Vol. 11, No. 3, September, 2004
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
<접수일:2004년 2월 17일, 심사통과일:2004년 6월 17일>
※통신저자:박 성 환
서울시 서초구 반포동 505번지 강남성모병원 류마티스 내과
Tel:02) 590-2712, Fax:02) 599-3589, E-mail : [email protected] 이 논문은 한국과학재단 우수연구센터 연구(R11-2002-098-01001-0)의 지원으로 이루어졌음.
베체트병 환자에서 혈청 대식세포 유주 억제 인자 (Macrophage Migration Inhibitory Factor, MIF)의 상승
가톨릭대학교 강남성모병원 류마티스내과
김성동․김상현․김해림․박미경․윤종현․김완욱 이상헌․박성환․조철수․김호연
= Abstract =
Elevated Serum Levels of Macrophage Migration Inhibitory Factor (MIF) in Patients with Behcet's Disease
Sung-Dong Kim, M.D., Sang-Hyon Kim, M.D., Hae-Rim Kim, M.D., Mi-Kyung Park, M.S., Chong-Hyeon Yoon, M.D., Wan-Uk Kim, M.D., Sang-Heon Lee, M.D., Sung-Hwan Park, M.D., Chul-Soo Cho, M.D., Ho-Youn Kim, M.D.
Department of Internal Medicine, Division of Rheumatology, Kangnam St. Mary's Hospital, College of Medicine, The Catholic University of Korea
Objective: Macrophage migration inhibitory factor (MIF) has emerged recently as an im- portant regulator of inflammatory and immune responses. This work was undertaken to evaluate serum levels of MIF and in vitro MIF production by whole blood cells in patients with Behcet's disease and investigate the relationship between serum levels of MIF and clinical manifestations.
Methods: Sixty-five patients with Behcet's disease and forty-eight healthy controls were studied to evaluate serum levels of MIF. Six patients with Behcet's disease and Five healthy controls were studied for evaluating the production of MIF by whole blood cells.
Serum and culture supernatant levels of MIF were measured by enzyme-linked immuno- sorbent assay (ELISA). The production of MIF by whole blood cells was investigated by culturing peripheral blood cells in the absence or presence of Concanavalin A (Con A).
서 론
베체트병은 구강과 외음부의 재발성 궤양, 피부병 변 및 포도막염 등을 특징으로 하며, 관절, 위장관, 혈관, 중추 신경계 등 여러 장기를 침범하는 염증성 질환으로 증상의 악화와 완화가 반복되는 것을 특징 으로 한다. 특히 혈관, 장관, 및 중추신경을 침범하 는 경우는 생명을 위협할 수 있다1). 베체트병의 병 인은 아직까지 확실히 밝혀지지 않았지만 선천면역 과 적응면역이 모두 관여하며 염증유발성 시토카인 과 Th1 형 시토카인이 활성화되고 부착분자나 염증 유발성 시토카인에 대한 유전변이와 같은 면역이상 으로 더 강력한 중성구 및 T세포 반응을 유발한다 고 알려져 있다. 또한 전사인자의 세포 내 신호이상 으로 외부자극에 대한 염증반응에 대한 역치를 떨어 뜨린다. 적응면역도 중요한 역할을 하며 외부(연쇄 구균, 초항원) 및 내부항원(열 충격 단백질, 장기 특 이 단백질)에 작용하여 조직 T 세포 침착을 유발한 다2). 베체트병의 면역학적 병인에 널리 알려진 가설 에 따르면 여러 가지 항원에 대한 T세포의 과민반 응과 이에 따른 단핵구의 활성화로 인터루킨 12의 생성을 유발하고 이 시토카인이 Th1 반응을 자극한 다. 또한 비정상적인 T세포 활성화로 인해 인터루킨 8, 인터루킨 17, 감마인터페론과 종양괴사인자와 같 은 시토카인에 의해 중성구가 활성화된다1).
