Korean J Gastroenterol Vol. 71 No. 1, 45-48 https://doi.org/10.4166/kjg.2018.71.1.45 pISSN 1598-9992 eISSN 2233-6869
CASE REPORT
Korean J Gastroenterol, Vol. 71 No. 1, January 2018 www.kjg.or.kr
복강내로 파열된 가스 형성 화농성 간농양의 성공적인 내과적 치료 증례
이경진, 류수형
인제대학교 의과대학 서울백병원 내과
Ruptured Gas-forming Pyogenic Liver Abscess into the Peritoneal Cavity Treated Successfully with Medical Treatment
Kyung Jin Lee and Soo Hyung Ryu
Department of Internal Medicine, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea
Gas-forming pyogenic liver abscess (GFPLA) is very rare and has a very high mortality in case of rupture into the abdominal cavity, which usually require surgical treatment. We experienced a case of a ruptured GFPLA due to Klebsiella pneumoniae complicated with peritonitis and sepsis in a 68-year-old diabetic woman. Immediate and aggressive medical treatments including intravenous antibiotics, percutaneous drainage, and continuous renal replacement therapy dramatically improved the liver abscess, peritonitis, and metabolic problems. We report an unusual case of a ruptured GFPLA without surgical management, treated successfully with only medical treatment. (Korean J Gastroenterol 2018;70:45-48)
Key Words: Liver abscess, pyogenic; Rupture; Klebsiella pneumoniae; Peritonitis
Received October 27, 2017. Revised December 21, 2017. Accepted December 22, 2017.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2018. Korean Society of Gastroenterology.
교신저자: 류수형, 04551, 서울시 중구 마른내로 9, 인제대학교 의과대학 서울백병원 내과
Correspondence to: Soo Hyung Ryu, Department of Internal Medicine, Seoul Paik Hospital, Inje University College of Medicine, 9 Mareunnae-ro, Jung-gu, Seoul 04551, Korea. Tel: +82-2-2270-0012, Fax: +82-2-2279-4021, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
INTRODUCTION
Pyogenic liver abscess (PLA) is an uncommon disease with an annual incidence rate ranging from two to 45 cases per 100,000 hospital admissions worldwide.1 Gas-forming pyo- genic liver abscess (GFPLA) is even rarer, which accounts for 7% to 24% of PLA. When GFPLA is ruptured into the abdomi- nal cavity and causes peritonitis, which is much rarer and sur- gical treatment is required.2 Here, we present a very rare case of a ruptured GFPLA accompanied with peritonitis and septic shock, which was fully recovered with only medical treatment.
CASE REPORT
A 68-year-old woman visited our hospital with a five-day history of fever and abdominal pain. She had no remarkable medical history. On physical examination, blood pressure was 119/73 mmHg, body temperature was 38.4℃and heart rate was 145 beats/min. Tenderness on right upper quad- rant of abdomen was noted. Laboratory data revealed a he- moglobin of 13.1 g/dL, white blood cells count of 3.73×109/L, platelet count of 128,000/mm3, aspartate aminotransferase of 698 IU/L, alanine aminotransferase of 650 IU/L, total bilir- ubin of 1.3 mg/dL, albumin of 2.6 g/dL, prothrombin time of
46 이경진, 류수형. 파열된 가스 형성 간농양의 성공적 내과적 치료 증례
The Korean Journal of Gastroenterology
A B C
Fig. 1. CT scan of the abdomen. (A) CT scan of the abdomen shows a huge gas-forming abscess in the right lobe of the liver. (B) Contrast-en- hanced CT shows free air in the perihepatic space caused by ruptured gas-forming pyogenic liver abscess (arrowheads). (C) Follow-up abdomi- nal CT shows a significant decrease in the size of the abscess cavity and disappearance of air bubbles of extrahepatic sites. CT, computed tomography.
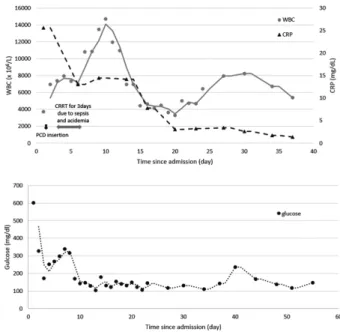
Fig. 2. The serial changes of serum levels of CRP, WBC and glucose during admission. CRP, C-reactive protein; WBC, white blood cells;
PCD, percutaneous catheter drainage; CRRT, continuous renal re- placement therapy.
