대한소화기학회지 2005;45:365-368
INTRODUCTION
Shiga toxin producingEscherichia coli(STEC) is a type of enterohemorrhagicE. coli(EHEC) that can cause illness rang- ing from mild watery diarrhea to severe hemorrhagic colitis fol- lowed by hemolytic uremic syndrome (HUS) in 10-15% of pediatric patients.1
Most outbreaks have been linked to O157:H7 strain, although more than 100 other non-O157:H7 strains such as O111 and O26 have been implicated. STEC associated HUS is the most common cause of renal failure on childhood in Western coun- tries,2but it has been a relatively rare disease in Korea. Fur-
thermore, there is no report about HUS with hemorrhagic colitis caused by STEC of non-O157:H7 strains such as O111 and O26 in adult. We herein report a case of HUS with hemor- rhagic colitis caused by STEC O111 in adult.
CASE REPORT
A 51-year-old woman came to our hospital due to bloody diarrhea and abdominal pain that suddenly occurred 3 days ago.
She had no specific past medical, personal and family history.
She denied a history of eating hamburger or undercooked meats. She and her family have been drinking purified water.
Escherichia coli O111 감염에 의한 용혈 요독증이 동반된 출혈 대장염 예 1
한양대학교 의과대학 내과학교실 구리병원,
김종표․한동수․백창희․정용우․김진배․손주현․함준수
A Case of Hemolytic Uremic Syndrome with Hemorrhagic Colitis due to Escherichia coli O111 Infection
Jong Pyo Kim, M.D., Dong Soo Han, M.D., Chang Hee Paik, M.D., Yong Woo Chung, M.D., Jin Bae Kim, M.D.,
Joo Hyun Sohn, M.D. and Joon Soo Hahm, M.D.
Department of Internal Medicine, Hanyang University College of Medicine, Guri, Korea
Shiga toxin producing E. coli (STEC) may cause severe hemorrhagic colitis followed by hemolytic uremic syn- drome (HUS). In Korea, there had been a few case reports of HUS by STEC, mostly due to O157 serotype. The reports of HUS caused by STEC non-O157 serotype were rare. We report a sporadic case of HUS associated with hemorrhagic colitis. A 51-year-old woman was admitted to our hospital due to intractable abdominal pain and bloody diarrhea. Three days after admission, azotemia and microangiopathic hemolysis developed. E. coli, serotype O111 was identified. Conservative management with plasmapheresis resulted in a complete recovery.
(Korean J Gastroenterol 2005;45:365-368)
Key Words: Escherichia coli infection; Hemolytic uremic syndrome
접수: 2004년 11월 5 ,일 승인: 2005년 2월 15일 연락처 한동수: , 471-701, 경기도 구리시 교문동 249-1
한양대학교 구리병원 내과학교실
Tel: (031) 560-2226, Fax: (031) 031-555-2998 E-mail: [email protected]
Correspondence to: Dong Soo Han, M.D.
Department of Internal Medicine, Hanyang University Guri Hospi- tal, 249-1 Gyomun-dong, Guri-si, Gyeonggi-do 471-701, Korea Tel: +82-31-560-2226, Fax: +82-31-555-2998
E-mail: [email protected]
366 대한소화기학회지 제: 45권 제 호5 , 2005
She had no recent travel history. Three days ago, she visited a community hospital because of abdominal pain and watery diarrhea after meals. She was treated with intravenous fluids and antibiotics, but watery diarrhea changed to bloody in nature on the next day.
On admission, her blood pressure was 150/100 mmHg, body temperature 36.2oC, pulse rate 82/min, and respiration rate 20/min. On physical examination, she appeared acutely ill. No abnormalities were noted on head and neck, chest examination.
Abdominal examination showed distended abdomen with in- creased bowel sounds. There was diffuse, mild tenderness without rebound tenderness in whole abdomen. There was no organomegaly or palpable mass. Rectal examination revealed bloody stool. On laboratory examination, leukocyte count was 16,000/mm3, hemoglobin 11.2 g/dL, platelet count 259,000/mm3. Serum electrolytes and biochemistries were within normal range.
