44
서 론화상에 의한 신체의 변형은 원상복귀가 사실상
어려우며 가능한 기능적인 측면을 먼저 고려하고 이후에 미용적인 측면을 고려하게 된다. 유방은 여 성에게 매우 중요한 구조물인 것은 당연하고 사춘 기에 발달하기 시작하여 특히 그 이전에 손상된 가슴은 유방의 발달을 저해한다. 이에 대한 보고는 실제의 환자에 비해 많지 않으며 중증도의 변형에 대한 재건만을 보고한 경우는 없고 일반적인 치료 원칙에 대한 보고나,1) 유륜유두의 재건,2) 그리고
화상유방의 교정
서울대학교 의과대학 성형외과
이 윤 호․권 성 택
Treatment of Burned Breast
Yoonho Lee, M.D., Ph.D. and Sungtack Kwon, M.D., Ph.D.
Department of Plastic Surgery, Seoul National University Hospital, Seoul, Korea
Backgrounds: Disfigurements resulted from burn are not restored easily due to the original deficiency of tissues. Because the breasts have three dimensional structure, more tissue is required to reconstruct them. Even with the physiologic development the burned breasts can be distorted toward at any direction and became more serious disfigured than any other structures.
Methods and Results: We treated severely deformed burned breasts of nine patients from 1991 to 2000. Deformities are divided into three types related to the steps of evaulation and planning of treatment progress; Type I-mid-sternal, Type II-peripheral, Type III-parenchymal deficient and type IV-nipple areolar. In order of type breasts were released by skin graft and tissue expander.
Musculocutanous flaps were employed to replace the deficiency in type III deformity usually after the correction of type I and II deformity in the complicated cases. In type IV deformity, the methods of reconstruction of nipple-areolar complex were individualized related to the status usually after the correction of the former typed disfigurements.
Conclusions: In our experiences, the burned breasts were to be examined carefully to determine the direction and the location of the contracture, not weighing no much on the scar itself. Release of the contracture along with the anatomical units resulted from the embryological development would promise reasonable results along with the methods of every possible ways.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Breast, Burn, Contracture
책임저자:이윤호, 서울시 종로구 연건동 28번지 우편번호: 110-744, 서울대학교병원 성형외과 Tel: 02-760-2374, Fax: 02-742-3821
E-mail: [email protected]
조직확장기를 이용한 보고3) 등이 10년 전을 끝으 로 있었다. 저자들도 실제로는 적지 않은 흉부에 화상을 입은 환자들을 많이 있어왔지만 단순한 반 흔이 있는 환자들과 유방자체의 구축이 아닌 액와 부 등의 구축으로 인한 유방의 변형이 있는 환자 들은 제외하고 1990년부터 2000년까지 11예의 화 상으로 인해 변형된 유방을 교정하면서 유방의 형 태를 재건하였는데 실제로 수술 전에 보이는 상태 보다 유방의 해부학적 위치와 발생학적인 점을 고 려한 유형에 따른 단계적 수술로 만족할만한 결과 를 얻었다.
대상 및 방법
저자들은 1995년부터 2000년까지 화상변형 유방 을 가진 11명의 환자를 치료하였다.
적은 수의 환자지만 그 치료의 방침에 따라 4가
지 유형으로 나누었다(Table 1).