대식세포 유주 억제 인자는 활성화된 T 세포에서 분비되어 대식세포의 이동을 억제하고 세포 내 기생 체나 종양세포를 사멸하는 능력을 향상시키는 물질
로 처음 알려졌다3-5). 최근의 연구에서는 대식세포, 내피세포, 섬유모세포 등에서도 분비되어6-8) 종양발 생과 같은 세포성장, T 세포 활성화와 혈관신생에도 관여하며 여러 가지 염증이나 면역 반응에 중요한 역할을 한다고 알려졌다9,10). 특히 종양괴사인자, 인 터루킨-1, 인터루킨-6, 인터루킨-8을 포함하는 염증유 발성 시토카인의 합성을 유발하고 글루코코르티코이 드에 의한 시토카인 생산억제를 길항하는 특수한 기 능을 가진다11). 이러한 MIF의 발현증가가 건선, 사 구체신염, 이식 거부, 유육종증, 천식을 포함하는 여 러 가지 면역 및 염증성 질환에서 보고되어 왔다12). 류마티스 질환에서의 MIF에 대한 연구를 살펴보면, 류마티스관절염에서는 환자의 염증성 활막조직에서 높은 MIF의 발현을 보인다고 하였고13), 활막의 MIF 발현 정도와 질병 활성도와의 연관성을 증명하여 류 마티스 관절염에 항 MIF 치료의 가능성을 보여주었 다14). 전신성 경화증에서 혈청 및 피부조직에서 MIF 의 발현 증가를 증명하여 병인에 중요한 역할을 할 것으로 보고하였으며15), 연소성 류마티스 관절염 환 자의 혈청과 활액에서 MIF가 증가됨을 보고하였다16). 베체트병에서 MIF에 대한 연구는 활성기의 포도 막염을 동반한 베체트병 환자에서 MIF의 농도가 증 가한다고 하였으며17), 신경을 침범한 베체트병에서 도 뇌척수액 내 MIF농도가 증가된다18)는 일부 보고 가 있으나 환자의 임상 양상과, 질병 활성도와의 관 련성에 대한 연구는 없었다.
본 연구에서는 베체트병 환자에서 혈청과 말초혈 액 세포 배양 상층액에서 MIF의 농도를 측정하고 MIF 수치와 환자의 임상양상과의 연관성을 알아보 Results: Serum levels of MIF were higher in patients with Behcet's disease than in healthy controls. Serum levels of MIF were changed in each patient with Behcet's disease according to clinical disease activity (higher at active state). The MIF production by Con A-stimulated peripheral blood cell culture was higher in patients with Behcet's disease than in healthy controls.
Conclusion: Circulating levels of MIF are higher in patients with Behcet's disease than in healthy controls and the levels of MIF may be associated with clinical disease activity. MIF may play an important role as a mediator of inflammation in Behcet's disease and provide opportunity for the development of anti-MIF strategy for the treatment of patients with Behcet's disease.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Behcet's disease, Macrophage migration inhibitory factor (MIF)
고 또한 각 환자에서 시간에 따른 임상적 질병 활성 도의 변화에 따라 혈청 MIF 수치의 변화를 알아보 고자 하였다.