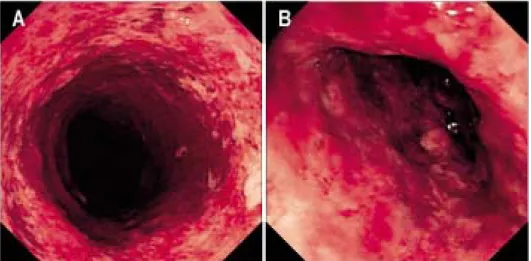
Sigmoidoscopy revealed diffuse and severe mucosal edema and hemorrhage with superficial ulcerations from descending colon to proximal sigmoid colon (Fig. 1). Multiple aphthous lesions were noted from distal sigmoid colon to rectum. Histopa- thologic examination revealed acute hemorrhagic colitis with inflammatory cell infiltration and fibrinoid exudates (Fig. 2).
On the third hospital day, oliguria and azotemia developed.
Laboratory examination revealed hemoglobin 9.0 g/dL, platelet count 36,000/mm3, total bilirubin 3.6 mg/dL, LDH 2,745 U/L, reticulocyte count 4.7%, BUN 51 mg/dL and creatinine 1.3 mg/dL. On peripheral blood smear, schistocytes were noted suggesting microangiopathic hemolytic anemia (Fig. 3). Sor- bitol-positiveE. coliwere isolated from her stool, which were ultimately confirmed asE. coli, serotype O111 by latex aggluti- nation test forE. coliO antigen. HUS caused by EHEC was
Fig. 1. Sigmoidoscopic findings.
Diffuse hemorrhagic ulcerative lesions were noted from des- cending colon (A) to proximal sigmoid colon (B).
Fig. 2. Histopathologic finding of descending colon. Microsco- pically ulcerative lesion with necrotic debris was noted. Severe necrotic change with interstitial inflammatory cells infiltration and fibrinoid exudates were noted. Mucosal glandular structures were relatively well preserved (H&E stain, ×40).
Fig. 3. Microscopic finding of peripheral blood smear. Thrombo- cytopenia and schistocytes were noted (Wright stain, ×1,000).
김종표 외 인 용혈 요독증을 동반한 출혈 대장염6 . 367
clinically diagnosed. Plasmapheresis and hemodialysis with con- servative managements were performed. The patient was com- pletely recovered without any complication after 2 weeks.
DISCUSSION
We report a rare case of HUS associated with hemorrhagic colitis by EHEC serotype O111 infection in adult. Hundreds of E. coliserotypes and at least six types ofE. coliintestinal pa- thogens have been recognized. Their virulence factors including toxin production, adherence to epithelial cell, and invasiveness are encoded by specific genetic elements (plasmids or chromo- somal genes) that determine pathogenicity.
Initial symptoms of EHEC infections usually begin with watery diarrhea, which last 1-2 days with abdominal cramping, followed by bloody diarrhea in 95% cases. Only 5% of cases will progress HUS with predilection for those less than five years of age and elderly patients.
EHEC prototype is O157:H7. The hallmark for this group is the production of Shiga toxins, a family of cytotoxins mediating the clinical manifestation of HUS, hemorrhagic colitis, and thrombotic thrombocytopenic purpura.3EHEC is also known as STEC.E. coliO157:H7 is the worldwide serotype of STEC and most commonly isolated from HUS patients in a series of outbreaks within North America, Japan, and the British Isles.2 Recently many epidemiologic studies in the area of other than these countries revealed that non-O157:H7 STEC may be underestimated as causative organisms of HUS by STEC.4-7 Furthermore, there have been some reports of STEC O111:H8 outbreaks in US, which previously known to be rare.8,9These findings suggested that suspected specimens of non-O157:H7 STEC should routinely be tested for serotyping and Shiga toxin assay.10
In Korea, there have been some cases of sporadic EHEC infections with or without HUS. According to the literatures about EHEC infections, non-O157:H7 STEC is a significantly important causative organism in hemorrhagic colitis associated with HUS in Korea. The revealed non-O157:H7 STEC serotypes areE. coliO8, O26, O111:H21, O114 and O171.11-14 But, the exact incidence and prevalence of EHEC infections in Korea have been suggested to be underestimated. The limited capability of many laboratories to identify Shiga toxins or other virulence factors may be the main cause of underestimation.
