The Importance of Breast Elastography Added to the BI-RADS
Ⓡ(5
thEdition) Lexicon Classification
Alvinlyle Kim, Chang Wan Jun, Dong Won Ryu
Department of Surgical, Kosin University Gospel Hospital, Busan, Korea
Received October 10, 2016 Revised October 23, 2016 Accepted October 28, 2016
Purpose: This study was conducted to investigate the addition of elastography to the BI-RADSⓇ lexicon for the classification of breast lesions.
Methods: A total of 301 patients diagnosed with breast lesions from January 2015 to September 2015 were included in our study. Acoustic radiation force impulse (ARFI) elas- tography and strain ratio (SR) evaluations were performed on 301 lesions. We compared the diagnostic performance of breast ultrasonography alone and the combination of breast ul- trasonography, ARFI elastography, and SR evaluations. The patients were classified accord- ing to the fifth edition of the breast imaging and reporting data system (BI-RADS) lexicon, which includes elastographic findings.
Results: Among the 301 lesions, 38 were malignant and 263 were benign. The addition of elastographic findings to the BI-RADS lexicon improved the sensitivity, specificity, and diag- nostic accuracy of ultrasound during assessment of breast lesions, which increased from 94.7, 66.7, and 70.4 to 92.1, 88.5 and 89.3%, respectively.
Conclusion: These findings suggest that the addition of elastography to the 4th BI-RADS lex- icon will improve the specificity and diagnostic accuracy of ultrasonography in the screening of breast lesions. Therefore, ARFI elastography and SR evaluations can be used as comple- mentary modalities to make more accurate breast lesion diagnoses.
Keywords: Breast neoplasms, Ultrasonography, Elastography, Specificity, Accuracy Correspondence to:
Dong Won Ryu
Department of Surgery, Kosin University Gospel Hospital, 262 Gamcheonro, Seo-gu, Busan 49267, Korea
Tel: +82-51-990-6462 Fax: +82-51-246-6093 E-mail: [email protected]
INTRODUCTION
Breast cancer is the most frequent cancer among women worldwide and the second most common can- cer in Korean women.(1) Early detection is critical for the successful man-agement of breast cancer.
B-mode ultrasonography has been used to accurately estimate breast lesion whether it is malignant or not.(2) While breast ultrasonography can be a useful method to differentiate breast lesions, this modality has the unavoidable limitation of low specificity re- ported about 87.7%.(3) To overcome this limitation,
elastography was introduced.(4) The fifth edition of the breast imaging and reporting data system (BI-RADS), an ultrasound atlas, was updated to in- clude the assessment of the elasticity of breast le- sions using elastography. Elastography was devel- oped as an additional tool for ultrasound studies in the 1990s.(5) The first corresponding clinical studies were conducted in the early 2000s, and elastography was eventually included in the latest edition of the BI-RADS lexicon.(6) The addition of elastography to the lexicon aimed to improve the specificity of ultra- sound, because low specificity is currently a major
ORIGINAL ARTICLE
J Surg Ultrasound 2016;3:46-52
JSU
Journal of Surgical Ultrasoundbarrier to the wide application of ultrasound in clin- ical practice.(7) Our study assessed the elasticity of breast lesions, using elastography combined with conventional findings that are suggested in the BI-RADS lexicon.(8) In addition, Our study inves- tigated the impact of elastography in routine testingElastography is a noninvasive imaging mo- dality to evaluate the stiffness of soft tissues. In general, benign breast lesions tend to be softer than malignant lesions.(9) This general characteristic provides the basis for using elastography to differ- entiate breast lesions.(10) The most frequently used elastography technique in the breast is strain elas- tography, which requires external compression.(11) Because external compression is performed man- ually, strain elastography is operator-dependent which influences its reproducibility. Instead of using manual compression, a new trend of applying acous- tic radiation force impulse (ARFI) imaging to elas- tography has arisen. ARFI elastography has the ad- vantage of being objective, reproducible, and less operator-dependent.(12) With this modality, ultra- sonography scanners are used to generate short-du- ration acoustic radiation forces that impart small, localized displacements in the tissue and create a static map of the relative stiffness of the tissues.(13) Strain ratio (SR) is a semiquantitative measurement to determine the firmness of tissue and to differ- entiate benign and malignant lesions by comparing the difference in compliance between a breast lesion and adjacent fatty tissue.(14) Previous studies have proven that SR is a highly valuable and more ob- jective parameter for differentiating malignant and benign breast lesions.(15) The aim of this study was to evaluate whether the combination of breast ultra- sonography, ARFI elastography, and SR improves the diagnostic performance of differentiating malignant and benign breast lesions.
