Willis환 내 뇌동맥류 진단시 전산화단층촬영 뇌혈관 조영술의 유용성
대구파티마병원 신경외과
이혁기·조재훈·이성락·강동기·김상철
= Abstract =
Usefulness of Computed Tomographic Angiography in the Detection and Evaluation of Aneurysms of the Circle of Willis
Hyuk Gi Lee, M.D., Jae Hoon Cho, M.D., Sung Lak Lee, M.D., Dong Gee Kang, M.D., Sang Chul Kim, M.D.
Department of Neurosurgery, Fatima Hospital, Taegu, Korea
bjective:The purpose of this study was to compare computed tomographic angiography(CTA) with conven- tional cerebral angiography(CCA) and to assess usefulness of CTA in detection and anatomic definition of intracranial aneurysms of the circle of Willis in subarachnoid hemorrhage.
Patients and Methods : Fifty consecutive patients with known or suspected intracranial saccular aneurysms underwent CTA with preoperative CCA from 1997 to 1999. Using surface shaded display post-processing technique, CTA was interpreted for the presence, location of aneurysms and anatomic features. The image obtained with CTA was then compared with CCA image.
Results:In 47 patients, CCA revealed 57 cerebral aneurysms and CTA revealed 54 aneurysms. Two of the 57 cerebral aneurysms were located outside of the imaging volume of CTA and one case was misdiagnosed. The sensitivity of CTA was 94.7% and the specificity was 100%. The results obtained with CTA were, compared with the results obtained with CCA, equal in determining dome shape, direction and lobularity. However, CTA provided a 3- dimensional representation of aneurysmal lesion very useful for surgical planning. Moreover, CTA was useful for rapid and relatively noninvasive detection of aneurysms in the circle of Willis.
Conclusion:CTA can be a diagnostic tool for the patients with acute subarachnoid hemorrhage due to a ruptured aneurysm of the circle of Willis and provides adequate anatomic detail for surgical planning, especially to complex cerebral aneurysms. However, we think CCA is necessary because of CTA limitations including its difficulty in detec- ting unusually located aneurysms(including those in cavernous sinus or distal artery) and combined vascular lesion (including arteriovenous malformation) and acquiring dynamic flow information.
KEY WORDS:Computed tomographic angiography・Conventional cerebral angiography・Intracranial aneurysms・
Circle of Willis.
서 론
뇌동맥류 파열에 의한 뇌지주막하출혈은 높은 사망률과 이환율을 보이므로
19)21)뇌동맥류의 조기진단과, 재파열에 의한 합병증을 줄이기 위한 조기치료가 필요하다
2). 현재까
지 널리 사용되는 고식적 뇌혈관조영술(conventional ce- rebral angiography, CCA)은 환자가 불안정할 때는 시행 하기 어렵고, 검사에 많은 시간이 요구될 뿐 아니라, 침습적 인 검사방법이며 0.1~2.6%에서 중추신경계 합병증을 유발 한다. 특히, 뇌지주막하출혈 후 CCA를 6시간 내에 시행할 때 재출혈의 가능성이 증가하여 조기검사방법으로 어려운
OOOO
점이 있다
10). 전산화단층촬영 혈관조영술(computed tom- ographic angiography, CTA)은 검사시간이 짧고, 전산화 단층촬영(CT)을 할 때 바로 시행할 수 있으며, 선택적 뇌 혈관도관술을 할 필요가 없으므로 중추신경계의 손상이 적 어 뇌지주막하출혈의 급성기 및 파열 전 진단에 매우 유용 하다
6). 또한, 두개강 내 동맥구조의 3차원적 영상을 제공하 여 해부학적 구조인식에 도움이 된다
8). 저자들은 뇌동맥류 의 진단에 있어 CTA와 CCA를 비교하여 CTA의 선별검사
로의 가능성과 해부학적 인식에 대한 유용성에 대해 문헌
고찰과 함께 보고한다.
