In 1965, Komatsu and Tamai reported the first successful digital replantation.1 Subsequent improvement in instru- mentation and the development of microsurgical techniques have greatly increased the success of this procedure. For example, multi-segment amputation, because of its poor results, has previously been described as a contraindication for replantation.2,3 The advent of microsurgical techniques and their refinement have largely expanded the indications of digital and palmar replantation, and have, more often, enabled the salvaging of severed fingers.4 Recently, there have been reports of successful replantation of a 10-digit amputation;5,6 however, reports on replantation for a multiple segment hand amputation are few.3 We report a case of a multi-segment amputation with satisfactory function following replantation.
CASE REPORT
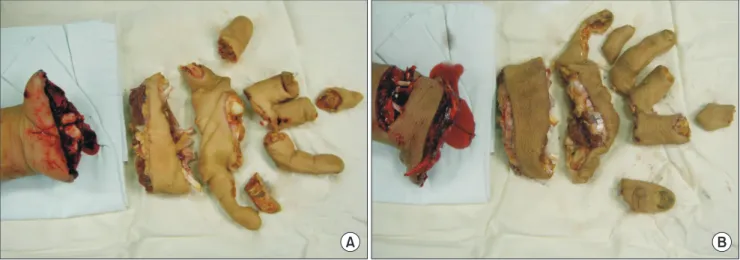
A 39-year-old man presented six hours after an accident, while using a straw cutter, that caused a multi-segment amputation of the entire palm and digits (Fig. 1). On presentation, his thumb, ring finger, and little finger were segmented into three parts; his index finger and middle finger were segmented into four parts from the 3 cm distal level to the radio-carpal joint. The most proximal segment was 2.4 cm and the second segment was 2 cm. The operation was performed from the proximal level to the distal level sequentially. For fast bone fixation, a K-wire was used for each digit. After connecting the tendons and arteries, sufficiency of circulation was confirmed; we then performed neurorrhaphy and venorrhaphy.
At the nearest level, after the ulnar and radial arteries were end-to-end anastomosed with 10-0 Ethilon sutures, the median and ulnar nerves were repaired using the epineural technique.
Replantation for Segmental Amputation of the Digits and Hand:
A Case Report
Sung Jin An, Sang Hyun Lee*, Hong Sung Min, In Hee Kim, Jeung Il Kim
Department of Orthopaedic Surgery, Pusan National University Hospital, Busan, Korea
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2016 by the Korean Society for Microsurgery. All Rights Reserved.
Received July 1, 2016 Revised July 11, 2016 Accepted July 11, 2016
*Correspondence to: Sang Hyun Lee Department of Orthopaedic Surgery, Medical Research Institute, Pusan National University Hospital, 179 Gudeok-ro, Seo- gu, Busan 49241, Korea
Tel: +82-51-240-7248 Fax: +82-51-247- 8395 E-mail: [email protected] ORCID: http://orcid.org/0000-0003-0091-4825 Financial support: None.
Conflict of interest: None.
Segmental amputation of the digits and hand has been described as a contraindication for replantation because of poor results. We report the results of replantation for a patient who experienced multi-segment amputation of the hand. A 39-year-old man presented six hours after an accident, while using a straw cutter, that caused a multi-segment amputation of the entire palm and digits. The replantation surgery took 18 hours. We observed the patient gain satisfactory function of the hand. For replantation of a multi- segment amputation, connecting as many blood vessels as possible without tension is most important.
Key Words: Segmental, Finger, Hand, Amputation, Replantation
ARMS
Archieves of Reconstructive MicrosurgeryCase Report
pISSN 2383-5257 eISSN 2288-6184 Arch Reconstr Microsurg 2016;25(2):60-64 https://doi.org/10.15596/ARMS.2016.25.2.60
Since the lengths of the amputated artery and nerve were less than 2 cm, a vessel anastomosis was performed, and inflicting little damage on the blood vessel. After the determination of sufficient blood flow, three veins were repaired on the dorsal side.
