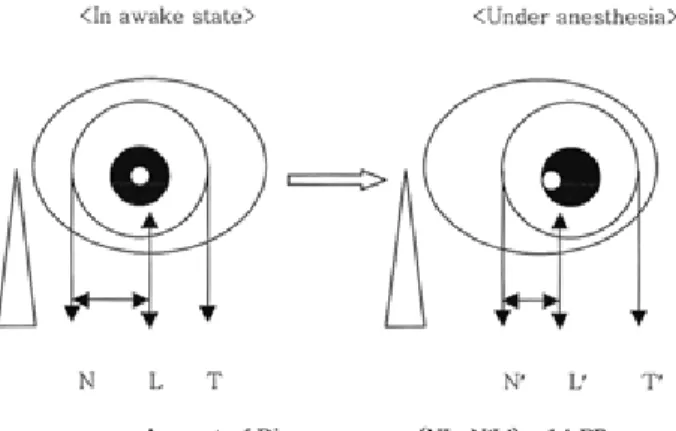
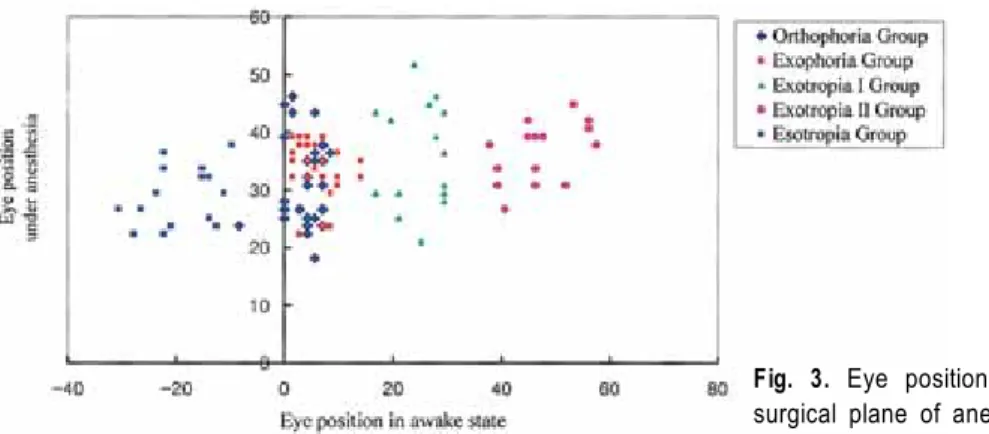
Change of eye position in patients with orthophoria and horizontal strabismus under general anesthesia
7
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
수치

관련 문서
The second method is for compensation thermal expansion offering pre-load assembling that the temperature change by the repetitive movement and the friction
The characteristic change according to the main design parameters of the magnetic gear can be confirmed, and the difference in loss and efficiency according
In this study, therefore, the method for measuring residual stresses using ESPI technique that is one of the laser applied measurement technique excellent in the view
The subjects were bowling community members and general bowling users in G Metropolitan City in 2013 selected by a convenience sampling
First, in the difference in Taekwondo image, Taekwondo loyalty, and memorial intention according to the general characteristics (gender, nationality,
In a difference according to position, fairness and immediacy show a statistically meaningful difference, and centers have the lowest awareness about the
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
Regarding SI or BI EMG measured at upright posture on hard platform, bio-feedback group under the condition with opening both eye and aqua group under the condition with