대상 및 방법
본 연구는 1997년 10월에서 1999년 2월까지 갑자기 발생한 의식소실, 두통, 구토 등의 증상으로 뇌동맥류파열이 의심되었던 환자 중 CCA와 CTA를 모두 시행한 50명을 대 상으로 하였다. CCA는 SIREGRAPH D2(Siemens, Mu- enchen, Germany)로 cut-film방법으로 시행하였다. 나선 형 CT로 SOMATOM PLUS 4(Siemens, Muenchen, Ger- many)를 이용하였고, 수용성 조영제인 Omnipaque(300 mgI/l isohexol, Nycomed, Cork, Ireland)를 주입펌프를 이용하여 말초정맥으로 초당 4ml의 속도로 140ml를 주입 하였다. 촬영은 조영제의 주입 15초 후부터 시작하여 터키 안 상연으로부터 35mm 상방까지 1mm 간격, 1mm/sec.
촬영속도로 촬영하고, 0.5mm 절편으로 재구성하여 횡단기 초영상을 얻었다. 영상의 재구성은 Sienet Magicview 1000 을 이용하여 120~2000HU(Hounsfield unit)에서 surface shaded display(SSD)방법으로 시행하였다. 3차원적 영상 재구성 후 주위의 골조직 및 불필요한 잔여구조물을 제거하였 고, Willis환 내 동맥구조를 확인하기 위하여 영상을 360°임
Table 1. Angiographic and surgical findings
Category No. in study
Patients 50
Patients in CTA(-) 2 Patients with aneurysms 47
1 aneurysm 39
2 aneurysms 4
3 aneurysms 2
1 aneurysm and 1 AVM 1
3 aneurysms and 1 AVM 1 Patients with AVM 1 Total number of aneurysms 57 CTA:computed tomographic angiog
AVM:arteriovenous malformation
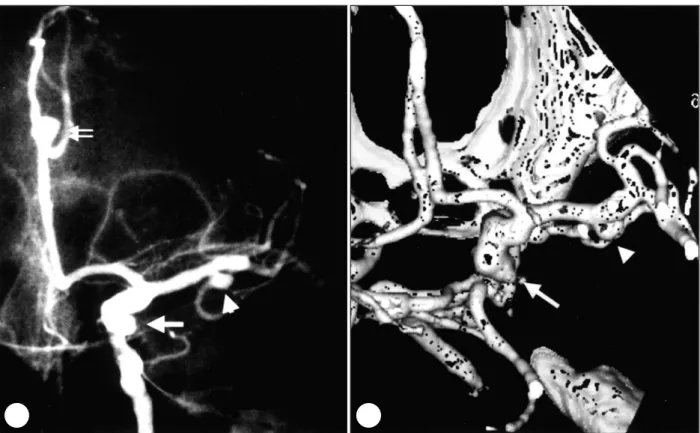
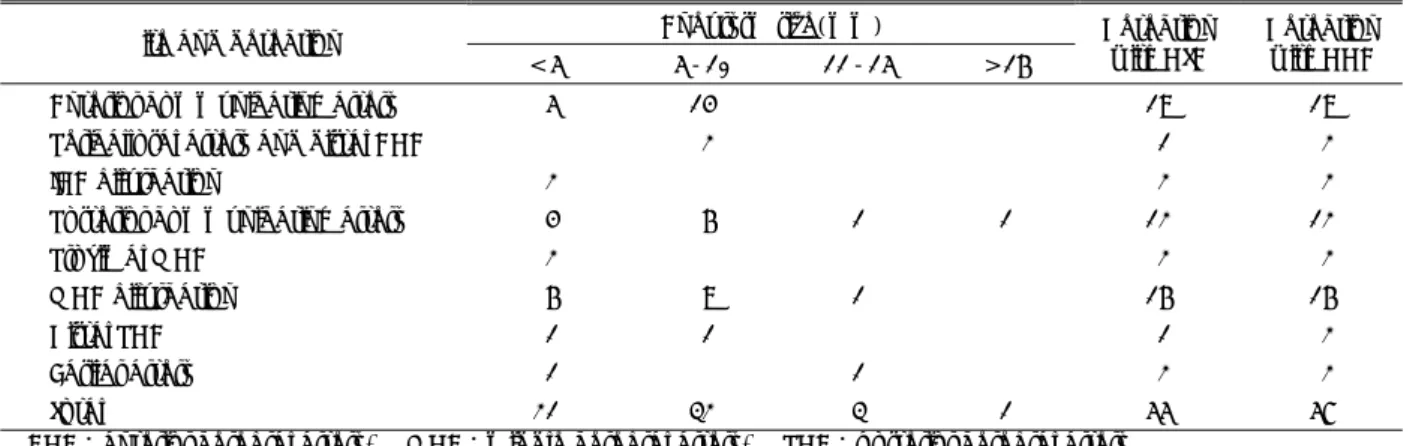
Fig. 1. A:Left internal carotid angiogram showing multiple aneurysms located in posterior communicating artery(arrow- head), middle cerebral artery(arrow) and pericallosal artery bifurcation(double arrow). B:Pericallosal artery bifurcation aneurysm is not found in CTA.
