Introduction
Liver cancer is the second most common cause of cancer- related deaths worldwide and the five-year survival of pa- tients with liver cancer is less than 18%.1) One of the barriers to reducing mortality of liver cancer is the late detection of most cases and the lack of treatment options for individuals with advanced stage disease. Patients with very early or early stage of liver cancer have multiple treatment options, includ- ing surgical resection, liver transplantation and loco-regional therapies with five-year survival between 50–75%. Therefore early identification of liver cancer is the key to reduce its mor- tality.2) Current guidelines by various gastroenterology and hepatology societies recommend surveillance of high risk groups using ultrasound (US) and alpha-fetoprotein (AFP) with the goal of detecting small lesions while curative options are still possible.3-5)
Because of the high prevalence of hepatitis B virus (HBV) in- fection and related liver problems in Korea, the Korean gov- ernment has made major efforts to reduce the burden of these problems. As one of the efforts, the National Liver Cancer
Surveillance Program (NLCSP) was implemented in 2003.
The target population for the surveillance included all indi- viduals 40 years and older, within which there was a high-risk group of patients with liver cirrhosis, carriers of HBV or hep- atitis C virus (HCV), or HBV- or HCV-induced chronic hep- atitis.6,7) Despite a nationwide surveillance programs are only implemented in Asian countries including Korea, Japan, and Taiwan, little is known regarding the variability in the sur- veillance adherence and diagnostic value in real surveillance program circumstance. As there is a lack of evidence for sur- veillance for liver cancer in Korea and Asian countries, this study aimed to assess the status of surveillance by determin- ing the proportion of cases for which the surveillance of liver cancer was undertaken in patients with HBV, HCV or cirrho- sis and identify factors that predict whether surveillance and diagnostic accuracy in real life surveillance practice in Korea.
Methods
Data sources
This study used health insurance claims data and NLCSP
J Health Tech Assess 2017;5(2):102-107 ISSN 2288-5811 Copyright © 2017 The Korean Association for Health Technology Assessment Original Article
JoHTA
Current Status of the National Liver Cancer Surveillance Program in Korea
Sangjin Shin1, Ha jin Tchoe1, Jayoun Lee1, Jae Kyung Suh1, and Jin Won Kwon1,2
1Division of Healthcare Technology Assessment Research, National Evidence-based Healthcare Collaborating Agency (NECA), Seoul, Korea
2Department of Pharmacy, Kyungpook National University, Daegu, Korea
Received November 17, 2017 Revised November 25, 2017 Accepted November 30, 2017 Address for Correspondence:
Jin Won Kwon
Department of Pharmacy, Kyungpook National University, 80 Daehak-ro, Buk-gu, Daegu 41566, Korea Tel: +82-53-950-8580 Fax: +82-53-950-8557 E-mail: [email protected]
Objectives: Surveillance for liver cancer has been shown to improve survival via earlier cancer de- tection. Although liver cancer surveillance is conducted at national level in Korea, little is known of the diagnostic performance and adherence to this surveillance, especially in a real surveillance set- ting. The purpose of this study was to evaluate the adherence and diagnostic accuracy of the liver cancer surveillance in real practice setting in Korea. Methods: We used the National Health Insur- ance Service claims data linked with the National Liver Cancer Surveillance Program (NLCSP) from 2013 to 2015. We analyzed the surveillance adherence and diagnostic accuracy. Sensitivity, speci- ficity, and positive predictability values were assessed based on patients diagnosed with liver cancer within 3, 6, or 12 months after undergoing surveillance during the study period. Results: The an- nual surveillance rate resulted that individuals undergoing the NLCSP was 41.2% in 2014. Female, the younger, and people with less comorbidity and more income received more surveillance. The sensitivity of the surveillance program was 37.0% and 40.4% for positive predictive value and it was varied depending on the criteria used to define the diagnosis of liver cancer. Conclusion: This study highlights the current status of the NLCSP and the needs for continues efforts to help improve the current surveillance practice in quantitative and qualitative to fulfil the goal of NLCSP.