Culture ofE. coliO157:H7 from stool by sorbitol-Mac- Conkey agar medium is a good screening method.2But STEC
other than serotype O157:H7 shows mostly sorbitol-positive colonies, and therefore the sorbitol-MacConkey medium alone is not useful for their identification. Identification of non- O157:H7 STEC requires more detailed tests such as PCR or immunologic techniques to reveal the producing capability of Shiga toxins 1 and 2, intimin and enterohemolysin.6,15But such diagnostic approach is not popularly performed in our clinical settings because of its extensive costs and efforts. In the present case, the diagnosis of HUS caused by non-O157:H7E. coliwas made by biochemical and microbiologic tests including screen- ing test for STEC by sorbitol-MacConkey agar and stool cul- ture and confirmatory latex agglutination test forE. coliO antigen. ELISA and indirect hemagglutination assay have been used to detect the antibodies against lipopolysaccharide ofE.
coli. The immunosorbent assay to detect antibodies against O157:H7 has a sensitivity of 75% and a specificity of 92%.16 Antibodies to serogroups O26, O103, O111, O128 and O55 have been studied in patients with HUS with broad range of serological responses.
All patients with HUS must be hospitalized. Management should be mainly supportive and aimed to control the com- plications.17Antibiotics usually have no effect on the course of disease and may increase the risk of the HUS in children.18 Therefore, physician should be aware of it and wait for the stool culture. Therapeutic plasma exchange seems to decrease the mortality in adults with HUS but remain controversial.19In this case, azotemia was recovered by plasma exchange and dialysis.
Because we could not reveal the Shiga toxin production of O111 strain isolated from this patient, we suggest the pro- bability of HUS due to non-O157:H7 STEC. According to statistics of Korea Center for Disease Control and Prevention, 26 cases of STEC have been identified and 19 cases of them were non-O157:H7 STEC. The clinical importance of non- O157:H7 STEC has been underestimated and an epidemiologic study on the incidence of non-O157:H7 STEC associated with hemorrhagic colitis or HUS has not been well established in Korea. So the efforts to identify non-O157:H7 STEC serotype with sorbitol positive colonies may be helpful in case of acute infectious bloody diarrhea.
요 약
생성 대장균은 경미한 설사에서 심한 출혈 장 Shiga toxin
염에 합병되는 용혈 요독 증후군까지 다양한 임상상을 유발
368 The Korean Journal of Gastroenterology: Vol. 45, No. 5, 2005
할 수 있다 국내에서. Shiga toxin생성 대장균에 의한 용혈 요독 증후군이 드물지 않게 보고되나 대부분 대장균 O157:
이며 다른 혈청형의 생성 대장균에 의한 것은
H7 Shiga toxin
드물다. 51세 여자 환자가 하복부 동통과 혈성 설사를 주소
로 내원하여 내원 일째 급성 신부전과 미소혈관 혈3 소판감
소증이 발생하였다 대변 배양 검사에서 혈청형. O111의 대장
균을 동정하였고 보존 치료 및 혈장교환술을 시행한 후 환 자는 완전 회복되었다 저자들은 대장균. O157:H7이 아닌 대
장균O111에 의한 출혈 장염 및 이에 병발된 용혈 요독 증
후군 예를 경험해 보고한다1 .
REFERENCES
1. Hamer DH, Gorbach SL. Infectious diarrhea and food poiso- ning. In: Feldman M, Friedman LS, Sleisenger MH, eds. Gas- trointestinal and liver disease. Volume 2. 7th ed. Philadelphia:
Saunders, 2002:1871-1874.
2. Boyce TG, Swerdlow DL, Griffin PM.Escherichia coliO157:
H7 and the hemolytic-uremic syndrome. N Engl J Med 1995;
333:364-368.