A A A
A B B B B
의로 돌려보았다. 3명 이상의 신경외과 전문의가 영상으로 확인된 뇌동맥류 각각에서 발생부위, 방향, 동맥류의 분엽 및 경부의 유무를 판독하였고, 이를 CCA의 소견과 비교하 여 동일성 검증법(quisquare test)으로 검증하였다.
결 과
뇌동맥류파열이 의심되어 CCA와 CTA를 모두 시행한 50 명에서 성비는 남자가 17명, 여자가 33명이었고, 연령 분포는 25~79세였으며 평균연령은 55.4세였다. CT촬영 상 46 명에서 뇌지주막하출혈이 있었으며, Fisher Grade
Ⅱ가 19명, Grade Ⅲ가 15명, Grade Ⅳ가 12명이었다.
CCA를 하기 전에 시행한 CTA로 46명에서 54개의 뇌동 맥류와 1개의 뇌동정맥기형이 발견되었으며, CCA로 47명 에서 57개의 뇌동맥류와 3개의 뇌동정맥기형이 발견되었고 그중 53개의 뇌동맥류가 수술로 확인되었다(Table 1).
CCA로 진단되었으나 CTA로 진단되지 않은 경우는 3례로, 2례는 뇌동맥류가 주사범위밖에 있었으며(Fig. 1), 1례는 CT촬영 상 혈종의 위치와 관계없는 곳에 생긴 미파열동맥 류로 판독할 때 간과되었다(Fig. 2).
뇌동맥류가 생긴 위치를 분류하면 57개 중 전교통동맥이 19개, 중뇌동맥이 18개로 가장 많았으며, 후교통동맥 12개,
Table 2. Aneurysm detection according to site and size
Aneurysm size(mm) Site and detection
< 5 5-10 11-15 > 16
Detection with CTA
Detection with CCA
Anterior communicating artery 5 14 19 19
Pericallosal artery and distal ACA 2 1 2
ICA bifurcation 2 2 2
Posterior communicating artery 4 6 1 1 12 12
Proximal MCA 2 2 2
MCA bifurcation 6 9 1 16 16
Distal PCA 1 1 1 2
Basilar artery 1 1 2 2
Total 21 32 3 1 55 57
ACA:anterior cerebral artery, MCA:middle cerebral artery, PCA:posterior cerebral artery CCA:conventional cerebral angiography, CTA:computed tomographic angiography
Fig. 2. A:CT showing right putaminal hematoma with some subarachnoid hemorrhage. B:CTA demonstrating a left laterally projecting anterior communicating artery aneurysm(arrow).
A A A
A B B B B
내경동맥 2개, 기저동맥 2개, 전뇌동맥 1개, 후뇌동맥 1개 와 주사범위밖에 위치하여 CTA로 진단할 수 없었던 원위 전뇌동맥 1개와 원위후뇌동맥 1개가 있었다. CTA로 뇌동 맥류의 직경은 측정하지 않았으나, CCA에서 뇌동맥류의 직 경은 3~20mm였고, 평균직경은 5.82mm였다(Table 2).