METHODS
1. Patients
Between January and September 2015, patients who visited to the outpatient clinic for breast mass, pain and screening study were evaluated. So Total of 301 lesions with breast lesions was included in our study. Regardless of the ultrasonographic findings, each lesion in the study underwent a histological ex- amination with the consent of the patient. In patients with benign lesions diagnosed by core needle biopsy, an excisional biopsy was subsequently per-formed when the patient opted for surgical removal. Breast ultrasonography, ARFI elastography, and SR exami- nations were performed before surgery and biopsy.
After the radiologic examinations, each breast lesion was diagnosed pathologically by radical surgery (38/301, 12.6%), excisional biopsy (5/301, 1.6%), or vacuum-assisted breast biopsy (258/301, 85.7%).
2. Imaging techniques
Breast ultrasonography, ARFI elastography, and SR evaluations were performed with a Siemens ACUSON S2000 US system (Siemens Medical Solutions, Mountain View, USA) with a linear probe (9L4;
Siemens Medical Solutions) by one operator with 9 years’ experience in breast imaging. First, we ob- tained breast ultrasonographic images of the lesions.
The lesion was described by using the BI-RADS lex- icon of ultrasonographic descriptors of mass shape, orientation, margin, lesion boundary, echo pattern, and posterior acoustic features. Next, ARFI elastog- raphy sequences were performed to evaluate the elasticity scores of the breast lesions in Virtual TouchTM imaging (VTI) mode by displaying the target lesion on breast ultrasonography, setting a region of interest (ROI) around the lesion, and ensuring that adequate surrounding breast tissue was included in the ROI. During the ARFI elastography examination, patients were instructed to continue breathing
normally. In Virtual TouchTM quantification (VTQ) mode, an acoustic impulse and detection pulses were used to calculate shear wave velocity (SWV). To per- form VTQ, a target region was identified with a fixed-size ROI of 5 × 5 mm. For the measurement, the marginal areas of the mass and surrounding tis- sues were included in the ROI, and the SWV was measured 3 times in these areas when measurements were feasible. The shear waves were detected by ul- trasonographic detection pulses; numeric SWV val- ues were calculated and displayed on the monitor.
When measurements were outside the allowable range (0-9 m/sec) for SWV calculations, the SWV might be displayed as “X.XX.” The SR was meas- ured on a static image including coupled B-mode and elastographic images. The calculation of the SR was based on a comparison of the average strain meas- ured in the lesion and adjacent fatty tissue at the same depth. The strain of the lesion was determined by selecting an ROI from the lesion. The SR was au- tomatically calculated and displayed on the monitor.
3. Image analysis
Breast ultrasonography images were assigned to 1 of 5 categories according to BI-RADS: category 1, negative findings; category 2, benign findings; cat- egory 3, probably benign findings; category 4, sus- picious of malignancy; and category 5, highly sug- gestive of malignancy. To classify VTI-mode images, we evaluated the color-mapped pattern both in the lesion and in the surrounding breast tissue (i.e., the pectoral muscle and rib were excluded). The ARFI elastography image was displayed as a color map with each voxel representing the degree of strain within the ROI by using a scale ranging from purple (softest components) to blue (intermediate components) and red (hardest components). The lesions were first classified according to the 4th edition of BI-RADS lexicon and, then, classified based on the elasto- graphic findings according to the 5th edition of
BI-RADS lexicon. The masses were classified ac- cording to the BI-RADS lexicon criteria. And then using the elastographic criteria, the lesions were classified as soft, intermediate, or hard. The techni- ques that were used in the elastographic classi- fication have been previously described. The final classification of the lesions was based on the BI-RADS ultrasound assessment categories and the elastographic findings. The positive predictive value, negative predictive value, sensitivity, specificity, and diagnostic accuracy of the BI-RADS classi- fication, with and without the elastographic data, were determined and compared.
4. Statistical analysis
All statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, USA). Differences in sensitivity, specificity, accuracy, positive pre- dictive value, and negative predictive value between evaluation methods were assessed by Student t-test.
The mean SWV and SR values were calculated using ANOVA. A P-value of < 0.05 was considered to in- dicate statistical significance.
