levator hiatus. Ultrasound Obstet Gynecol 2007;30:A447.
4. Beer-Gabel M, Teshler M, Barzilai N, Lurie Y, Malnick S, Bass D, et al. Dynamic transperineal ultrasound in the diagnosis of pelvic floor disorders: pilot study.
Dis Colon Rectum 2002;45:239-45; discussion 245-8.
5. Brusciano L, Limongelli P, Pescatori M, Napolitano V, Gagliardi G, Maffettone V, et al. Ultrasonographic patterns in patients with obstructed defaecation. Int J
7. Pescatori M, Regadas FSP, Regadas SMM, Zbar AP.
Imaging Atlas of the Pelvic Floor and Anorectal Diseases. Milano: Springer-Verlag; 2008.
8. Beer-Gabel M, Frudinger A, Zbar A. Dynamic trans- perineal ultrasound and transvaginal sonography. In:
Wexner SD, Zbar AP, Pescatori M, editors. Complex anorectal disorders: investigation and management.
London: Springer; 2005. pp.246-58.
9. Kleinübing H Jr, Jannini JF, Malafaia O, Brenner S, Pinho TM. Transperineal ultrasonography: new method to image the anorectal region. Dis Colon Rectum 2000;43:1572-4.
10. Roche B, Deléaval J, Fransioli A, Marti MC. Compari- son of transanal and external perineal ultrasono- graphy. Eur Radiol 2001;11:1165-70.
11. Piloni V. Dynamic imaging of pelvic floor with trans- perineal sonography. Tech Coloproctol 2001;5:103-5.
12. Santoro GA, Wieczorek AP, Dietz HP, Mellgren A, Sultan AH, Shobeiri SA, et al. State of the art: an in- tegrated approach to pelvic floor ultrasonography.
Ultrasound Obstet Gynecol 2011;37:381-96.
13. Dietz HP. Pelvic floor ultrasound: a review. Am J Obstet Gynecol 2010;202:321-34.