대상 및 방법 1. 연구대상
가톨릭대학교 부속 강남성모병원 류마티스 센터에 내원한 International Study Group Criteria for Behcet's disease 진단 기준19)을 만족하는 베체트병 환자 65명 (남자 18명, 여자 47명; 평균연령 41.4±9.9)과 정상 인 48명(남자 20명, 여자 28명; 평균연령 43.5±9.6) 을 대상으로 하였다. 베체트병 환자들의 평균 유병 기간은 10.7±8.1년이었고 평균 발병 연령은 30.7±
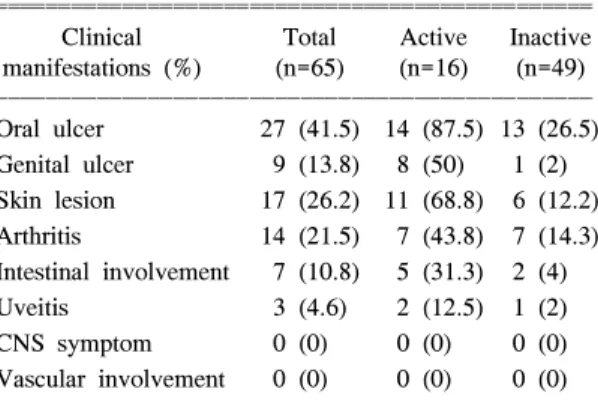
9.2세였다. 환자는 채혈 당시의 임상증상을 기준으로 활성상태와 비활성상태로 나누었는데, 구강궤양, 외 음부궤양, 관절염, 피부병변, 포도막염, 혈관염, 장염 및 중추신경증상 중 두 가지 이상이 있는 경우 활성 상태로 분류하였다. 환자 중 16명(25%)이 활성 상태 였고 49명(75%)이 비활성상태였다. 활성 상태의 환 자와 비활성 상태 환자의 평균 유병기간은 각각 10
±7.1, 11±8.6년이었고 평균 발병 연령은 33.8±8, 30±9.2세로 차이가 없었다. 혈관염과 중추신경 증상 은 한 명도 없었고 다른 증상들은 모두 활성 상태의 환자들에서 더 많이 나타났다(표 1). 채혈한 혈액은 혈청을 분리한 후 MIF를 측정하기 위해 -20oC에서 보관하였다. 65명의 환자 중 22명에서 3개월 후 재
채혈을 하여 혈청 MIF를 측정하였고 재채혈 당시의 질병 활성도를 기록하여 각각의 베체트병 환자에서 시간에 따른 질병 활성도의 변화에 따라 혈청 MIF 의 변동을 알아보고자 하였다.
2. 전혈 세포 분리 및 배양
6명의 환자와 5명의 정상 대조군의 전박정맥에서 헤파린으로 처리된 주사기로 10 mL의 혈액을 채취 한 후 10% FBS (fetal bovine serum)가 첨가된 IMDM (2 mM L-glutamine, 100 IU/mL penicillin, 100μg/mL streptomycin) 배양액에 1:5의 비율로 희석하여 24- well 세포배양판(TRP, Switzerland)에 넣어 각각 2 well 씩 Concanavalin A (Con A)10μg/mL로 자극하였고, 5% CO2, 37oC 배양기에서 3일간 배양한 후 배양액 상층액을 취하여 MIF 농도를 측정하였다.
3. MIF의 측정
혈청 MIF와 배양액 상층액에 있는 MIF농도는 sand- wich ELISA로 측정하였다. Sandwich ELISA용 96 well plate (NUNC, Denmark)에 단클론성 MIF 항체 (R&D, USA) 4μg/mL로 50μL/well씩 넣고 4oC에 밤 새 반응시킨 다음 차단용액(1% BSA/PBST)을 200μL/
well씩 넣고 실온에서 2시간 반응시켰다. Standard로 는 재조합 인형 MIF (R&D, USA)를 이용하여 5 ng/
mL∼7.8 pg/mL 농도를 사용하였다. 표준시료와 함께 측정할 혈청 및 세포 배양 상층액을 50μL/well씩 넣 고 실온에서 2시간 반응시켰다. 반응용기를 세척용 액(0.05% Tween20/ Phosphate-Buffered Saline)으로 4 번 세척하고 Biotinylated goat-anti-human MIF antibody (R&D, USA)를 200 ng/mL로 희석하여 50μL/well씩 넣어 실온에서 2시간 반응시킨 후 세척용액으로 4번 세척하였다. 마지막으로는 Extravidin-Alkaline phospha- tase conjugate(SIGMA, USA)를 1:2000으로 희석하여 50μL/well씩 넣고 실온에서 2시간 반응시키고 세척 후 PNPP (Fluka, Phosphate Disodium Salt Hexahy- drate)/DEA 용액 (Diethanolamine 97 mL, NaN3 0.2 g, MgCl26H2O 0.1 g, 1차 증류수 800 mL)을 1 mg/mL 농도로 녹여 50μL/well씩 넣어 30분 후 0.2 M NaOH 로 반응을 멈추고 405 nm파장에서 흡광도를 측정하 였다.