뇌동맥류의 특징인 동맥류의 발생부위, 경부의 유무와 분 엽의 유무, 방향 등을 구별할 수 있는지를 두 개의 검사법에 서 비교하여, CTA에서 경부와 분엽을 각각 43개, 20개 확 인할 수 있었으며, 동맥류의 방향은 모든 검사 예에서 확인 할 수 있었다. CTA 상 뇌동맥류의 특징은 CCA의 그것과 비교했을 때 유의할 만한 차이가 없었으며(Table 3), 오히 려 3차원적 영상을 임의로 돌려볼 수 있어 해부학적 구조를 더 잘 알 수 있었다(Fig. 3 A, B, C). 특히, 뇌동맥류 크기가 큰 경우, 동맥류 주위의 구조를 보는데 도움이 되었다(Fig.
3D).
의식이 좋지 않았던 1명의 환자에서 미치료동맥류의 추
적검사를 시행한 결과 뇌동맥류의 성장을 확인하였다(Fig.
4). 또 뇌동맥류-클립복합체를 가진 2명의 환자에서 CTA 를 시행한 결과 금속효과 때문에 잔여동맥류를 볼 수 없었 으나, 이것이 다른 부위에 생긴 뇌동맥류의 진단에는 영향 을 주지 않았다(Fig. 5).
고 찰
CCA는 뇌동맥류의 진단에 가장 많이 이용되는 방법이나, 환자의 의식이나 전신상태가 나쁠 때에는 시행하기 어렵고, 혈관의 선택적 도관술이 불가능한 경우가 있으며, 혈관패색 이나 혈관연축이 있는 경우 또는 작은 뇌동맥류 주위로 혈 관이 돌아가거나 겹쳐 있을 때 정확한 해부학적 구조를 보 는데 어려움이 있다. 또한 침습적 검사이므로 혈관의 자상, 뇌허혈, 국소혈종, 알러지, 고열, 패혈증 등의 합병증을 야기 할 수 있으며, 특히 뇌지주막하출혈 후 6시간이내에 검사를
Table 3. Characteristics of aneurysms
Aneurysm neck Aneurysm lobulation Aneurysm direction
Present Absent Mono- Multi- Absent Present Absent
CTA 43 11 10 10 34 54 0
CCA 47 10 9 11 37 57 0
CCA: conventional cerebral angiography, CTA: computed tomographic angiography No difference between two groups to aneurysmal neck and lobulation(χ
2=0.190<5.99, α=0.05)
Fig. 3. CCA and CTA showing various sites of aneurysms. A:Aneurysm of the anterior communicating artery(arrow). B:
Aneurysm of the middle cerebral artery(arrow). C:Aneurysm of the basilar artery(arrow). D:Large aneurysm of the posterior communicating artery(arrow).
A A A
A B B B B
C C C
C D D D D
시행할 경우 뇌동맥류 파열의 위험성이 증가하여 조기검사 에 어려운 점이 있다
10). 미세수술 및 혈관연축에 대한 연구 의 발전으로 뇌동맥류의 치료성적은 크게 향상되었지만 뇌 동맥류의 유병률 및 사망률은 변화가 없어 뇌동맥류의 파열 전 진단과 조기치료의 중요성이 제기되어
2)CCA 외에 정맥 내 혈관조영술, 자기공명 뇌혈관조영술 및 CTA가 시도되
었다
14)17)32). 그러나 정맥내 뇌혈관조영술은 부적절한 영상
과 많은 양의 조영제가 필요하여 사용하기 어려우며, 자기 공명 뇌혈관조영술은 검사시간이 길어, 환자의 상태가 나쁘 거나 비협조적인 경우에는 검사에 어려움이 있고, 운동허상 이 쉽게 생기는 문제점이 있다
3)17). CTA는 검사시간이 짧 고, 선택적 도관술에 따른 합병증의 위험성이 없어 응급환 자나 CCA를 시행할 수 없는 환자에 있어 CT촬영을 하면 서 조기에 시행할 수 있다. 1990년 Kalender 등
22)에 의해 나선형 CT촬영이 최초로 보고된 이래 뇌혈관의 해상도의 개선을 위한 많은 연구가 행해지고 있다. CTA의 해상도는 주사하는 순간 조영제의 혈관 내 농도와 주사절편간격의 최 소화에 의한 부분용적감소에 의해 결정된다
32)33). 혈관 내
조영제의 농도에 영향을 주는 인자로 환자의 나이와 뇌압의 변화, 체내 순환의 변화가 있으며, 직정맥동 및 중뇌동맥 주 위로 생기는 정맥에 의한 간섭이 있을 수 있으므로
28), 조영 제의 주사 및 주사시간의 최적화가 필요하다. 본 연구에서는 문헌을 참고하여
8)20)28)36)40)43)44)수 차례의 시행착오를 거쳐 140cc의 조영제를 4mm/sec. 속도로 주입하고, 주입 시작 15 초 후부터 35mm 용적깊이를 1mm 간격으로 1mm/sec.의 속도로 촬영하였고, 0.5mm 절편으로 재구성하였다, surface shaded display법
4)25)40)44)으로 영상을 재구성하여 재구성 시간을 단축하였으며 수술을 위한 동맥의 입체적인 해부학 적 구조를 얻을 수 있었다.