제1형은 정중형으로 그 구축의 중심이 sternum을 향하여 있는 경우이고 제2형은 외측형으로 제3형 은 결손형으로 구축자체의 원인도 있겠지만 근본 적으로 화상으로 인하여 유방조직의 결손이 심하 여 피부이식이나 조직확장 등만으로는 구축의 이 완만으로는 해결되지 않아 원거리에서 조직을 옮 겨 보충을 해야 하는 경우이다. 제4형은 유륜-유두 의 파괴로 이에 대한 재건이 필요한 경우로 순수 하게 유륜-유두만의 재건이 필요한 경우는 물론 제1, 2, 3형의 화상유방의 치료가 끝난 후 유륜-유 두의 재건이 남아 있는 상태를 포함할 수 있다. 제 1형은 정중부의 흉골을 따라 구축을 이완시켜 유 방조직이 외측으로 움직이게 하였고(Fig. 1), 제2형 은 재건해야 할 부위에 조직을 보충하는 것으로 제일 목표부위는 inframammary crease로 이 부위가 정상적인 상태가 되도록 필요한 조처를 취한다. 대
Table 1. Types of Burned Breasts and the Description
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Types
Description ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Type I Type II Type III Type IV
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Location of main problem Midline Infra-/lateral Parenchymal deficiency Nipple-areolar
No. of patients 2 6 2 1 (7)*
Main treatment modalities Skin graft Skin graft and Musculocutaneous flap Graft from various sites tissue expansion including the opposit breast ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
*numbers including the patients from other types
Fig. 1. Case of Type I burned breast. Left, preoperative status. Right, status of 1 year after operation.
부분의 경우(4예) 주위에 조직확장기를 이용하여 inframammary fold로 피판을 넣어주었고(Fig. 2),순 수하게 피부이식만을 한 경우도 2예가 있었다(Fig.
3). 제3형은 등배부에서 활배근피판을 이용하여 필 요한 위치에 이전시켰다(2예, Fig. 4). 제4형은 따로
환자를 가지고 있는 경우는 물론 다른 형의 환자 들 중에서 원래의 문제를 해결하고 난 후 유륜-유 두가 없는 경우가 포함되며 일반적인 방법으로 피 부이식과 earlobe의 복합조직이식은 물론 다른 편 의 유륜을 축소 절제하여 이를 이용하기도 하였다
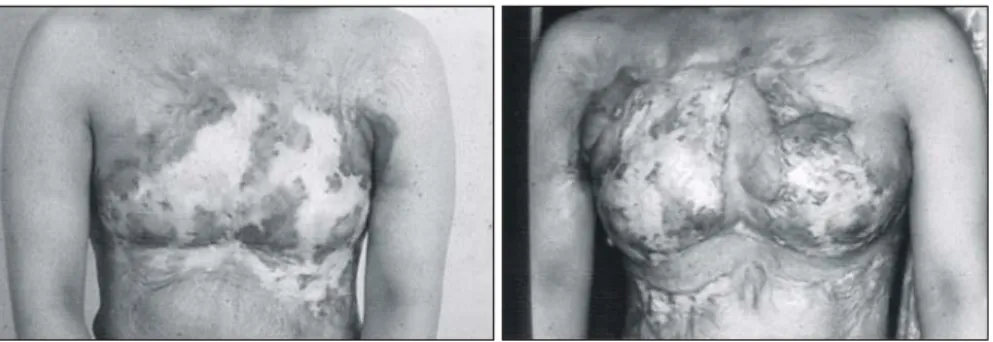
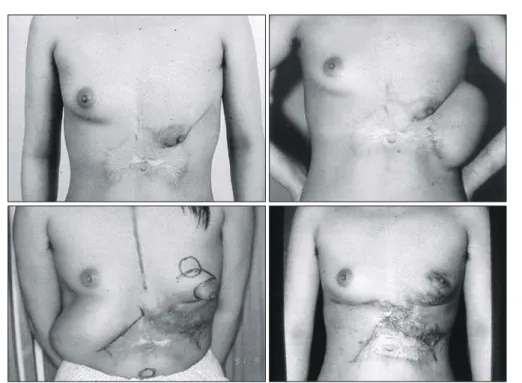
Fig. 2. Case of Type II burned breast. Staged tissue expansion was employed for exact match with the location and shape of opposit breast. Above left, preoperative status. Above right, status of tissue expansion for the release of lateral contracture and inframammary fold. Below left, status of next tissue expansion for the release of medial contracture and inframammary fold. Below right, status of 8 months after operation.