Key Words Liver neoplasm · Surveillance · Diagnostic accuracy · Surveillance rate.
data managed by National Health Insurance Service (NHIS- 2017-1-315). NHIS data has comprehensive data sets for di- agnoses, treatments including prescriptions and procedures, surgical history, and prescription records of all health insured or Medicaid patients visiting hospitals or clinics. NLCSP data includes the alanine aminotransferase, hepatitis B surface antigen test, US, and AFP Test results for medically checked subjects under NLCSP. The Institutional Review Board of the National Evidence-based Healthcare Collaborating Agency approved this study protocol (NECA-IRB16-003). The in- formed consent was not required because the data was pro- vided in the de-identified or anonymous form.
Study population
First, individuals with liver related diseases and liver can- cer in 2014 were selected. Liver-related diseases (HBV, HCV or cirrhosis) using International Classification of Diseases- 10th revision (ICD-10) codes (B18, B18.0, B18.1, B18.2, B18.8, B18.9, B19, B19.0, B19.9, K70.1, K70.10, K70.11, K70.2, K70.3, K70.30, K70.31, K70.9, K73, K73.0, K73.1, K73.2, K73.8, K73.9, K74, K74.0, K74.1, K74.2, K74.3, K74.4, K74.5, K74.6, K75.4, K76, K76.1, K76.5, K76.6, Z22.5) were defined. Liver cancer was defined with specific cancer identi- fication code of V193 and of C22.x To complement the accu- racy of ICD-10 code, the target participants (C22.x) of this study were patients who also had claimed health insurance benefits with the special cancer claim code (V193). Among of them, to define the target population for national surveillance program in 2014, we excluded patients having liver-related diseases at the age of <40 years and liver cancer diagnosed be- fore surveillance date in 2014.
Definition of surveillance adherence and diagnostic accuracy
The surveillance adherence was defined as the proportion of patients had the surveillance among all liver-related dis- eases patients in 2014. For diagnostic accuracy, to define true positive, we use period of 3, 6, and 12 months. After receiv- ing positive or negative results from the surveillance (AFP, US and final diagnosis), within 3, 6, and 12 months, in the case of patients whether or not have the diagnosis of liver cancer (C22.x and V193) and treatment based on claims in health insurance was defined as the true positive, true nega- tive, false positive. Based on this definition, we calculated sensitivity, specificity, and positive predicative value. The sen- sitivity, specificity, and positive predictive value (PPV) were calculated for each algorithm using a 2×2 table [liver cancer diagnosis results (yes/no) based on the surveillance versus true patients (yes/no; within 3, 6, and 12 months after the sur- veillance date) defined by C22.x and V193 based on NHI
claims database]. We determined the sensitivity, specificity and predictive value of each diagnostic tool.
Covariates
Baseline characteristics such as age and sex, income status based on insurance type, and concomitant diseases were con- sidered as covariates. In order to consider the health status, 1 year prior to index date, the diagnosis of concomitant dis- eases and cirrhosis (ICD-10, K74, K74.0–K74.6, K76.1, K70.2, K70.3, K70.30, and K70.31) was taken into consider- ation. We used the Charlson Comorbidity Index (CCI) to de- fine the severity of the concomitant diseases, which summa- rizes information on myocardial infarction, coronary heart disease, peripheral vascular disease, cardiovascular disease, chronic pulmonary disease, rheumatic heart disease, and re- nal insufficiency or renal failure.
Statistical analysis
We compared the baseline characteristics between groups using t-test for continuous variables and chi-squared test for categorical variables. A multivariate logistic regression model was used to identify predictors for adherence to surveillance.
The predictors considered in the model are sex, age, CCI, in- come status, cirrhosis and disability. All analyses were per- formed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and the proposed p-value was 2-sided with a significance lev- el of 5%.
Results
Patient characteristics by the surveillance rates The patient flow diagram is shown in Fig. 1. The number of target population was 657,415. From these, we investigated pa- tients having surveillance in 2014. Among the target popula- tion, 30% (197,511 patients) participated in the NLCSP. The intensity of the surveillance tests (receipt of ≥2 tests as com- pared with one or none) was very low (51 patients, 0.01%).