Katz와 Napel
23)은 Willis환을 이루고 있는 뇌혈관들의 해부학적 구조를 발견하는데 있어 CCA와 CTA의 차이는 없다고 하였다. Crompton
5)은 뇌동맥류의 파열은 동맥류의 직경이 4mm 이상일 때 증가한다고 하였다. Schwartz
34)는 3mm 이상의 뇌동맥류는 CTA로 진단이 가능하다고 하였 고, Young 등
43)은 CCA로 진단하지 못한 작은 뇌동맥류를 CTA로 진단할 수 있었다고 하였다. Lownie
27)는 뇌지주막
Fig. 4. A:Angiograms indicating a small middle cerebral artery aneurysm(arrow). B:Follow up angiograms showing the growth of the aneurysm(double arrow).
A A A A
B B
B B
하출혈 환자의 20%에서 다발성동맥류가 생긴다고 하였으 며, Dorsh
9)는 5%에서 뇌동정맥기형이 동반된다고 하였다.
Hacker 등
12)은 Willis환 밖에서 동맥류가 생기는 경우는 5-10%정도라고 보고하였다. Hope
16)는 CTA로 모든 뇌동 맥류를 진단할 수는 없었으나 뇌동맥류를 가진 모든 환자를 알 수는 있었다고 보고하였다.
본 연구에서 CCA 및 수술로 확인된 모든 동맥류에 있어 CTA의 발견예민도는 94.7%였고, Willis환 내 뇌동맥류의 발견예민도(sensitivity)는 98.2%였으며, 정확도(specifi- city)는 100%였다. CCA상 뇌동맥류를 가진 환자 중 진단 시 간과한 한 명을 제외한 모든 환자가 CTA에서도 1개 이 상의 뇌동맥류를 가졌다(발견예민도=97.8%). 뇌동맥류의 평균크기는 5.82mm였으며, CCA에서 3mm크기의 뇌동맥 류도 CTA로 진단이 가능하였다. CTA로 발견하지 못한 2 례에서 뇌동맥류 및 뇌동정맥기형이 CT촬영의 주사범위밖 에 있었으며, 뇌출혈이 피각부위에 있어 전교통동맥 동맥류 를 간과한 경우가 1례 있었다. 동맥류의 경부발견률 및 분 엽유무, 방향의 결정에서 두 검사 사이에 특이한 차이는 없 었으며 오히려 입체적인 영상을 돌려봄으로서 작은 동맥류 및 경부가 넓은 경우, 복잡한 작은 혈관이 동맥류 주위에 있 는 경우에는 CTA가 더 나았다. 2명의 환자에서 뇌동맥류-
클립복합체의 금속효과로 잔여동맥류를 확인할 수 없었으나, 주위구조 및 다른 부위에 생긴 뇌동맥류는 확인할 수 있었다.