RESULTS
1. Pathologic diagnosis
Of the 301 lesions, 38 (12.6%) were malignant and 263 (87.3%) were benign. The pathologic diagnoses of these lesions are shown in Table 1. The most common malignant and benign tumors were invasive ductal carcinoma (n = 34) and fibrocystic changes (n = 257), respectively.
2. ARFI elastography and SR for breast lesions Distributions of elasticity scores according to pathologic diagnosis when ARFI elastography was displayed in VTI mode are shown in Table 2 and Table 3. The hard elasticity score was significantly higher for malignant lesions (55.3%) than for benign lesions
Table 2. The Distribution of Elasticity Scores in Benign Breast Lesions Elasticity score in
benign lesions
The number of
lesions Rate
Soft 228 86.7%
Intermediate 19 7.2%
Hard 13 5.0%
Missed date 3 1.1%
Total 263 100%
Table 3. The Distribution of Elasticity Scores in Malignant Breast Lesions
Elasticity Score in Malignant lesions
The number of
lesions Rate
Soft 13 34.2%
Intermediate 4 10.5%
Hard 21 55.3%
Total 38 100%
Table 1. Pathologic Diagnosis of the Examined Malignant and Benign Breast Lesions
Pathologic diagnosis Number of lesions (%) in 301 patients Malignant (n = 38)
Invasive ductal carcinoma 34 (89.4%) Invasive lobular carcinoma 1 (0.3%) Ductal carcinoma in situ 3 (1.0%) Benign (n = 263)
Fibrocystic disease 257 (97.7%)
Hyperplastic disease 1 (0.3%)
Intraductal papilloma 3 (1.1%) Atypical ductal hyperplasia 2 (0.7%)
Table 4. Comparison of Elasticity Scores According to Pathologic Diagnosis
Malignant No. (%)
Benign No. (%)
Total
No. (%) P-value
Elasticity score 0.001
Soft 13 (34.2) 228 (86.7) 241 (80.1) Intermediate 4 (10.5) 19 (7.2) 23 (7.6) Hard 21 (55.3) 13 (5.0) 34 (11.3) Total 38 (100) 263 (100)
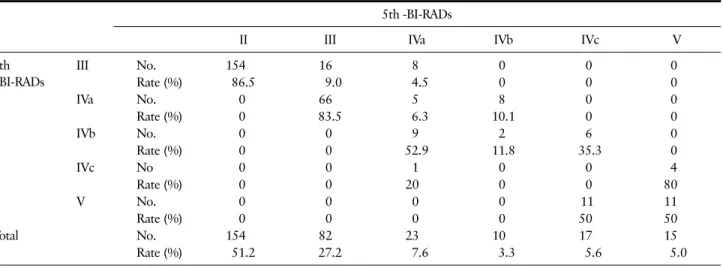
Table 5. The 5th BI-RADSⓇ Classification of Breast Lesions After the Addition of Elastographic Findings to the 4th BI-RADSⓇ Classification 5th -BI-RADs
II III IVa IVb IVc V
4th BI-RADs
III No. 154 16 8 0 0 0
Rate (%) 86.5 9.0 4.5 0 0 0
IVa No. 0 66 5 8 0 0
Rate (%) 0 83.5 6.3 10.1 0 0
IVb No. 0 0 9 2 6 0
Rate (%) 0 0 52.9 11.8 35.3 0
IVc No 0 0 1 0 0 4
Rate (%) 0 0 20 0 0 80
V No. 0 0 0 0 11 11
Rate (%) 0 0 0 0 50 50
Total No. 154 82 23 10 17 15
Rate (%) 51.2 27.2 7.6 3.3 5.6 5.0
(5.0%) (Table 4). Of the 38 malignant lesions, 21 (55.3%) lesions had a hard elasticity scores. In this group, 13 lesions (34.2%) had a soft elasticity scores.
Of the 263 benign lesions, 228 (86.7%) had a soft elasticity scores. 19 lesions (7.2%) had a intermediate elasticity scores. There was a high correlation be- tween elasticity score and malignancy (P = 0.001)
(Table 4). In VTQ mode, the mean SWV value of be- nign lesions (1.22 ± 0.88 m/sec) was lower than that of malignant lesions (2.54 ± 1.09 m/sec, P < 0.01).
The SWV cutoff point for malignant lesions was esti- mated as 2.37 m/sec. The mean SR value of benign lesions (1.54 ± 1.40) was significantly lower than that of malignant lesions (3.42 ± 1.63, P < 0.001).