Table 1. Clinical characteristics of patients with Beh- cet's disease
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Clinical Total Active Inactive manifestations (%) (n=65) (n=16) (n=49) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Oral ulcer 27 (41.5) 14 (87.5) 13 (26.5) Genital ulcer 9 (13.8) 8 (50) 1 (2) Skin lesion 17 (26.2) 11 (68.8) 6 (12.2) Arthritis 14 (21.5) 7 (43.8) 7 (14.3) Intestinal involvement 7 (10.8) 5 (31.3) 2 (4) Uveitis 3 (4.6) 2 (12.5) 1 (2) CNS symptom 0 (0) 0 (0) 0 (0) Vascular involvement 0 (0) 0 (0) 0 (0) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ CNS: central nervous system
4. 통계분석
베체트병 환자와 건강대조군 사이의 혈청 MIF 농 도의 차이, 질병 활성도에 따른 베체트병 환자의 혈 청 MIF 농도의 차이, Con A 자극에 따른 베체트병 환자와 정상인의 말초혈액 배양세포의 MIF 분비능 의 차이 및 각 환자에서 질병 활성도에 따른 MIF 농도의 차이는 SPSS (Windows용 SPSS 11.0)를 이용 한 independent Student's t-test, paired t-test 및 Mann- Whitney test를 시행해서 분석했고 통계학적 유의성 의 수준은 p<0.05인 경우로 하였다.
결 과
1. 베체트병 환자와 정상인의 혈청 MIF
혈청 MIF 농도는 베체트병 환자에서 8777±4712 pg/mL (평균값±표준편차)였고 정상 대조군은 665±
329 pg/mL로 환자군에서 유의하게 높았다(p<0.001) (그림 1). 환자군과 정상 대조군 모두에서 성별에 따 른 차이는 없었다. 활성상태 환자군의 혈청 MIF 농 도는 9,959±4,817 pg/mL였고 비활성상태 환자군은 8,391±4,636 pg/mL로 활성상태 환자군에서 높은 경 향을 보였으나 통계적 유의성은 관찰되지 않았다(p=
0.251)(그림 2).
베체트병의 각각의 임상 양상과 MIF농도를 조사 한 결과 특정 임상양상과 MIF농도와의 상관 관계는 관찰되지 않았다(결과 표기하지 않음).
2. 전혈 세포 배양 후 MIF
베체트병 환자(6명)의 전혈 세포배양 후 MIF 농도 는 자극을 가하지 않은 경우 1,113±435 pg/mL였고, Con A 10μg/mL로 자극한 경우 2349±858 pg/ml로 자극 시 MIF 농도가 유의하게 증가하였다(p<0.05).
정상 대조군(5명)의 전혈 세포배양 후 MIF 농도는 자극하지 않은 경우 581±192 pg/mL였고, Con A 10 μg/mL로 자극한 경우 1,238±353 pg/ml로 자극 시 MIF 농도가 유의하게 증가하였으며(p<0.05), 전혈
Fig. 1. Serum levels of MIF were higher in patients with Behcet's disease than in healthy controls (8,777±4712 vs 665±329 pg/mL, p<0.001, independent Student's t-test).
Fig. 2. Serum level of MIF tended to be higher in patients with Behcet's disease in active state than inactive state, but did not reach statistical significance (9,959±4,817 vs. 8,391±4,636 pg/mL, p=0.251, independent Student's t-test).
Fig. 3. The MIF production by Con A-stimulated peri- pheral blood cell culture was higher in patients with Behcet's disease than in healthy controls (p<0.05, independent Student's t-test, paired t-test).
세포 배양 후 자극하지 않은 경우나 Con A로 자극 한 경우 모두, 환자군에서 정상 대조군에 비해 MIF 농도가 유의하게 높았다(p< 0.05)(그림 3).
