ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
<접수일:2004년 8월 30일, 심사통과일:2005년 7월 26일>
※통신저자:김 신 규
서울시 성동구 행당동 17번지, 한양대학교 류마티스병원 진단면역과, 진단검사의학과 Tel:02) 2290-9200, 8975, Fax:02) 2298-1735, E-mail:[email protected]
Can Polymerized C9 be a New Disease Activity Parameter in Rheumatoid Arthritis?
Jung-UK Sir, M.D., Think-You Kim, M.D.
Department of Diagnostic Immunology/Laboratory Medicine,
The Hospital for Rheumatic Diseases, Hanyang University Medical Center, Seoul, Korea
= 국문초록 =
류마티스 관절염에서 질병활성 표지자로서의 중합 C9 검사의 유용성
한양대학교 류마티스병원 진단면역과, 진단검사의학과 서 정 욱․김 신 규
목적: 류마티스 관절염은 만성적으로 진행되는 전신적인 염증성 질환이며 주요 관절의 변형이나 장애를 초래하게 된다. 질병활성 표지자(disease activity parameter)는 이러한 염증성 질환의 활성도 를 측정하는 객관적인 지표로서 환자의 상태를 평가하고 치료계획을 수립하는데 중요한 역할을 하게 된다. 저자들은 류마티스 관절염에 대해 현재까지 알려져 있는 C반응성단백(C-reactive protein, CRP), 류마티스 인자(rheumatoid factor, RF), 적혈구침강속도(erythrocyte sedimentation rate, ESR) 등과 같은 질병활성 지표들의 결과와 최근에 소개된 시험관에서 보체를 활성화시킨 후 단일 클론성 항체를 사용하여 보체 활성의 최종 생성물인 중합 C9 (polymerized C9)을 정량적으로 측정 하는 중합 C9 검사의 결과를 비교하여 류마티스 관절염의 새로운 질병활성 표지자로서의 유용성 과 류마티스 관절염 환자에서 동반되는 신장병증의 예측인자로서의 가능성을 알아보고자 하였다.
방법: 미국 류마티스 협회의 류마티스 관절염 진단 기준에 의해 류마티스 관절염으로 진단 받은 대상 환자군(n=86)의 임상 소견 및 검사 소견을 종합하여 류마티스 관절염 활성군(active RA, n=43), 류마티스 관절염 비활성군(inactive RA, n=35) 및 신장병증을 동반한 류마티스 관절염군(RA with nephropathy, n=8)으로 분류하였고, 각 군에서 CRP, RF, ESR 및 중합 C9 검사(CAE, INCSTAR- DiaSorin, Italy)를 시행하였다. 각 검사간의 민감도와 특이도 비교는 ROC 곡선(receiver operating characteristic curve)을 통하여 시행하였고 통계처리는 ANOVA test를 시행하였다.
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic, recurrent, systemic inflammatory disease and results in major de- formity or dysfunction of joints. A disease activity parameter has the important clinical significance be- cause it is a useful objective tool for assessing disease activity and planning individualized therapeutic pro- gram. The early detection of combined nephropathy in a patient with RA is an important issue for clinical immunology laboratory because it is closely associated with long-term patient prognosis and renal survival1). In clinical immunology laboratory, a few parameters are available such as C-reactive protein (CRP), eryth- rocyte sedimentation rate (ESR), or rheumatoid factor (RF). CRP and ESR tests are based on the reaction of acute phase reactants in patient with inflammatory disorder. Acute phase reactants, which are produced in the liver in response to cytokines synthesized in in- flamed tissue, limit the tissue damage due to inflam- mation. They serve as markers for disease activity and include serum amyloid A, fibrinogen, haptoglobin, complement, and CRP2). ESR is a simple and an in- expensive clinical test that had been used in most laboratories. ESR, however, is a reflection of the level of acute phase reactants and is influenced by some other factors including age, sex, and anemia3,4). On the other hand, CRP is a direct measure of the inflam-
mation and rises in hours to an inflammatory stimulus and returns to normal in a few days after the stimulus is removed. Thus, CRP is a more useful clinical mar- ker of active inflammation and its resolution. However, CRP is not as simple or inexpensive as ESR and requires special assay equipment. As with ESR, CRP can be elevated by pregnancy, trauma, and stress, but it does not vary with age or sex. In approximately 20% of patients with clinically apparent RA, RF may yield negative results, but a positive RF test had been found to predict more severe disease than a negative RF test. The concentration of serum RF may fluctuate with the degree of inflammation and disease activity in RA, but the variation in RF can be measured suffi- ciently precisely only with continuous techniques, such as nephelometry5). Thus, RF had been used as a screening test rather than a disease activity marker for RA.