At the second level, after bone fixation with a K-wire, five palmar digital arteries and nerves were repaired. Four dorsal veins were repaired, restoring sufficient blood flow.
At the third level, keeping the blood volume of the first finger, we fixed the distal phalanx and constructed an anastomosis
with two digital arteries, one digital nerve, and two digital veins.
Because of insufficient blood flow in the other four fingers, we performed a transition replantation of the ring finger to the location of the middle finger and constructed two artery, one nerve, and two vein anastomosis (Fig. 2).
A fingertip examination showed poor arterial circulation in the middle finger of the left hand three days after replantation;
finger necrosis developed six days after the surgery (Fig. 3).
Necrotic tissue was excised four weeks after replantation, and a 10×6 cm free flap from the anterolateral thigh was grafted as the
A B
Fig. 1. A 39-year-old man working on a farm presented six hours after an accident while using a straw cutter causing multi-segment amputation, involving the whole palm and digits. His left hand was cut into four parts at three levels on the palmar side (A) and dorsal side (B). The length of the most proximal segment was 2.4 cm and the second, 2 cm. Carpal bones and several tendons were exposed. The ring finger was cut longitudinally and the most distal part of the middle finger was lost.
A B
Fig. 2. After sequential replantation from the nearest to the farthest level for 18 hours, blood circulation was well maintained. For quick bone fixation, a K-wire was used for each digit. After the connections, the tendons, arteries, nerves, and veins were repaired sequentially. The third parts of the index, middle, and ring finger were abandoned. Transition replantation was performed to the middle finger by the ring finger. On palmar side (A) and dorsal side (B).
Arch Reconstr Microsurg Vol. 25. No. 2. November 2016
secondary surgery to improve the mobility of the finger (Fig.
4). The patient had no thumb-related complications. The final assessment of the patient was made two years after replantation.
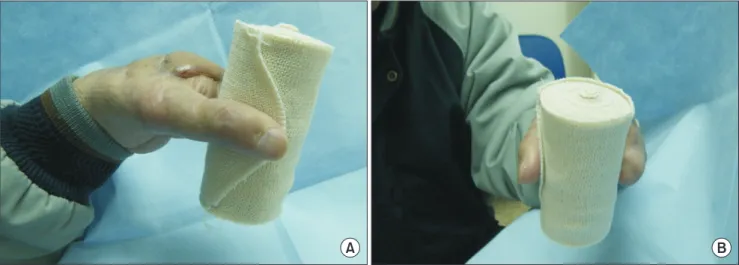
We observed that the patient gained satisfactory function of the hand; the dynamic two-point discrimination test result was 1.0 cm at the palm and 1.5 cm at the thumb. The patient did not have difficulty in performing daily activities such as holding a cylinder (Fig. 5).
DISCUSSION
There exist reports on patients who underwent successful
replantation of ten amputated fingers,5-7 but few cases of multi- segment amputation have been reported. Belsky and Ruby3 have reported successful treatment of a patient with a double level amputation through the palm and forearm. Cai et al.8 have described successful replantation of a multiple digit and circular palm amputation. Pei et al.9 classified a multi-segment hand amputation into five groups (Table 1). Our patient was classified as Type I for his multi-segment hand amputation (Table 1).
The complexity of the multi-segment amputation made the reattachment technically challenging. However, as in microsurgery, technical advancements have allowed
A B
Fig. 3. Six days after replantation: the middle finger showed poor arterial circulation and developed necrosis. (A) The skin on the palmar side of middle finger was dry and shrank. (B) On the dorsal side, more extensive necrosis developed.
A B
Fig. 4. Four weeks after replantation: the middle finger developed dry gangrene that required amputation. Necrotic tissue of middle finger was excised and 10×6 cm of free flap from anterolateral thigh was grafted onto the defected portion. The surgical wound healed without any complication.