14.1 sec (81%), and blood urea nitrogen of 23 mg/dL and cre- atinine of 1.3 mg/dL. Arterial blood gas analysis revealed pH 7.425, pCO2 25 mmHg, pO2 80.4 mmHg, HCO3 19.6 mEq/L, and O2 saturation 96.4%. Serological tests for hepatitis B and C were negative. The serum level of C-reactive protein was in- creased by 25.6 mg/dL (normal range, 0-0.8 mg/dL). Her se- rum glucose and HbA1c levels were 601 mg/dL and was 10.9%, respectively, which was consistent with diabetes mellitus. Abdominal contrast-enhanced computed tomog- raphy (CT) scan revealed a huge abscess with gas formation in the right lobe of the liver, which size was measured as 10 cm in diameter. In addition, free air and ascites were noted along right subphrenic area and right paracolic gutter due to leak- ing from hepatic abscess (Fig. 1A, B). These findings in- dicated rupture of gas-forming liver abscess into the peri- toneal cavity. Patient’s condition was not good for surgical treatment because of uncontrolled high serum glucose lev- els and sepsis state. We consider medical therapy first. The patient underwent ultrasound guided percutaneous cathe- ter drainage (PCD). Broad spectrum intravenous antibiotics (imipenem/cilastatin) and insulin treatment were started.
Later, Klebsiella pneumoniae was isolated from both periph- eral blood and drained bloody pus. Even though the best treatment, her condition deteriorated and progressed to met- abolic acidosis by sepsis (white blood cells count of 7.25×109/L, platelet count of 41,000/mm3, aspartate ami- notransferase 740 IU/L, alanine aminotransferase 610 IU/L, creatinine 1.08 mg/dL, arterial blood gas analysis revealed pH 7.25, pCO2 39.6 mmHg, pO2 89.4 mmHg, HCO3 17.8 mEq/L, and O2 saturation 95.4%). She underwent continuous renal
replacement therapy for three days. After the continuous re- nal replacement therapy, the acidemia and right upper quad- rant tenderness were improved. Intravenous antibiotics and PCD were maintained. Follow-up CT scan showed slowly de- creased abscess size and periheptic fluid collection.
Therefore, we kept PCD drainage. The drainage tube was re- moved 51 days after admission as the patient’s condition was improved and follow-up CT showed significant size re- duction of the abscess and diminished fluid collection of sub- phrenic, perihepatic, and paracolic gutter (Fig. 1C). Finally,
Lee KJ and Ryu SH, et al. Ruptured Gas-forming Pyogenic Liver Abscess Treated Successfully with Medical Treatment 47
Vol. 71 No. 1, January 2018
the patient was fully recovered and discharged with oral anti- biotics (Fig. 2).
DISCUSSION
GFPLA is less common, accounting for 7% to 24% of all PLAs.3 Most reports of GFPLA have come from Asia, most commonly associated organisms are the Klebsiella spp.3 A variety of microorganisms may be identified in older adults with PLA. In addition to Klebsiella pneumoniae, other causa- tive agents such as Escherichia coli and polymicrobial with or without anaerobic bacteria are frequently found in older adults.4,5 Cases of PLA with Clostridium perfringens are rare- ly reported.6,7
Diabetes mellitus, biliary stones, malignancy, liver cir- rhosis, and alcoholism are the risk factors for PLA in older adults.4 Younger individuals are more likely to be male and have alcoholism and cryptogenic etiology than older adults.
On admission, older adults have significantly less common right upper abdominal tenderness than younger individuals, resulting in delay in diagnosis.6,8 The patient had only uncon- trolled severe hyperglycemia caused by newly diagnosed dia- betes mellitus. High fever and right upper quadrant pain were obvious in this patient who was relatively old age.