Table 6. Frequency of the 4th BI-RADSⓇ Categories for the Lesions that were Classified Without (BI-RADSⓇ) Elastographic Findings
4th BI-RADs III 4th BI-RADs IV 4th BI-RADs V
True positive 16 (15.8%) 20 (90.9%)
True negative 176 (98.8%)
False positive 85 (84.2%) 2 (9.1%)
False negative 2 (1.1%)
Total N 178 101 22
PPV 15.8% 90.9%
NPV 98.8%
Sensitivity 94.7%
Specificity 66.9%
Accuracy 70.4%
PPV = positive predictive value; NPV = the negative predictive value.
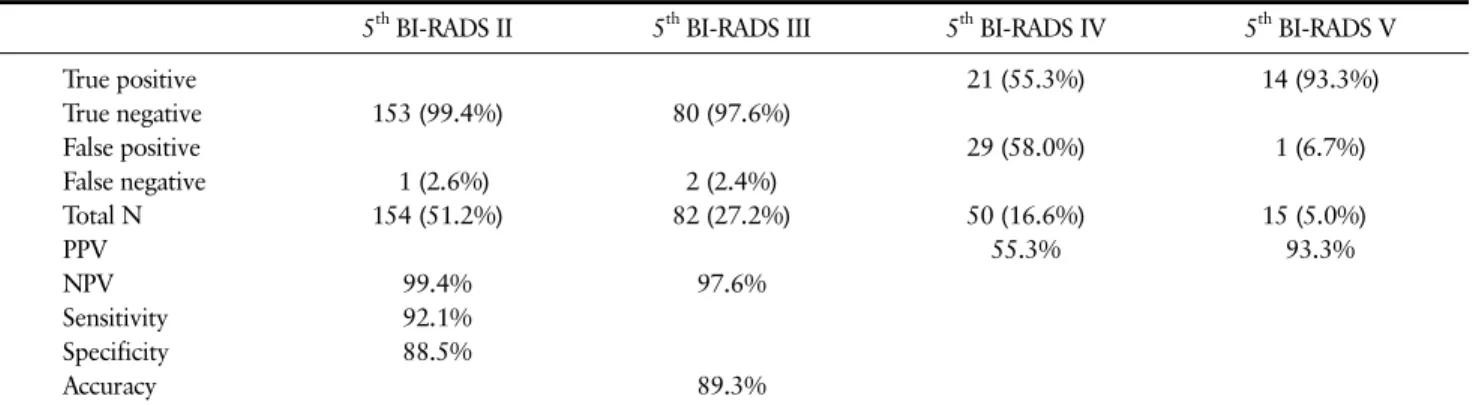
Table 7. Frequency of the 5th BI-RADSⓇcategories for the lesions that were classified with (BI-RADSⓇ Elastography)
5th BI-RADS II 5th BI-RADS III 5th BI-RADS IV 5th BI-RADS V
True positive 21 (55.3%) 14 (93.3%)
True negative 153 (99.4%) 80 (97.6%)
False positive 29 (58.0%) 1 (6.7%)
False negative 1 (2.6%) 2 (2.4%)
Total N 154 (51.2%) 82 (27.2%) 50 (16.6%) 15 (5.0%)
PPV 55.3% 93.3%
NPV 99.4% 97.6%
Sensitivity 92.1%
Specificity 88.5%
Accuracy 89.3%
PPV = Positive predictive value; NPV = The negative predictive value.
3. Diagnostic performance of BUS alone and a combination of BUS, ARFI elastography, and SR evaluations for breast lesions
Table 5 shows the comparison of the number of breast lesions in each 4th edition and 5th edition of BI-RADS lexicon. Among the 79 lesions with the 4th edition of BI-RADS score of 4a, 66 cases (83.5%) were adjusted to 5th edition of BI-RADS score of 3 and 8 cases (10.1%) were re-categorized as a 5th edi- tion of BI-RADS score of 4b. And among the 178 le- sions with the 4th edition of BI-RADSⓇ score of 3, 8 cases (4.5%) were adjusted to 5th edition of BI-RADSⓇ score of 4a (Table 5). According to 4th edition of BI-RADS lexicon, Breast ultrasonography showed
94.7% sensitivity, 66.9% specificity, 70.4% accuracy, a 15.8% positive prediction value, and a 98.8% neg- ative prediction value for malignant lesions (Table 6).