Individuals with liver related disease in 2014 (n=785,142)
Individuals aged <40 when liver related disease diagnosed (n=119,597)
Individuals identified with liver cancer diagnosis code before surveillance (n=8,130)
Target population for national surveillance program in 2014 (n=657,415)
Fig. 1. Flow diagram of the patient selection.
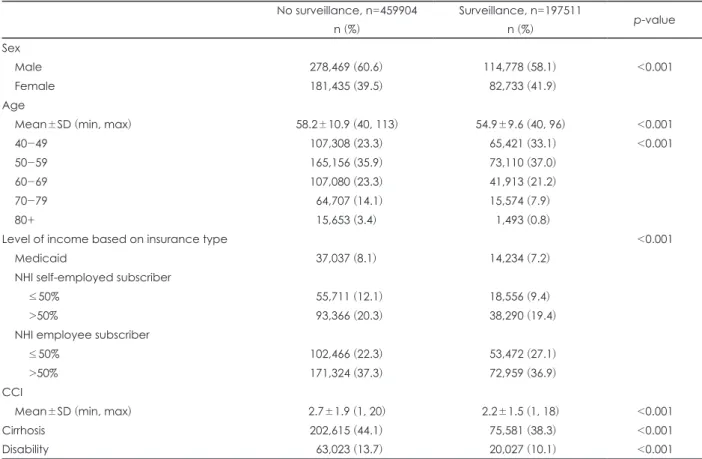
Characteristics of patients stratified by surveillance are shown in Table 1. In the surveillance group, there were more female (41.9% vs. 39.5%, p<0.001), less comorbidity (CCI 2.2±1.5 vs.
2.7±1.9, p<0.001), less cirrhosis (38.3% vs. 44.1%, p<0.001), and less disability (10.1% vs. 13.7%, p<0.001). And the average age was slightly younger (54.9±9.6 vs. 58.2±10.9, p<0.001).
According to income distribution, NHI employee subscriber with >50% income has the highest surveillance rate (36.9%).
Predictors for complete surveillance
Table 2 presents predictors for adherence to surveillance using multivariate analysis with baseline characteristics in- cluding those described in Table 1. On multivariate regression, all characteristics were significant for surveillance adherence.
Among of these, strong independent predictors were age. The percentage of surveillance was 0.456 (95% CI: 0.447–0.466) times lower among patients in 70’s than under 50 years old.
Diagnostic accuracy of HCC surveillance
In real setting of NLCSP, the sensitivity, specificity and PPV was not high. In 2014, sensitivity of final diagnosis was 46.3%
(37.0% for 6 months; 25.7% for 12 months), 99.8% for speci- ficity, and 38.6% (40.4% for 6 months; 43.6% for 12 months)
for PPV (Table 3).
The diagnostic accuracy of each modality also was checked.
For US, sensitivity was 43.8% (34.7% for 6 months; 23.8% for 12 months), 99.8% (same for 6 and 12 months) for specificity and 44.3% (46.0% for 6 months; 48.9% for 12 months). For AFP, sensitivity was even higher than US (55.3% for 3 months;
51.9% for 6 months; 44.8% for 12 months), and specificity was lower (95.4%). AFP has much lower PPV than US (3.8% for 3 months; 4.7% for 6 months; 6.4% for 12 months).
Discussion
In this study using NLCSP database and NHI claims data- base in Korea, we found that the adherence to surveillance of HBV, HCV or cirrhosis patients is poor (30% of all liver-relat- ed disease patients) and diagnostic accuracy is also not good as much as known in previous studies.8) The study also found that characteristics of patients are significantly related to sur- veillance adherence.