Defatting procedures were still needed on the dorsal side (A) and the palmar side (B).
replantation surgery to become a routine procedure.3,8,9 A satisfactory functional recovery depends on several conditions:
the surgeon’s expertise, short ischemic time, sufficient functional rehabilitation, and secondary lysis of tendon adhesion.10
During the replantation of a multi-segment amputation, surgeons should consider some factors potentially affecting the results. The procedure should be determined based upon the condition of the amputated surface. For a satisfactory result, the surgeon should connect as many blood vessels as possible for sufficient blood flow. The blood flow of repaired vessels can decrease depending on the level of obstruction.10 In replantation of a multi-segment amputation, most vessels have more than one anastomotic stoma. The blockage of any anastomotic stoma can cause the necrosis of the distal end of fingers. Special attention should be paid to ensure non- traumatic suturing and operation.9 The reduction of one anastomotic stoma may help prevent the circulation crisis and shorten the operation time; adequate debridement is the key to
survival of the digits and prevention of infection.8,9 In this case, we constructed vessel anastomoses with minimal dissection due to the short length of the intermediate vessels. The first finger showed blood circulation through three anastomotic stomas, but the other fingers did not because severe crushing injury at the interphalangeal joint damaged vessel walls, which led to necrosis.
Most commonly bone fixation is perform to reduce ischemic time.4 We performed bone fixation using K-wires. Stable bone fixation is important for early rehabilitation, but early correction and continuous functional exercise of the fingers is especially important for functional recovery.8,9
Replantation should be performed for multi-segment amputation of the hands. Vascular anastomoses should be constructed without causing vascular damage, especially for multi-segment amputations. Therefore, vascular anastomoses should be made with little separation to ensure minimal blood vessel movement and prevent vessel collapse. The replantation should be performed starting from proximal one. After
Table 1. Classification of multi-segment hand amputations9
Type Involvement Level Characteristic
I Wrist, palm and digit At least three Most severe
Require the highest technical proficiency
II Wrist and palm At least two Secondary severe
III Palm and digit(s) At least two
IV Only palm At least two
V Only digits At least two
A B
Fig. 5. (A, B) Two years after replantation: the final assessment of the patient was made; he could hold a cylinder without any difficulty. The patient did not have difficulty in performing daily activities.
Arch Reconstr Microsurg Vol. 25. No. 2. November 2016
checking the volume of each blood vessel, the surgeon should perform the surgeries one by one. A good result can be obtained by linking the blood vessels, as many as possible, for smooth blood flow.
REFERENCES
1. Masuhara K, Tamai S, Fukunishi H, Obama K, Komatsu S.
Experience with reanastomosis of the amputated thumb. Seikei Geka 1967;18:403-4.
2. Casal D, Gomez MM, Antunes P, Candeias H, Almeida MA.
Defying standard criteria for digital replantation: a case series.
Int J Surg Case Rep 2013;4:597-602.
3. Belsky MR, Ruby LK. Double level amputation: should it be replanted? J Reconstr Microsurg 1986;2:159-62.
4. Beris AE, Lykissas MG, Korompilias AV, Mitsionis GI, Vekris
MD, Kostas-Agnantis IP. Digit and hand replantation. Arch Orthop Trauma Surg 2010;130:1141-7.
5. Kantarci U, Cepel S, Buldu H. Successful replantation in ten- digit amputation. Acta Orthop Traumatol Turc 2010;44:76-8.
6. Qing-tai L, Chang-qing JZ, Ke-fei Y, Sha-ling C, Jan L, Zun-ying L. Successful replantation in 10-digit complete amputations.
Plast Reconstr Surg 1996;98:348-53.
7. Baek SM, Kim SS. Ten-digit and nine-digit replantation (4 cases). Br J Plast Surg 1992;45:407-12.
8. Cai J, Cao X, Pan J, Hu J. Replantation of a multiple digit and circular palm amputation: a case report. Microsurgery 1993;14:221-4.
9. Pei GX, Zhao DS, Xie CP, Wang ST. Replantation of multi-level hand severances. Injury 1998;29:357-61.
10. Lassaline JV, Moon BC. A computational fluid dynamics simulation study of coronary blood flow affected by graft placement. Interact Cardiovasc Thorac Surg 2014;19:16-20.