In the same way, according to 5th edition of BI-RADS lexicon, Breast ultrasonography presented 92.1%
sensitivity, 88.5% specificity, 89.3% accuracy, 53.3%
positive prediction value, and a 99.4% negative pre- diction value for differentiating breast lesions (Table 7). The specificity, accuracy, and PPV of breast ul- trasonography combined with ARFI elastography and SR were higher than those of breast ultrasonography alone.
DISCUSSION
The introduction of elastographic findings into the BI-RADS lexicon serves as an additional tool to im- prove the specificity and diagnostic accuracy of ul- trasound in the screening of breast lesions.(5) The low specificity of current ultrasound techniques has led to a large number of false positive results, which often necessitate diagnostic biopsies. The low spe- cificity of ultrasound hinders its use in the routine diagnostic screening of breast lesions.(16)
Elastography requires the coupling of specific software and an ultrasound device to assess the soft- ness of tissue in areas of interest.(17) This method is based on the assumption that benign lesions tend to
be softer than malignant lesions.(18) Elastography software is currently included in most commercial ultrasound devices; however, this software has not been standardized.(19) This software may be used for a qualitative assessment of lesions, which is based on the visual evaluation of changes in color in the area of interest; however, this type of assessment is subjective.(20) In a quantitative assessment, the de- gree of hardness in a lesion is estimated using ob- jective data. Compressions to induce the required deformation may be performed manually or using specific probes, such as ARFI and shear-wave imaging.(21) Even with the introduction of these new technologies, there seems to be a convergence in the literature to adopt the qualitative criteria for the evaluation of breast masses as a standard, rather than quantitative criteria.(22) The reason for this is that ultrasound is, in essence, a sub-jective method of image interpretation, which depends on the expe- rience and training of the examiner.(18) Lesions deeper than 2 cm are less accurately characterized by means of shear-wave elastography. The latest edi- tion of the BI-RADS atlas includes elastographic findings, and lesions are classified as soft, inter- mediate, or hard. Fibroadenomas include both soft and hard lesions. It was observed that the most in- dolent fibroadenomas (hypocellular with collagen) appeared softer on elastographic assessment, whereas the complex and hypercellular lesions were harder.
Elastography allows for an unequivocal diagnosis in complicated cysts. Because of the inclusion of elas- tographic data in the BI-RADS lexicon, in this study, a large number of lesions that would have been clas- sified as BI-RADS category 3 (most likely benign and soft) were reclassified as BI-RADS category 2 (benign). Elastography may impact lesions that are classified as BI-RADS category 4a, which include le- sions that meet most of the criteria for benign le- sions, but would benefit from further investigation with diagnostic methods or short-term follow-up.
The classification of soft lesions would shift from category 4a to category 3, for which short-term fol- low-up (usually 6 months) is recommended. The risk of malignancy in lesions that are classified in the BI-RADS lexicon as category 4a varies from 2-10%.
CONCLUSION
The results of this study demonstrate that the use of elastography as recommended in the latest edition of the BI-RADSⓇ lexicon improved the specificity and accuracy of ultrasonography, which increased from 66.7 to 88.5% and from 70.4 to 89.3%, respectively.
The sensitivity of this method did not significantly changes from 94.7 to 92.1%. But this study was con- ducted at a single center for patients with breast lesions. So Further studies needed to validate the results. The use of elastographic findings according to the recommendations in the 5th edition of the BI-RADSⓇ lexicon may improve the specificity and diagnositic accuracy of breast ulatrasonography in the screening of breast cancer.
ACKNOWLEDGEMENTS
This article is presented in 67th congress of the Korean Surgical Society. This article was supported by Kosin Medical colleage.
REFERENCES
1. Min SY, Kim Z, Hur MH, Yoon CS, Park EH, Jung KW.
The basic facts of Korean breast cancer in 2013: re- sults of a nationwide survey and breast cancer regis- try database. J Breast Cancer 2016;19:1-7.
2. Fausto A, Rubello D, Carboni A, Mastellari P, Chon- drogiannis S, Volterrani L. Clinical value of relative quantification ultrasound elastography in character- izing breast tumors. Biomed Pharmacother 2015;75:
88-92.
3. Ohuchi N, Suzuki A, Sobue T, Kawai M, Yamamoto S, Zheng YF, et al. Sensitivity and specificity of mam- mography and adjunctive ultrasonography to screen
for breast cancer in the Japan Strategic Anti-cancer Randomized Trial (J-START): a randomised con- trolled trial. Lancet 2016;387:341-8.