Most of studies9-11) which have assessed predictors for car- rying out surveillance and the proportion of cases for which NLCSP was carried out among liver related diseases patients using medical receipt databases have reported that surveil- Table 1. Characteristics of Korean patients with cirrhosis, chronic hepatitis B, and chronic hepatitis C, stratified by surveillance
No surveillance, n=459904 n (%)
Surveillance, n=197511
n (%) p-value
Sex
Male 278,469 (60.6) 114,778 (58.1) <0.001
Female 181,435 (39.5) 82,733 (41.9)
Age
Mean±SD (min, max) 58.2±10.9 (40, 113) 54.9±9.6 (40, 96) <0.001
40-49 107,308 (23.3) 65,421 (33.1) <0.001
50-59 165,156 (35.9) 73,110 (37.0)
60-69 107,080 (23.3) 41,913 (21.2)
70-79 64,707 (14.1) 15,574 (7.9)
80+ 15,653 (3.4) 1,493 (0.8)
Level of income based on insurance type <0.001
Medicaid 37,037 (8.1) 14,234 (7.2)
NHI self-employed subscriber
≤50% 55,711 (12.1) 18,556 (9.4)
>50% 93,366 (20.3) 38,290 (19.4)
NHI employee subscriber
≤50% 102,466 (22.3) 53,472 (27.1)
>50% 171,324 (37.3) 72,959 (36.9)
CCI
Mean±SD (min, max) 2.7±1.9 (1, 20) 2.2±1.5 (1, 18) <0.001
Cirrhosis 202,615 (44.1) 75,581 (38.3) <0.001
Disability 63,023 (13.7) 20,027 (10.1) <0.001
NHI: National Health Insurance, CCI: Charlson Comorbidity Index
lance was performed in 30–80% of patients, but it is the sta- tus in clinical setting not national surveillance program. One study conducted in Japan12) reported that the hepatocellular carcinoma (HCC) surveillance rate was 42.3% among pa- tients with chronic viral hepatitis and 56.6% with cirrhosis.
Although the rate was higher than this study, they concluded that surveillance rate for HCC was not adequately carried out among patients at risks for HCC in Japan, despite of rec- ommendation in guideline. The surveillance rate in 2014 from this study was 30% among the surveillance target pop- ulation and 38.8% in cirrhosis, these rate are lower than the rate from in Japan.
In addition, sensitivity and specificity in this study is very lower compared to the existing evidence.8,13) Previous studies have addressed the accuracy of US with a meta-analysis of 6
studies showing the pooled sensitivity and specificity for de- tection of HCC was 95% and 91% respectively. While US has become the established standard, there are wide variation in the quality of sonography that is performed.9) US is highly operative dependent and requires patient cooperation for op- timal surveillance. Performance of US-based surveillance is frequently deemed “operator-dependent” with various impli- cations regarding the experience of the technician or site of study, i.e., large territory/academic center with liver expertise versus a community or private imaging unit.14,15) US in nation- al surveillance program were performed by multiple medical centers likely with variable experience and expertise. There- fore diagnostic value would be different between in surveil- lance and clinical practice setting. AFP measurement is also commonly used for the surveillance of liver cancer because it Table 2. Predictive factors for carrying out surveillance
OR 95% CI p-value
Sex
Male 0.878 (0.686-0.888) <0.001
Female Ref
Age
40-49 Ref
50-59 0.722 (0.712-0.732) <0.001
60-69 0.686 (0.675-0.697) <0.001
70-79 0.456 (0.447-0.466) <0.001
80+ 0.186 (0.176-0.197) <0.001
Level of income based on type of insurance
Medicaid 0.879 (0.875-0.882) <0.001
NHI self-employed subscriber
≤50% 0.786 (0.777-0.795) <0.001
>50% Ref
NHI employee subscriber
≤50% 1.289 (1.268-1.310) <0.001
>50% 1.084 (1.077-1.111) <0.001
CCI 0.879 (0.875-0.882) <0.001
Cirrhosis
No Ref
Yes 0.786 (0.777-0.795) <0.001
Disability
No Ref
Yes 0.875 (0.859-0.891) <0.001
NHI: National Health Insurance, CCI: Charlson Comorbidity Index, OR: odds ratio, CI: confidence interval Table 3. Diagnostic value of national surveillance of liver cancer in 2014
3 months 6 months 12 months
Sen Spe PPV Sen Spe PPV Sen Spe PPV
US 43.8 99.8 44.3 34.7 99.8 46.0 23.8 99.8 48.9
AFP 55.3 95.4 3.8 51.9 95.4 4.7 44.8 95.5 6.4
Final diagnosis 46.3 99.8 38.6 37.0 99.8 40.4 25.7 99.8 43.6
US: ultrasonography, AFP: alpha-fetoprotein, Sen: sensitivity, Spe: specificity, PPV: positive predictive value
is relatively inexpensive, simple to perform, and is widely available. However, AFP is not a precise marker since it pro- vides low the sensitivity (20–60%) and specificity (50–94%),16) therefore AFP alone is not recommended as the surveillance test. US and AFP are most widely recommended as the pri- mary surveillance modalities for liver cancer. Compared with any single test, the combination of AFP and US increases both the sensitivity and specificity of liver cancer detection.8) However in Korea there is no consensus and uniform diag- nostic criteria for final diagnosis based on the results of both AFP and US.