Abnormal values of serum complement are closely associated with rheumatic diseases and concomitant ne- phropathy, such as systemic lupus erythematosus (SLE), lupus nephritis, and RA. Complement can function as two kinds of marker at the same time, one is inflam- matory activity marker as an acute phase reactant and another is nephropathy marker due to systemic com- plement consumption in rheumatic patients with ne- phritis6,7). Traditional tools for complement are comple- ment activity (CH50) or serum levels of C3 and C4.
However, these are neither sensitive nor precise for 결과: CRP, RF, ESR 및 중합 C9 검사는 류마티스 관절염의 활성군과 비활성군의 비교에서 모두 통계적으로 유의한 차이를 보였고(p<0.05), ROC 곡선을 통한 각 검사간의 민감도와 특이도의 비 교에서는 중합 C9 검사와 CRP 검사가 가장 우수한 결과를 보였다. 한편, 류마티스 관절염의 비활 성군과 신장병증을 동반한 류마티스 관절염군의 비교에서는 중합 C9 검사만이 통계적으로 유의한 차이를 보였다(p<0.05).
결론: 중합 C9 검사는 류마티스 관절염에 있어서 질병 활성도를 잘 반영하는 새로운 질병 감시 지표가 될 것으로 사료되며, 예후에 중요한 영향을 미치는 신장병증의 동반 유무를 예측할 수 있는 유용한 검사가 될 것으로 사료된다.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Complement, C-reactive protein, Erythrocyte sedimentation rate, Rheumatoid
factor, Rheumatoid Arthritis
clinical use because they have a wide reference range and a number of reagents that are difficult to stan- dardize. Polymerized C9 testing is a novel approach for measurement of total classical complement activity.
After in vitro activation of complement in a well of a microtiter plate, the neoantigen of terminal polymerized C9 is quantified by using an enzyme- conjugated mo- noclonal antibody. This newer method compared well with a CH50 assay and was equally sensitive in screen- ing routine clinical data8).
We evaluated polymerized C9 in RA patients with various disease states, as a new disease activity para- meter for RA and a marker for concomitant nephro- pathy, and we compared it with CRP, ESR, and RF at the same time.
MATERIALS AND METHODS 1. The study population and RA patients groups
The study population for this investigation was selected at random from all patients who met the RA criteria of the American College of Rheumatology and diagnosed at the Hospital for Rheumatic Diseases, Hanyang University Medical Center, Seoul, Korea.
Polymerized C9, CRP, ESR and RF testing on 86 pa- tients were undertaken. Patients were divided into three groups based on the severity of their disease process.
On the basis of clinical and laboratory review, such as morning stiffness, joint pain, existence of newly aff- ected joint, routine urine analysis (RUA) and/or renal biopsy, three groups of patients were defined as active RA (n=43), inactive RA (n=35), and RA with neph- ropathy (n=8). The asymptomatic cases were included to inactive RA group, and other cases that had mild to severe symptoms were included to active RA group.
In RA with nephropathy group, all of these RA pa- tients had proteinuria and/or hematuria of renal origin that was evaluated for other causes by ultrasonography, and a few patients had nephropathy that was proven by renal biopsy. For the evaluation of serial change of polymerized C9 and CRP, we followed up the results
of specimens for 2 weeks in active RA patients (n=8) who were treated with disease-modifying antirheumatic drugs (DMARD), nonsteroidal anti-inflammatory drugs (NSAIDs), and/or low dose steroid.
2. Methods
1) Polymerized C9 assay: Serum specimens were obtained from all patients using standard complement procedures. A minimum of 5 mL of whole blood was collected and allowed to clot in plain tube, without serum separator, for 60∼65 minutes at room tem- perature (20∼25oC). Blood samples were centrifuged in a refrigerated centrifuge and cell-free serums were transferred to clean tubes. Fresh serum was stored at -70oC and was not thawed for other purposes.
Polymerized C9 assay (CAE, INCSTAR-DiaSorin, Ita- ly) were carried out according to enzyme immunoas- say (EIA) method. 5μL of serum was diluted into 1:
120 with cold sample diluents on the ice bath. 150μL of diluted sample was applied to duplicate microtiter wells which was coated with rabbit gamma globulin.