3. 각 환자에서 시간에 따른 질병 활성도의 변화에 따른 혈청 MIF 농도의 변동
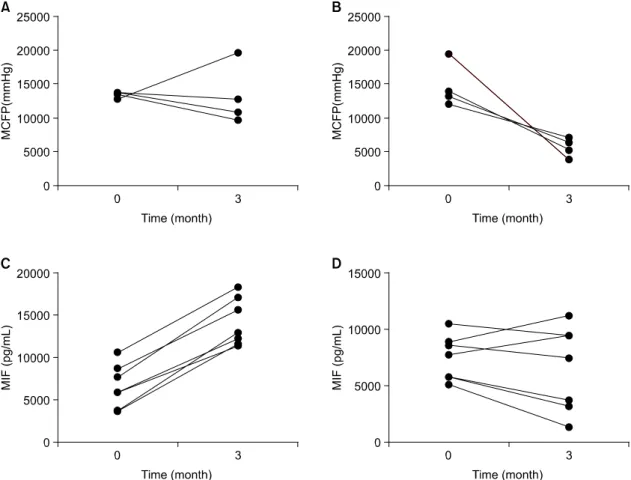
활성화상태에서 활성화상태로 질병활성도의 변화 가 없는 4명의 환자에서 13,398±496 pg/mL에서 13,240±4,464 pg/mL로 혈청 MIF 농도가 변동이 없 었고(p=0.486)(그림 4A) 활성화상태에서 비활성화상 태로 질병활성도의 변화가 있는 4명의 환자에서 14,661±3,280 pg/mL에서 5,610±1,413 pg/mL로 혈청 MIF 농도가 유의하게 감소하였고(p<0.05)(그림 4B) 비활성화상태에서 활성화상태로 질병활성도의 변화
가 있는 7명의 환자에서 6,571±2,560 pg/mL에서 14,156±2,802 pg/mL로 혈청 MIF 농도가 유의하게 증가하였으며(p<0.05)(그림 4C) 비활성화상태에서 비 활성화상태로 질병활성도의 변화가 없는 7명의 환자 에서 7,467±1,993 pg/mL에서 6,530±3,778 pg/mL로 혈청 MIF 농도가 변동이 없었다(p= 0.805)(그림 4D).
고 찰
베체트병의 병인에는 단핵구, T세포, 중성구 등이 활성화되고 여러 가지 시토카인들이 관여한다고 알 려져 있으며 여기에는 종양괴사인자, 인터루킨 8, 인 터루킨 12, 인터루킨 17, 감마인터페론 등이 포함된 다1). 특히 이 중에서 인터루킨 8은 질병 활성도를
Fig. 4. Serum levels of MIF were changed in each patient with Behcet's disease according to clinical disease activity such as, active to active state (A, p=0.486), active to inactive (B, p<0.05), inactive to active state (C, p<0.05) and inactive to inactive state (D, p=0.805) (Mann-Whitney test).
나타내는 시토카인으로 알려져 있다20). 그외에도 활 성화된 상태에서 종양괴사인자, 인터루킨-6, 인터루 킨-10, 인터루킨-17, 인터루킨-18, 인터페론 감마가 증가된다고 보고하였다21,22).
MIF는 여러 가지 염증이나 면역 반응에 중요한 역할을 하는 시토카인으로, 류마티스 질환에서는 류 마티스관절염에서 MIF의 역할이 많이 연구되었다.