3. Begue RE, Mehta DI, Blecker U.Escherichia coliand the hemolytic-uremic syndrome. South Med J 1998;91:798-804.
4. Kulkarni H, Goldwater PN, Martin A, Bettelheim KA.Escheri- chia coli‘O’ group serological responses and clinical cor- relations in epidemic HUS patients. Comp Immunol Microbiol Infect Dis 2002;25:249-268.
5. Elliott EJ, Robins-Browne RM, O'Loughlin EV, et al. Nation- wide study of haemolytic uraemic syndrome: clinical, micro- biological, and epidemiological features. Arch Dis Child 2001;
85:125-131.
6. Blanco JE, Blanco M, Alonso MP, et al. Serotypes, virulence genes, and intimin types of Shiga toxin (verotoxin)-producing Escherichia coliisolates from human patients: prevalence in Lugo, Spain, from 1992 through 1999. J Clin Microbiol 2004;
42:311-319.
7. Gerber A, Karch H, Allerberger F, Verweyen HM, Zimmer- hackl LB. Clinical course and the role of Shiga toxin- producingEscherichia coliinfection in the hemolytic-uremic syndrome in pediatric patients, 1997-2000, in Germany and Austria: a prospective study. J Infect Dis 2002;186:493-500.
8. [No authors listed]Escherichia coliO111:H8 outbreak among
teenage campers--Texas, 1999. MMWR Morb Mortal Wkly Rep 2000;49:321-324.
9. Brooks JT, Bergmire-Sweat D, Kennedy M, et al. Outbreak of Shiga toxin-producingEscherichia coliO111:H8 infections among attendees of a high school cheerleading camp. Clin Infect Dis 2004;38:190-198.
10. Park CH, Kim HJ, Hixon DL. Importance of testing stool specimens for Shiga toxins. J Clin Microbiol 2002;40:3542- 3543.
11. Lee JE, Kim SY. Clinical features of hemolytic uremic syn- drome in children. Korean J Pediatr Soc 2000;43:1473-1479.
12. Cho YH, Park HJ, Song KS, Song YG, Lee SI, Park IS. A case of hemolytic uremic syndrome caused byEscherichia coli O8: case report. Korean J Gastrointest Endosc 2002;25:213- 216.
13. Bae GR, Lee SW, Yang BG, et al. Cause of enterohemorrhagic Escherichia coliinfection in Ulju county, Korea. Korean J Prev Med 2003;36:77-84.
14. Ryu SJ, Hahn H, Yoo SJ, et al. Two cases of hemolytic uremic syndrome associated withEscherichia coliO114. J Korean Soc Pediatr Nephrol 2002;6:102-108.
15. Eklund M, Scheutz F, Siitonen A. Clinical isolates of non- O157 Shiga toxin-producingEscherichia coli: serotypes, viru- lence characteristics, and molecular profiles of strains of the same serotype. J Clin Microbiol 2001;39:2829-2834.
16. Barrett TJ, Green JH, Griffin PM, Pavia AT, Ostroff SM, Wachsmuth IK. Enzyme linked immunosorbent assays for detecting antibodies to Shiga like toxin 1, Shiga like toxin 2 andEscherichia coliO157:H7 lipopolysaccharide in human serum. Curr Microbiol 1991;23:189-195.
17. Bonnet R, Souweine B, Gauthier G, et al. Non-O157:H7 Stx2- producingEscherichia colistrains associated with sporadic cases of hemolytic-uremic syndrome in adults. J Clin Microbiol 1998;36:1777-1780.
18. Wong CS, Jelacic S, Habeeb RL, Watkins SL, Tarr PI. The risk of the hemolytic-uremic syndrome after antibiotic treat- ment ofEscherichia coliO157:H7 infections. N Engl J Med 2000;342:1930-1936.
19. Dundas S, Murphy J, Soutar RL, Jones GA, Hutchinson SJ, Todd WT. Effectiveness of therapeutic plasma exchange in the 1996 LanarkshireEscherichia coliO157:H7 outbreak. Lancet 1999;354:1327-1330.