After complement activation at 37oC for 60 minutes, the neoantigen of terminal polymerized C9 was quan- tified by using horseradish peroxidase (HRP) conjugat- ed monoclonal antibody at 450 nm. Results were ex- pressed relative to the reference serum and calculated from the average of duplicated sample. Reference range of polymerized C9 assay was 63∼145 (CAE Units).
2) CRP, RF and ESR test: Quantification of CRP and RF levels were performed by nephelometry using Beckman ArrayⓇ 360 system. Reference range of CRP level was less than 0.8 mg/dL and RF was less than 20 IU/mL. ESR test was performed by modified Win- trobe method. Reference range of ESR was less than 10 mm/hr for men, and was less than 20 mm/hr for women.
3. Statistics
In comparing with sensitivity and specificity of each disease activity parameter, we performed the receiver
operating characteristic test (ROC) in each disease group. In comparing with levels of each parameter between disease groups, we performed statistical analy- sis with multiple comparisons between groups after ANOVA test using SPSS for windows.
RESULTS
We compared means of polymerized C9, CRP, ESR, and RF levels between 3 disease categories by mul- tiple comparisons after ANOVA test (Table 1∼3). In Table 1. Comparisons of polymerized C9, CRP, ESR, and RF levels between RA patient groups
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Mean±SD
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Patients groups No. (n=86) CRP ESR RF Polymerized C9
(mg/dL) (mm/hr) (IU/mL) (CAE Unit)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
I. Active RA 43 2.8±2.7* 45.0±12.5* 231.0±176.2* 128.6±29.0*
II. Inactive RA 35 0.7±0.9* 29.9±16.7* 120.5±92.8* 93.6±28.0*
III. RA with nephropathy 8 0.7±0.9 41.1±12.8 212.4±198.1 54.5±19.2*
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*Mean difference between groups: p<0.05. CRP: C-reactive protein, ESR: erythrocyte sedimentation rate, RF:
rheumatoid factor, RA: rheumatoid arthritis
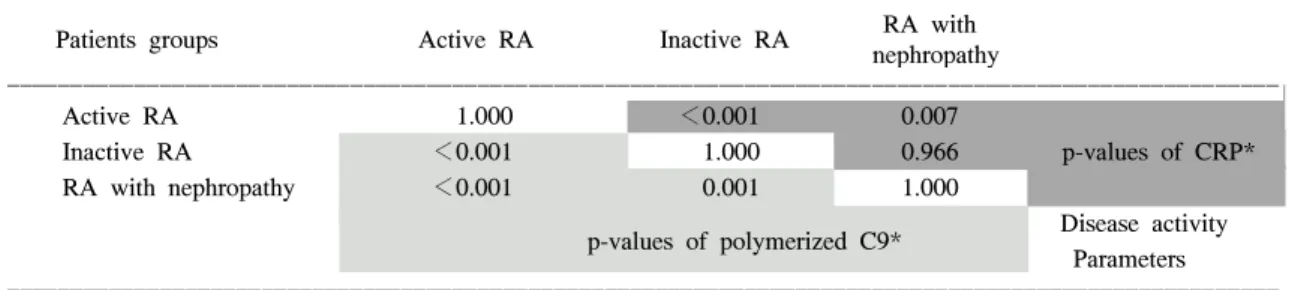
Table 2. p-values in multiple comparisons of polymerized C9 and CRP levels between RA patient groups
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
RA with
Patients groups Active RA Inactive RA
nephropathy
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Active RA 1.000 <0.001 0.007
Inactive RA <0.001 1.000 0.966 p-values of CRP*
RA with nephropathy <0.001 0.001 1.000
Disease activity p-values of polymerized C9*
Parameters ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*Multiple comparisons after ANOVA test. CRP: C-reactive protein, RA: rheumatoid arthritis
Table 3. p-values in multiple comparisons of RF and ESR levels between RA patient groups
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
RA with
Patients groups Active RA Inactive RA
nephropathy
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Active RA 1.000 <0.001 0.484
Inactive RA 0.002 1.000 0.057 p-values of ESR*
RA with nephropathy 0.748 0.122 1.000
Disease activity p-values of RF*
Parameters ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*Multiple comparisons after ANOVA test. RF: rheumatoid factor, ESR: erythrocyte sedimentation rate, RA: rheumatoid arthritis
comparing with each disease activity parameter in RA, polymerized C9, CRP, ESR, and RF made a distinc- tion between active RA and inactive RA (p<0.05) (Table 1). The ROC performance test showed polyme- rized C9 and CRP as the best disease activity parame- ter in RA (Table 4). However, only polymerized C9 discriminated active RA from inactive RA and also predicted nephropathy in RA patient (p<0.05)(Table 1∼4). Follow-up results of polymerized C9 and CRP in 8 patients mostly showed similar trends (Fig. 1), and showed that CRP tended to response rapidly than polymerized C9, and also it decreased to within nor- mal limit in a week or a few more days.