Diagnosis can easily be made using radiological imaging such as sonography and CT. On ultrasonography, GFPLA pres- ent with diffuse hyperechoic spots with acoustic shadows, and CT reveals a low attenuation area with Hounsfield units similar to that of the lungs.9 Radiographs may show pockets of gas within the liver parenchyma, but this has been reported to be visible in only up to 36% of patients with GFPLA.3
The production of gas occurs as a result of mixed acid fer- mentation of glucose within the abscess. The mechanism in- volves fermentation by formic hydrogenlyase, an enzyme that is produced only in an acidic environment, when the local pH reaches 6 or less as a result of acid accumulation. Formic hy- drogenlyase converts formic acid accumulated within the ab- scess into carbon dioxide and hydrogen gas.3 It also been postulated that poor microcirculation in the affected areas contributes to gas accumulation, which may explain the high- er incidence of GFPLA in individuals with diabetes mellitus.10 GFPLA is a significant cause of morbidity and mortality, es- pecially in older adults with diabetes mellitus. To reduce mor- bidity and mortality, adequate antibiotics, such as ceftriax-
one with or without metronidazole, and good control of blood glucose with early adequate drainage are mandatory.11,12 Surgical drainage is performed in case of large and multi-lo- culated abscesses, ruptured abscesses, percutaneous drai- nage failure and critically ill patient with severe sepsis (high American Society of Anesthesiologists [ASA] score, low albu- min and hemoglobin).1,11,13 Because our patient exhibited a septic shock condition, we performed ultrasound-guided ab- scess drainage with the administration of intravenous antibiotics.
A case of successful non-surgical treatment of ruptured PLA has been reported recently.2 However, in case of rup- tured GFPLA into the peritoneal cavity, surgical treatment has known to be only treatment option.12,14 To the best of our knowledge, the present case may be the first report that rup- tured GFPLA accompanied with peritonitis and sepsis, which was fully recovered with only medical treatment.
REFERENCES
1. Johannsen EC, Sifri CD, Madoff LC. Pyogenic liver abscesses.
Infect Dis Clin North Am 2000;14:547-563, vii.
2. Motoyama T, Ogasawara S, Chiba T, et al. Successful non-surgi- cal treatment of ruptured pyogenic liver abscess. Intern Med 2013;52:2619-2622.
3. Lee HL, Lee HC, Guo HR, Ko WC, Chen KW. Clinical significance and mechanism of gas formation of pyogenic liver abscess due to Klebsiella pneumoniae. J Clin Microbiol 2004;42:2783-2785.
4. Pu SJ, Liu MS, Yeh TS. Pyogenic liver abscess in older patients:
comparison with younger patients. J Am Geriatr Soc 2010;58:
1216-1218.
5. Chen SC, Lee YT, Yen CH, et al. Pyogenic liver abscess in the eld- erly: clinical features, outcomes and prognostic factors. Age Ageing 2009;38:271-276.
6. Eltawansy SA, Merchant C, Atluri P, Dwivedi S. Multi-organ failure secondary to a Clostridium perfringens gaseous liver abscess following a self-limited episode of acute gastroenteritis. Am J Case Rep 2015;16:182-186.
7. Law ST, Lee MK. A middle-aged lady with a pyogenic liver abscess caused by Clostridium perfringens. World J Hepatol 2012;4:
252-255.
8. Chong VH, Yong AM, Wahab AY. Gas-forming pyogenic liver abscess. Singapore Med J 2008;49:e123-e125.
9. Yang CC, Chen CY, Lin XZ, Chang TT, Shin JS, Lin CY. Pyogenic liver abscess in Taiwan: emphasis on gas-forming liver abscess in diabetics. Am J Gastroenterol 1993;88:1911-1915.
10. Chou FF, Sheen-Chen SM, Chen YS, Lee TY. The comparison of clinical course and results of treatment between gas-forming and non-gas-forming pyogenic liver abscess. Arch Surg 1995;130:401-405; discussion 406.
48 이경진, 류수형. 파열된 가스 형성 간농양의 성공적 내과적 치료 증례
The Korean Journal of Gastroenterology 11. Ho MP, Chou AH, Cheung WK. Gas-forming pyogenic liver abscess
in an elderly adult with diabetes mellitus. J Am Geriatr Soc 2013;61:837-838.
12. Shiba H, Aoki H, Misawa T, Kobayashi S, Saito R, Yanaga K.
Pneumoperitoneum caused by ruptured gas-containing liver abscess. J Hepatobiliary Pancreat Surg 2007;14:210-211.
13. Alkofer B, Dufay C, Parienti JJ, Lepennec V, Dargere S, Chiche L.
Are pyogenic liver abscesses still a surgical concern? A Western experience. HPB Surg 2012;2012:316013.
14. Jun CH, Yoon JH, Wi JW, et al. Risk factors and clinical outcomes for spontaneous rupture of pyogenic liver abscess. J Dig Dis 2015;16:31-36.