In Korea, the target population for NLCSP included all indi- viduals 40 years and older, within which there was a high-risk group of patients with liver cirrhosis, carriers of HBV or HCV, or HBV-or HCV-induced chronic hepatitis.7) Despite this sur- veillance program since 2003, in Korea, 16178 new cases of liv- er cancer are reported per year and liver cancer is responsible for roughly 11311 deaths per year.17) Death from liver cancer is still dismally high. While there are still controversies for the implementation of NLCSP, there are several studies have reported on the effectiveness of liver cancer screening for high-risk group.18-23) Poor rate of surveillance or inappropri- ate diagnostic value could be one of the major responsible causes. This result can be generalizable because this study is investigated in real life practice setting. Our findings highlight the need for additional efforts to help improve the current sur- veillance practice in quantitative and qualitative to fulfil the goal of NLCSP.
The low surveillance rate of NLCSP likely reflects a combi- nation of misconception (faith of poor quality of national screening) as well as logistical factors, such as the need for repeated testing over relatively short periods of time and du- plicated tests in clinical setting. All hospitals and clinics pro- vide self-paid screening for liver cancer. These factors are likely obstacles facing the implementation of any effective NLCSP.
Because the target population for NLCSP is a high-risk popu- lation rather than a general population, it is imperative to in- crease participation in screening programmes.7)
Our study has some limitations. First, in the study the inci- dence of liver cancer was confirmed by ICD-10 code. Howev- er, information on diagnosis and disease included in the NHI database may not be optimal for identifying disease occur- rence, since the data have not been established for research purposes but for medical service claims and reimbursement.
To overcome this limitation liver cancer was defined by ICD- 10 code with the special claim code (V193). Second, the study is retrospective in design and NLSCP adherence can be un- derestimated or overestimated because all target population of NLSCP surveillance were not included in this study. The excluded group has clinically less possibility for causing liver
cancer, so in this study, we did not include them all. The sur- veillance adherence for liver cancer can be underestimated if surveillance imaging test were performed in clinical setting not national surveillance setting. In the future, methodologi- cal research might be needed to increase surveillance rates for NLSCP in patients with chronic hepatitis or those who received treatment at a clinic.
Conclusion
The surveillance rate of NLSCP in 2014 is suboptimal in the national setting and since 2004, it keeps increasing. Future studies should investigate reasons for poor adherence or per- sistency to inform effective clinical and governmental poli- cies that may improve the surveillance adherence of NLSCP.
Furthermore further studies need to be done for clarification to how overall diagnostic decision can be making based on US and AFP.
Acknowledgments
We thank all the professionals from National Health Insurance Ser- vice (NHIS) and all relevant data were obtained from the National Health Insurance Sharing Service (NHIS-2017-1-315).
REFERENCES
1) seer.cancer.gov [Homepage on the Internet] Bethesda, MD: National Cancer Institute; SEER Cancer Statistics Review (CSR) 1975-2014 [updated 2017 Jun 28; cited 2017 Aug 23]. Available from: https://
seer.cancer.gov/csr/1975_2014.
2) Tunissiolli NM, Castanhole-Nunes MMU, Biselli-Chicote PM, Pa- varino EC, da Silva RF, da Silva RC, et al. Hepatocellular Carcino- ma: a Comprehensive Review of Biomarkers, Clinical Aspects, and Therapy. Asian Pac J Cancer Prev 2017;18:863-872.