류마티스관절염의 질병 활성도를 나타내는 C-반응성 단백질 수치와 활막 MIF 농도와 양의 상관성을 보 였고 동일한 환자에서 활성화된 상태에서는 활막 MIF 농도가 증가되었다가 치료 후에는 감소하여 MIF가 류마티스 관절염의 임상적 발현 및 활성화에 중요한 역할을 함을 증명하였다14). 또한 시험관내에 서 MIF가 대식세포를 자극하여 종양 괴사 인자, 인 터루킨 1, 인터루킨 6, 인터루킨 8을 포함하는 류마 티스관절염에서 이미 알려져 있는 여러 가지 시토카 인의 분비를 자극하고23,24), 시토카인 발현과 염증성 효과 분자의 조절 및 관절 손상에 관여하는 것으로 알려지면서 면역 매개성 염증 질환에 있어서 MIF 가 중요한 역할을 하는 것으로 제시되고 있다12). MIF는 여러 가지 염증유발성 시토카인인 종양괴사 인자, 인터루킨-1, 인터루킨-6, 인터루킨-8 등의 분비 를 촉진하는 것으로 알려져 있어 베체트병에서 MIF 의 발현 정도를 알아보는 것이 베체트병의 병인에 중요한 의미를 가질 것으로 생각된다. 이에 저자들 은 베체트병 환자에서 혈청과 말초혈액 세포배양 상 층액에서 MIF 농도를 알아보았다. 베체트병 환자는 정상인보다 혈청 MIF가 유의하게 높았고 특히 활성 상태와 안정상태 환자 모두에서 혈청 MIF가 정상 대조군보다 높았다. MIF 농도는 환자군, 정상 대조 군 모두 남녀에 따른 차이가 없어 비록 환자군에서 정상인에 비해 여자의 숫자가 많았으나 환자군의 MIF 농도 증가와 상관관계는 없을 것으로 생각된다.
또한 혈청 MIF 농도는 질병 활성도에 따라 변화하 였다. 활성기의 환자가 비활성상태의 환자보다 혈청 MIF는 증가된 경향을 보였으나 통계적으로는 의미 있는 차이가 없었으나, 각각의 환자에서 시간변동에 따라 질병 활성도의 변화에 따른 혈청 MIF 수치가 변하여 질병 활성도를 반영하였다. 이는 Con A 자 극에 따른 MIF의 생산능 증가가 베체트병 환자에서 증가되어 있는 사실과 더불어 혈청 내 MIF의 증가
가 베체트병의 염증반응의 진행에 중요한 역할을 함 을 시사하며, 혈청 MIF가 질병 활성도의 지표로서의 가능성을 시사해준다. 베체트병에서 MIF를 분비하는 세포와 MIF의 분비를 조절하는 인자 및 그 신호 전 달체계에 대해서는 앞으로 더 많은 연구가 필요할 것으로 생각된다.
결 론
본 연구의 결과, 혈청 MIF농도가 베체트병에서 증 가되어 있고 베체트병의 병인에서의 면역반응에 관 여할 것으로 생각된다. 또한 혈청 MIF가 질병 활성 도의 지표로서의 가능성을 시사해준다. 향후 베체트 병에서 MIF가 증가되는 기전과 MIF의 기능 및 MIF 를 분비하는 세포에 대한 더 많은 연구가 필요할 것 으로 생각되며 이는 베체트병의 발병기전을 밝히는 데 많은 기여를 하며 베체트병에서 항 MIF 치료의 가능성을 제시할 것으로 기대된다.
REFERENCES
1) Hirohata S, Kikuchi H. Behcet's disease. Arthritis Res Ther 2003;5:139-46.
2) Direskeneli H. Behcet's disease: infectious aetiolo- gy, new autoantigens, and HLA-B51. Ann Rheum Dis 2001;60:996-1002.
3) David JR. Delayed hypersensitivity in vitro: its me- diation by cell free substances formed by lym- phoid cell-antigen interaction. Pathology 1966;56:
72-7.
4) Nathan CF, Karnovsky ML, David JR. Alterations of macrophage functions by mediator from lym- phocytes. J Exp Med 1971;133:1356-76.
5) Bloom BR, Bennet B. Mechanism of a reaction in vitro associated with delayed hypersensitivity. Sci- ence 1966;153:80-2.
6) Shimizu T, Ohkawara A, Nishihira J, Sakamoto W. Identification of macrophage migration inhibi- tory factor (MIF) in human skin and its immuno- histochemical localization. FEBS Lett 1996;381:
199-202.
7) Matsuda A, Tagawa Y, Matsuda H, Nishihira J.
Identification and immunohistochemical localization of macrophage migration inhibitory factor in hu-
man cornea. FEBS Lett 1996;385:225-8.