DISCUSSION
We evaluated the cross sectional comparative use- fulness of polymerized C9, CRP, ESR, and RF in RA patient with various disease states. Our experience shows that measurement of serum polymerized C9 level is a new clinical guide as a useful parameter for disease activity of RA and a predictor for concomitant nephropathy in RA patients. Because the purpose of our study was to investigate the possibility as a new disease activity marker of polymerized C9 in com- paring with previously well investigated other markers, Table 4. AUC of polymerized C9, CRP, ESR, and RF in comparing between RA patient groups
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Comparing patients groups
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ RA activity parameter Active RA vs. Inactive RA Inactive RA vs. RA with nephropathy
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
AUC SE AUC SE
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Polymerized C9 0.8123 0.0506 0.8964 0.0538
CRP 0.8345 0.0462 0.5294 0.1352
ESR 0.7647 0.0608 0.7235 0.0970
RF 0.6811 0.0656 0.6018 0.1497
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ AUC: the area under a ROC curve, SE: standard error, CRP: C-reactive protein, ESR: erythrocyte sedimentation rate, RF: rheumatoid factor, RA: rheumatoid arthritis
Fig. 1. Follow-up data of polymerized C9 and CRP in 8 active RA patients for 2 weeks. The con- tinuous lines indicate level of polymerized C9, and the interrupted lines indicate level of CRP, the horizontal interrupted lines indicate the upper and lower limits of reference range for polymerized C9 and CRP. CRP: C-reactive protein, RA: rheumatoid arthritis.
Polymerized C9 (Units)
0
Day 0
250
CRP (mg/dL)
50 200
150 100 50
40 30 20 10
0
1 7 14
Polymerized C9 CRP
such as CRP or ESR, we defined concise patient group- ing, such as active or inactive, rather than grade sys- tems used in other studies9,10). Thus, we could not describe in more detail how these parameters correlate with the severity of RA. Our results showed all para- meters made a distinction between active RA and inac- tive RA (p<0.05)(Table 1). However, for inactive RA group, where the parameters should mostly be within normal range, only 20% (7/35) of those cases had normal range RF figure whilst other parameters in- cluding C9 and CRP had 83% (29/35) and 71% (25/
35) of those cases that were within normal ranges, respectively. In comparing discriminate performance by comparing the area under a ROC curve (AUC) bet- ween active RA and inactive RA, we found CRP and polymerized C9 had good performance, and ESR and RF in order (Table 4).
Measuring levels of C3 and C4 components and CH50 activity remains useful in predicting the activity of lupus nephritis. However, these tests have been regarded as rarely useful in gauging the activity of other connective tissue diseases. Our results showed significant correlation between serum polymerized C9 levels and RA disease groups. In our cases, when complement acts as an acute phase reactant in an in- flammatory disease process, measured polymerized C9 tended to be elevated. On the other hand, measured polymerized C9 often were more decreased in RA nephropathy than in the cases without nephropathy.
Although traditional complement assay (CH50) can pro- vide general information about the integrity of the classical complement pathway, the principle of poly- merized C9 assay is quite different with that of tra- ditional CH50 assay. Therefore, it is clear that accurate and reproducible assay can reflect disease status ex- actly. In polymerized C9 assay, the source of error can be decreased by using simple enzyme immunoas- say and calculating the result from the average of dup- licated sample. Renal disorders are a frequent cause of death in patients with RA1). Renal amyloidosis and gold or D-penicillamine induced glomerulonephritis are
the most well known renal abnormalities associated with RA. These cases are not usually associated with immune complexes or complement activation. However, deposits of immunoglobulins and complement have been detected by immunofluorescence in renal biopsy of RA with hematuria or proteinuria11). Renal disorder in RA patients is less manifested than in patients with other rheumatic disorders such as SLE. This could be explained by a slow rate of progression and insensitive screening methods1). Previous other study showed he- maturia in RA patients was associated with mesangial glomerulonephritis11,12), and in other report, there were no differences in the concentration of C3 and C4 bet- ween the various RA nephropathy groups and con- trols13). Our results showed significant mean differences between RA with nephropathy and other disease groups (p<0.05) while other parameters could not.