CTA는 검사시간이 짧아 운동허상이 적고, 동맥의 유속 만 있으면 조영증강이 되어 뇌동맥류를 볼 수 있고, 다각도 의 영상을 얻을 수 있어 보다 나은 해부학적 구조인식 및 의심스러운 혈관병변의 확인이 가능하며, 특히 거대동맥류 의 주위 구조가 동맥류에 의해 가려져 안 보이는 경우에 유
용하다
7)8)24)32-34). 그러나 많은 양의 조영제가 필요하여 재
검사가 불가능하며, 영상의 질이 시술자의 기술에 크게 의 존되는 단점이 있다. 또, 전맥락막동맥과 같은 작은 중요혈 관이나 천공동맥, 측부혈관, 동맥경화성 변화 및 혈관연축을 CCA처럼 잘 보여주지 못하며, 뇌기저골에 의해 뇌동맥류가 가려질 수 있어 Willis환 내의 작은 뇌동맥류를 찾는데 주의 을 요한다. 또한 방사선 조사영역에 제한이 있어 뇌동맥류 가 주사범위밖에 위치한 경우에는 진단할 수 없다
6)11)32-34). 뇌동맥류 치료에 있어 CCA는 중요혈관의 확인, 측부혈 류에 대한 정보 및 거대동맥류의 수술 전 패색검사를 위해 서 필요하다
41). 또한 뇌동맥류와 동반된 뇌동정맥기형이나 다발성동맥류, 동맥박리증, 혈관염을 알기 위한 수술 전 검 사로서 필요할 것으로 사료된다.
CTA는 CCA가 불가능한 경우 및 응급을 요하는 경우에
Fig. 5. A:left carotid angiogram showing one straight clip located in right middle cerebral artery territory(star-mark) and two aneurysms in anterior cerebral artery(arrow) and left middle cerebral artery(arrowhead). B:CTA showing a metal artifact of aneurysmclip complex in right middle cerebral artery(double arrow). Aneurysmclip complex is not affecting on other two aneurysms.
A A
A A B B B B
CCA를 대신하여 시행할 수 있으며, 3차원적인 해부학적 구 조를 얻을 수 있어 CCA와 더불어 수술 전 검사로 유용하다.
또 높은 발견예민도와 정확도를 보이므로 주사영역을 조절 함으로서 뇌동맥류의 선별검사 및 미치료동맥류의 추적검사 로 유용하게 쓰일 수 있을 것이다.
결 론
전산화단층촬영 뇌혈관 조영술은 검사시간이 짧고 비침습 적인 검사로 해상도에 있어서도 고식적 뇌혈관조영술과 유 사하여 뇌동맥류 파열의 조기검사 및 고식적 뇌혈관조영술 의 보조적 검사로 가치가 있으며, 파열전 동맥류의 선별검 사로 널리 사용될 수 있을 것이다. 그러나 뇌동맥류와 동반 된 뇌동정맥기형이나 다발성동맥류의 검사 및 작은 중요혈 관의 확인과 측부 혈류에 대한 정보를 알기 위해 수술 전 검사로 고식적 뇌혈관조영술이 필요할 것으로 사료된다.
•
논문접수일:1999년 7월 5일•
심사완료일:1999년 8월 25일•
책임저자:이 혁 기701-600 대구광역시 동구 신암동 302-1 대구파티마병원 신경외과
전화:053) 940-7114, 전송:053) 954-7417 E-mail:[email protected]
References
1) Alberico RA, Patel M, Casey S, et al:Evaluation of the
circle of Willis with three-dimensional CT angiography in patients with suspected intracranial aneurysms. AJNR 16
:1571-1578, 1995
2) Almen T, Aspelin P:Cardiovascular effects of ionic mono-
meric and ionic dimeric and non-ionic contrast media. Effects in animals on myocardial contractile force, pulmonary and aortic blood pressure and aortic endothelium. Invest Radiol 10
:557, 1975
3) Anderson CM, Saloneer D, Tsuruda JS, et al:Artifact in ma-
ximum-intensity-projection display of MR angiograms. AJR 154
:623-629, 1990
4) Anderson GB, Findlay JM, Steinke DE, et al:Experience
with computed tomographic angiography for the detection of intracranial aneurysms in the setting of acute subarachnoid hemorrhage. Neurosurgery 41
:522-528, 1997
5) Crompton MR:Mechanism of growth and rupture in cere-
bral berry aneurysm. Br Med J 1
:1138-1142, 1966
6) Dillon EH, Van Leeuwen MS, Fernandez MA, et al:CTangiography
:Application to the evaluation of carotid artery stenosis. Radiology 189
:211-219, 1993
7) Dillon EH, van Leeuwen MS, Fernandez MA, et al:Spiral
CT Angiography. AJR 160
:1273-1278, 1993
8) Dorsch NWC, Young N, Kingston RI, et al:Early experience
with spiral CT in the diagnosis of intracranial aneurysms.