8) Onodera S, Suzuki K, MatsunoT, Kaneda K, Kuri- yama T, Nishihira J. Identification of macrophage migration inhibitory factor in murine neonatal calvariae and osteoblasts. Immunology 1996;89:
430-5.
9) Bacher M, Metz CN, Calandra T, Mayer K, Che- sney J, Lohoff M, et al. An essential role for macrophage migration inhibitor factor in T-cell acti- vation. Proc Natl Acad Sci USA 1996;93:7848-54.
10) Lolis E. Glucocorticoid counter regulation: macro- phage migration inhibitory factor as a target for drug discovery. Curr Opin Pharmacol 2001;1:662-8.
11) Calandra T, Bernhagen J, Metz CN, Spiegel LA, Bacher M, Donelly T, et al. MIF as a glucoco- rticoid-induced modulator of cytokine production.
Nature 1995;377:68-71.
12) Morand EF, Bucala R, Leech M. Macrophage mig- ration inhibitory factor: an emerging therapeutic tar- get in rheumatoid arthritis. Arthritis Rheum 2003;
48:291-9.
13) Leech M, Metz C, Hall P, Hutchinson P, Gianis K, Smith M, et al. Macrophage migration inhi- bitory factor in rheumatoid arthritis: evidence of proinflammatory function and regulation by gluco- corticoids. Arthritis Rheum 1999;42:1601-8.
14) Morand EF, Leech M, Weedon H, Metz C, Bucala R, Smith MD. Macrophage migration inhibitory fac- tor in rheumatoid arthritis: clinical correlations.
Rheumatology 2002;41:558-62.
15) Selvi E, Tripodi SA, Catenaccio M, Lorenzini S, Chindamo D, Manganelli S, et al. Expression of macrophage migration inhibitory factor in diffuse systemic sclerosis. Ann Rheum Dis 2003;62:460-4.
16) Meazza C, Travaglino P, Pignatti P, Magni- Manzoni S, Ravelli A, Martini A, et al. Macro- phage migration inhibitory factor in patients with
juvenile idiopathic arthritis. Arthritis Rheum 2002;
46:232-7.
17) Kotake S, Kitaichi N, Ohno S. Macrophage migra- tion inhibitory factor in uveitis. Int Ophthalmol Clin 2002;42:99-103.
18) Niino M, Ogata A, Kikuchi S, Tashiro K, Nishi- hira J. Macrophage migration inhibitory factor in the cerebrospinal fluid of patients with conven- tional and optic-spinal forms of multiple sclerosis and neuro-Behcet's disease. J Neurol Sci 2000;
179:127-31.
19) International Study Group for Behet's Disease. Cri- teria for diagnosis for Behet's disease. Lancet 1990;
335;1078-80.
20) Katsantonis J, Adler Y, Orfanos CE, Zouboulis CC. Adamantiades-Behcet's disease: serum IL-8 is a more reliable marker for disease activity than C-reactive protein and erythrocyte sedimentation rate. Dermatology 2000;201:37-9.
21) Hamzaoui K, Hamzaoui A, Guemira F, Bessioud M, Hamza M, Ayed K. Cytokine profile in Beh- cet's disease patients. Relationship with disease activity. Scand J Rheumatol 2002;31:205-10.
22) Evereklioglu C, Er H, Turkoz Y, Cekmen M.
Serum levels of TNF-alpha, sIL-2R, IL-6, and IL- 8 are increased and associated with elevated lipid peroxidation in patients with Behcet's disease.
Mediators Inflamm 2002;11:87-93.
23) Calandra T, Bernhagen J, Metz CN, Spiegel LA, Bacher M, Donnelly T, et al. MIF as a glucoco- rticoid-induced modulator of cytokine production.
Nature 1995;377:68-71.
24) Donnelly SC, Haslett C, Reid PT, Grant IS, Wal- lace WAH, Metz CN, et al. Regulatory role for macrophage migration inhibitory factor in acute res- piratory distress syndrome. Nat Med 1997;3:320-3.