Among 8 cases of RA with nephropathy, 2 cases were active RA and 6 cases were inactive RA. Because we used small sized cases, we could not evaluate the influence of disease activity on polymerized C9 levels in RA with nephropathy. However, Our results showed association of complement activation and RA patients who have evidence of nephropathy, such as hematuria and/or proteinuria. Therefore, we thought that additio- nal polymerized C9 assay with routine measure for renal function would be required in clinical care.
In conclusion, the measurement of serum poly- merized C9 level can be a new clinical guide as a disease activity parameter for RA and predictive para- meter for nephropathy in RA.
ACKNOWLEDGEMENTS
We would like to thank Dr. Won-Ho Choe for his thoughtful review of this manuscript.
REFERENCES
1) Boers M. Renal disorders in rheumatoid arthritis.
Semin Arthritis Rheum 1990;20:57-68.
2) Kushner I. C-reactive protein and the acute-phase response. Hosp Pract 1990;25:13-28.
3) Bötiger LE, Svedberg CA. Normal erythrocyte se- dimentation rate and age. Br Med J 1967;2:85-7.
4) Bull BS. Is a standard ESR possible? Lab Med 1975;6:31-5.
5) Wener MH. Rheumatoid factors. In: Rose NR, Ha- milton RG, Detrick B, eds. Manual of clinical la- boratory immunology. 6th ed. p. 961-72, Washing- ton DC, ASM press, 2002.
6) Frank MM. Detection of complement in relation to disease. J Allergy Clin Immunol 1992;89:641-8.
7) Goldstein IM. Clinical applications of complement measurement in rheumatic diseases. Am J Med Sci 1975;269:172-81.
8) Jaskowski TD, Martins TB, Litwin CM, Hill HR.
Comparison of three different methods for mea- suring classical pathway complement activity. Clin Diagn Lab Immunol 1999;6:137-9.
9) Wolfe F. Comparative usefulness of C-reactive pro- tein and erythrocyte sedimentation rate in patients
with rheumatoid arthritis. J Rheumatol 1997;24:
1477-85.
10) Mallya RK, de Beer FC, Berry H, Hamilton EDB, Mace BEW, Pepys MB. Correlation of clinical parameters of disease activity in rheumatoid ar- thritis with serum concentration of C-reactive pro tein and erythrocyte sedimentation rate. J Rheuma- tol 1982;9:224-8.
11) Helin H, Korpela M, Mustonen J, Pasternack A.
Mild mesangial glomerulopathy-a frequent finding in rheumatoid arthritis patients with hematuria or proteinuria. Nephron 1986;42:224-30.
12) Hordon LD, Sellars L, Morley AR, Wilkinson R, Thompson M, Griffiths ID. Haematuria in rheuma toid arthritis: an association with mesangial glome- rulonephritis. Ann Rheum Dis 1984;43:440-3.
13) Korpela M, Mustonen J, Helin H, Pasternack A.
Immunological comparision of patients with rheu- matoid arthritis with and without nephropathy. Ann Rheum Dis 1990;49:214-8.
Abstract ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Objective: Rheumatoid arthritis (RA) is a chronic, recurrent, systemic inflammatory disease and results in major deformity or dysfunction of joints. A disease activity parameter has important clinical significance because it is a useful objective tool for assessing disease activity and planning individualized therapeutic program. However, in RA, only a few parameters have been available such as C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), or rheumatoid factor (RF). By using these parameters, it is difficult to recognize concomitant nephropathy in RA. Therefore, as a new disease activity parameter for RA and a marker for nephropathy, we evaluated polymerized C9 which is the neoantigen produced after in vitro activation of complement and is quantified by using an enzyme conjugated monoclonal antibody.
Methods: Polymerized C9 (CAE, INCSTAR-DiaSorin, Italy), CRP, ESR and RF testing on 86 patients diagnosed with RA were undertaken. According to clinical and laboratory review, we grouped the patients into three disease categories as active RA (symptomatic, n=43), inactive RA (asymptomatic, n=35), and RA with nephropathy (n=8) and compared the means between three groups.
Results: In comparing with each disease monitoring parameter between groups, polymerized C9, CRP, ESR, and RF discriminated active RA from inactive RA (p<0.05). The ROC performance test showed polymerized C9 and CRP are the two best parameters in discriminating disease activity of RA. Furthermore, only polymerized C9 accurately discriminated disease activity and also predicted nephropathy in RA patient (p<0.05).
Conclusion: Like CRP, Polymerized C9 can be a useful disease activity parameter for RA and also a predictive parameter for RA nephropathy.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