Neurosurgery 36
:230-238, 1995
9) Dorsch NWC:Special problems associated with subarach-
noid hemorrhage, in Youmans ed 4
:Neurological Surgery
:W.B. SAUNDERS 1996, Vol 2, pp1438-1441
10) Earnest F, Forbes G, Sandok BA, et al:Complications of ce-
rebral angiography
:Prospective assessment of risk. AJR 142
:247-253, 1984
11) Galanski M, Prokop M, Chavan A, et al:Renal arterial sten-
osis
:Spiral CT angiography. Radiology 189
:185-192, 1993
12) Hacker RJ, Krall JM, Fox JL:Data ⅠIn Fox JL, ed. Intracr-
anial aneurysms. New York
;Springer-Verlag, 1983, pp19-62
13) Harrison MJ, Johnson BA, Gardner GM, et al:Preliminaryresults on the management of unruptured intracranial aneury- sms with magnetic resonance angiography and computed to- mographic angiography. Neurosurgery l40
:947-957, 1997
14) Harbaugh RE, Schlusselberg DS, Jeffrey R, et al:Three dim-ensional computed tomographic angiography in the diagnosis of cerebrovascular disease. J Neurosurg 76
:408-414, 1992
15) Harbaugh RE, Schlusselberg DS, Jeffrey R, et al:Three dim-ensional computed tomographic angiography in the preoper- ative evaluation of cerebrovascular lesions. Neurosurgery 36
:320-327, 1995
16) Hope KA, Wilson JL, Thomson FJ:Three-dimensional CT
angiography in the detection and characterization of intrac- anial berry aneurysms. Am J Neuroradiol 17
:439-445, 1996
17) Horikoshi T, Jukamachi A, Nishi H, et al:Detection of intra-cranial aneurysms by three-dimensional time-of-flight mag- netic resonance angiography. Neuroradiol 36
:203-207, 1994
18) Imakita S, et al:Subtraction CT angiography with controlledorbit helical scanning for detection of intracranial aneurysms.
Am J Neuroradiol 19
:291-295, 1998
19) Jane JA, Kassel NF, Torner JC, et al:The natural history of
aneurysms and arteriovenous malformations. J Neurosurg 62
:321, 1985
20) Je H, Jung S, Kim TH, et al:Usefulness of computed tomo-
graphic angiography
(CTA
)in the evaluation of cerebral an- eurysms. J Korean Neurosurg Soc 25(2)
:331-337, 1996
21) Juvela S, Porras M, Heiskanen O:Natural history of unrup-tured intracranial aneurysms
:A long-term follow-up study. J Neurosurg 79
:174-182, 1993
22) Kalender WA, Seissler W, Klotz E, et al:Spiral volumetric
CT with single-breath-hold technique, continuous transport, and continuous scanner rotation. Radiology 176
:181-183, 1990
23) Katz DA, Marks MP, Napel SA, et al:Circle of Willis.