4. Kuehlmann B, Prantl L, Michael Jung E. Imaging of idle breast implants with ultrasound-strain elastog- raphy- A first experimental study to establish cri- teria for accurate imaging of idle implants via ultra- sound-strain elastography. Clin Hemorheol Microcirc 2016;61:645-56.
5. Fleury Ede F. The importance of breast elastography added to the BI-RADSⓇ (5th edition) lexicon classi- fication. Rev Assoc Med Bras (1992) 2015;61:313-6.
6. Botticelli A, Mazzotti E, Di Stefano D, Petrocelli V, Mazzuca F, La Torre M, et al. Positive impact of elas- tography in breast cancer diagnosis: an institutional experience. J Ultrasound 2015;18:321-7.
7. Kim SJ, Ko KH, Jung HK, Kim H. Shear Wave Ela- stography: Is It a Valuable Additive Method to Con- ventional Ultrasound for the Diagnosis of Small (≤2 cm) Breast Cancer? Medicine (Baltimore) 2015;94:
e1540.
8. Skaane P. Breast elastography. Acta Radiol 2015;56:
NP46.
9. Youk JH, Son EJ, Gweon HM, Han KH, Kim JA.
Quantitative lesion-to-fat elasticity ratio measured by shear-wave elastography for breast mass: which area should be selected as the fat reference? PLoS One 2015;10:e0138074.
10. Hao SY, Ou B, Li LJ, Peng YL, Wang Y, Liu LS, et al.
Could ultrasonic elastography help the diagnosis of breast cancer with the usage of sonographic BI-RADS classification? Eur J Radiol 2015;84:2492-500.
11. Gkali CA, Chalazonitis AN, Feida E, Sotiropoulou M, Giannos A, Tsigginou A, et al. Breast elastography:
how we do it. Ultrasound Q 2015;31:255-61.
12. Carlsen J, Ewertsen C, Sletting S, Vejborg I, Schäfer FK, Cosgrove D, et al. Ultrasound elastography in breast cancer diagnosis. Ultraschall Med 2015;36:
550-62; quiz 563-5.
13. Lo CM, Chang YC, Yang YW, Huang CS, Chang RF.
Quantitative breast mass classification based on the integration of B-mode features and strain features in
elastography. Comput Biol Med 2015;64:91-100.
14. Feldmann A, Langlois C, Dewailly M, Martinez EF, Boulanger L, Kerdraon O, et al. Shear Wave Elasto- graphy (SWE): an analysis of breast lesion character- ization in 83 breast lesions. Ultrasound Med Biol 2015;41:2594-604.
15. Xian-Quan S, Jun-Lai LI, Qiu-Yang LI, Yan H, Wen-Bo W, Jie T. Performance of ultrasonic shear wave elastography in assessing benign and malignant breast lesions. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2015;37:294-9.
16. Li DD, Guo LH, Xu HX, Liu C, Xu JM, Sun LP, et al.
Acoustic radiation force impulse elastography for dif- ferentiation of malignant and benign breast lesions: a meta-analysis. Int J Clin Exp Med 2015;8:4753-61.
17. Park CS, Kim SH, Jung NY, Choi JJ, Kang BJ, Jung HS. Interobserver variability of ultrasound elastog- raphy and the ultrasound BI-RADS lexicon of breast lesions. Breast Cancer 2015;22:153-60.
18. Faruk T, Islam MK, Arefin S, Haq MZ. The journey of elastography: background, current status, and future possibilities in breast cancer diagnosis. Clin Breast Cancer 2015;15:313-24.
19. Kim MY, Choi N, Yang JH, Yoo YB, Park KS. False positive or negative results of shear-wave elastog- raphy in differentiating benign from malignant breast masses: analysis of clinical and ultrasonographic characteristics. Acta Radiol 2015;56:1155-62.
20. Barr RG, Zhang Z. Shear-wave elastography of the breast: value of a quality measure and comparison with strain elastography. Radiology 2015;275:45-53.
21. Zhang Q, Xiao Y, Chen S, Wang C, Zheng H. Quanti- fication of elastic heterogeneity using contourlet- based texture analysis in shear-wave elastography for breast tumor classification. Ultrasound Med Biol 2015;41:588-600.
22. Ganau S, Andreu FJ, Escribano F, Martín A, Tortaja- da L, Villajos M, et al. Shear-wave elastography and immunohistochemical profiles in invasive breast can- cer: evaluation of maximum and mean elasticity values. Eur J Radiol 2015;84:617-22.