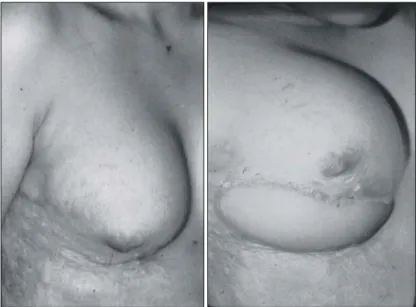
Fig. 3. Case of Type II burned breast. Simple skin graft was done for inframammary fold reconstruction and
nipple-areolar reconstruction. Left, preoperative status. Right, status of 6 months after operation.
(Fig. 5).
결 과
수술 후 6개월에서 3년까지 추적하였으며 모든 환자에서 결과에 만족하였다.
수술 전 유방조직이 전혀 발달하지 못하였을 것 으로 기대되었던 제1형의 경우에 해부학적인 구조 를 따라 구축을 이완하였을 때 유방조직이 마치 흉각안에 숨어 있다가 솟아 나오듯이 발육하기도
하였고(Fig. 1), 심하게 한쪽으로 변형되었던 경우 에도 inframammary crease를 재건하면 유방의 형태 가 이루어졌다(Fig. 2). Inframammary fold를 피부이 식만으로 만들어 유반조직을 상향과 전방으로 이 완시킨 경우도 유방의 입체적 구조가 많이 개선되 었다(Fig. 3). 제3형의 경우 활배근피판은 그 필요 한 양과 위치의 조절이 용의하였다(Fig. 4). 유륜- 유두의 재건은 고식적인 방법으로 개선이 가능하 였다(Fig. 5).
Fig. 5. Case of Type IV burned breast. Areolar skin from opposit breast were grafted. Left, preoperative status. Right, status of 2 years after operation.
Fig. 4. Case of Type III burned breast. Lattisimus dorsi musculocutanous flap was transferred. Left,
preoperative status. Right, status of 1 year after operation.
고 찰
신체의 어느 부위도 화상의 예외가 되는 곳은 없다. 흉부의 화상은 대개의 경우 중증 이상의 화 상을 입었을 때에 특히 여성에게 치명적인 외형장 해를 일으킨다.
유방의 모양은 신체 다른 부위보다도 특히 3차 원적 구조를 가지고 있고 사춘기에 발달을 하므로 그 이전에 화상을 입은 여아에 있어서는 그 발육 의 미숙을 초래하게 된다.
화상에 대한 연구는 전세계적으로 많이 이루어 져 있으나 연구에 대한 투자가 병태생리와 창상치 유 등의 기초연구에 주로 집중되어 있고 특히 체 간부에 생긴 장해는 이후로 주목받을 만한 치료법 에 대한 발표가 최근에는 미비하다. 저자들은 단지 조직의 파괴에 의한 결손만으로 기초한 것이 아니 고 환자를 평가할 때의 중점적으로 이학적 검사를 하는 순서와 구축을 해결해 나가는 부위별의 순서 와도 일치하는 즉 평가와 치료의 계획을 세우는 방침과 합치하는 분류이다. 유방의 발달은 발생학 적으로 양측에서 유성을 따라 내려오므로 유방조 직은 흉골을 중심으로한 양측의 조직이 먼저 확보 되어야 하고 제4, 5늑골간에서 정지하면서 전방으 로 발육하는 데 이때 복부의 피판과 유방조직은
그 전환되는 부위로 inframammary fold가 생기는 것이다. 그러므로 보통의 유방의 재건에서처럼 유 방의 mound의 형체는 흉부의 중심부와 inframam- mary fold가 확보된 연 후에 고려해야 하며 화상에 서와 같이 그 손상이 광범위할수록 실제 그 형태 의 변형이 어디에서 기인하는 가를 냉철히 판단하 고 제3형의 경우로 판단 될 때는 제1, 2형의 요소 를 확실히 제외할 수 있었는가를 짚고 넘어가야 할 것이다.
저자들은 화상으로 인한 유방변형을 재건함에 있어 그 발생학적인 면을 고려하고 치료의 순서에 입각하여 환자를 분류하고 각각의 유형 및 그 단 계에 맞는 치료를 하여 만족할만한 결과를 얻어 이에 보고하는 바이다.
참 고 문 헌