Evaluation with spiral CT angiography, MR angiography and conventional angiography. Radiology 195
:445-449, 1995
24) Klein HM, Bertalanffy H, Nayfrank L, et al:Three-dimen-sional spiral CT for neurosurgical planning. Neuroradiol
36
:435-439, 1994
25) Liang EY, Chan M, Hsiang JGK, et al:Detection and ass-
essment of intracranial aneurysms
:value of CT angiography with shaded-surface display. AJR 165
:1497-1502, 1995
26) Lanzino G, Kaptain G Kallmes DF, et al:Intracranial dis-secting aneurysm causing subarchnoid hemorrhage
:The role of computerized tomographic angiography and magnetic res- onance angiography. Surg Neurol 48
:477-481, 1997
27) Lownie SP:Cerebral Angiography:Multiple Aneurysms. in
Youmans ed 4 Neurological Surgery
:W.B. SAUNDERS 1996, Vol. 1, pp265-266
28) Nakajima Y, Yoshimine T, Yoshida H, et al:Computerized
tomographic angiography of ruptured cerebral aneurysms
:Factors affecting time to maximum contrast concentration. J Neurosurg 88
:663-669, 1998
29) Ogawa T, Okudera T, Noguchi K, et al:Cerebral aneu-
rysms
:Evaluation with three-dimensional CT angiography.
AJNR 17
:447-454, 1996
30) Park SH, Lee KH, Oh SM:The clinical usefulness and the
value of 3D CT angiography using spiral CT in patients with cerebral aneury. J Korean Neurosurg Soc 25(11)
:2234-2241, 1996
31) Rieger J, Hosten N, Neumann K, et al :Initial clinical
experience with spiral CT and 3D arterial reconstruction in intracranial aneurysms and arteriovenous malformations. Ne- uroradiology 38
:245-251, 1996
32) Ross JS, Masaryk TH, Modic MT, et al : Intracranial
aneurysms
:Evaluation by MR angiography. AJNR 11
:449- 455, 1990
33) Rubin GD, Dake MD, Napel SA, et al:Three-dimensional
spiral CT angiography of the abdomen
:Initial clinical ex- perience. Radiology 186
:147-152, 1993
34) Schwartz RB, Tice HM, Hooten SM, et al:Evaluation of
cerebral aneurysms with helical CT. Correlation with conven- tonal angiography and MR angiography. RSNA 192
:717-
722, 1994
35) Schwartz RB:Neuroradiological apllications of spiral CT.
Seminars in Ultrasound, CT, MRI 15
:139-147, 1994
36) Song SH, Yoon SH, Ahn YH, et al:Comparison between CTangiography and conventional angiography in the diagnosis of intracranial aneurysms. J Korean Neurosurg Soc 25(10)
:2017-2023, 1996
37) Tamatani S, Sasaki O, Takeuchi S, et al:Detection of dela-
yed cerebral vasospasm, after rupture of intracranial aneury- sms, by Magnetic Resonance angiography. Neurosurgery 40
:748-754, 1997
38) Tampieri D, Leblanc R, OleszekJ, et al:Three-dimensional
computed tomographic angiography of cerebral aneurysms.
Neurosurgery 36
:749-755, 1995
39) Velthuis BK, Rinkel GJE, Ramos LMP, et al:Subarachnoid
hemorrhage
:Aneurysmal detection and preoperative evalu- ation with CT angiography. Radiology 208
:423-430, 1998
40) Velthuis BK, van Leeuwen MS, Witkamp TD, et al:CT Ani-ography
:Source images and postprocessing techniques in the detection of cerebral aneurysms. AJR 169
:1411-1417, 1997
41) Vieco PT, Shuman WP, Alsofrom GF, Gross CE:Detectionof circle of Willis aneurysms in patients with acute subara- chonid hemorrhage
:A comparison of CT angiography and digital subtraction angiography. AJR 165
:425-430, 1995
42) Wilms G, Guffens M, Gryspeerdt S, et al:Spiral CT ofintracranial aneurysms
:Correlation with digital subtraction and magnetic resonance angiography. Neuroradiology 38
:520-525, 1996
43) Young N, Dorsch NWC, Kingston RJ, et al:Spiral CT
scanning in the detection and evaluation of aneurysms of the circle of Willis. Surg Neurol 50
:50-61, 1998
44) Zouaoui A, Sahel M, Marro B, et al:Three-dimensional