3) European Association for the Study of the Liver, European Organisa- tion for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2012;56:908-943.
4) Bruix J, Sherman M; American Association for the Study of Liver Dis- eases. Management of hepatocellular carcinoma: an update. Hepatol- ogy 2011;53:1020-1022.
5) Omata M, Lesmana LA, Tateishi R, Chen PJ, Lin SM, Yoshida H, et al.
Asian Pacific Association for the Study of the Liver consensus recom- mendations on hepatocellular carcinoma. Hepatol Int 2010;4:439-474.
6) Kim DY, Kim HJ, Jeong SE, Kim SG, Kim HJ, Sinn DH, et al. The Korean guideline for hepatocellular carcinoma surveillance. J Korean Med Assoc 2015;58:385-397.
7) Lee EH, Han MA, Lee HY, Jun JK, Choi KS, Park EC. Liver cancer screening in Korea: a report on the 2008 National Cancer Screening Programme. Asian Pac J Cancer Prev 2010;11:1305-1310.
8) Singal A, Volk ML, Waljee A, Salgia R, Higgins P, Rogers MA, et al.
Meta-analysis: surveillance with ultrasound for early-stage hepatocel- lular carcinoma in patients with cirrhosis. Aliment Pharmacol Ther 2009;30:37-47.
9) Davila JA, Morgan RO, Richardson PA, Du XL, McGlynn KA, El- Serag HB. Use of surveillance for hepatocellular carcinoma among patients with cirrhosis in the United States. Hepatology 2010;52:132- 141.
10) Jou JH, Chen PH, Jazwinski A, Bouneva I, Smith AD, Muir AJ. Rates
of surveillance and management of hepatocellular carcinoma in pa- tients evaluated at a liver transplant center. Dig Dis Sci 2010;55:3591- 3596.
11) Palmer LB, Kappelman MD, Sandler RS, Hayashi PH. Surveillance for hepatocellular carcinoma in a Medicaid cirrhotic population. J Clin Gastroenterol 2013;47:713-718.
12) Hirata A, Hirata T, Takahashi Y, Nakayama T. Surveillance rates for hepatocellular carcinoma among patients with cirrhosis, chronic hep- atitis B, and chronic hepatitis C based on Japanese claims database.
Hepatol Res 2017;47:283-292.
13) Kansagara D, Papak J, Pasha AS, O’Neil M, Freeman M, Relevo R, et al. Screening for hepatocellular carcinoma in chronic liver disease:
a systematic review. Ann Intern Med 2014;161:261-269.
14) Finberg HJ. Whither (wither?) the ultrasound specialist? J Ultrasound Med 2004;23:1543-1547.
15) Singal AG, Yopp AC, Gupta S, Skinner CS, Halm EA, Okolo E, et al.
Failure rates in the hepatocellular carcinoma surveillance process.
Cancer Prev Res (Phila) 2012;5:1124-1130.
16) Morimoto M, Numata K, Nozaki A, Kondo M, Moriya S, Taguri M, et al. Novel Lens culinaris agglutinin-reactive fraction of α-fetoprotein:
a biomarker of hepatocellular carcinoma recurrence in patients with low α-fetoprotein concentrations. Int J Clin Oncol 2012;17:373-379.
17) cancer.go.kr [Homepage on the Internet] National Center Informa- tion Center; survival rate [cited 2017 Aug 23]. Available from: http://
www.cancer.go.kr/mbs/cancer/subview.jsp?id=cancer_040304000000.
18) El-Serag HB, Kramer JR, Chen GJ, Duan Z, Richardson PA, Davila JA. Effectiveness of AFP and ultrasound tests on hepatocellular carci- noma mortality in HCV-infected patients in the USA. Gut 2011;60:992- 997.
19) Tanaka H, Nouso K, Kobashi H, Kobayashi Y, Nakamura S, Miyake Y, et al. Surveillance of hepatocellular carcinoma in patients with hepatitis C virus infection may improve patient survival. Liver Int 2006;26:543-551.
20) Tong MJ, Sun HE, Hsien C, Lu DS. Surveillance for hepatocellular carcinoma improves survival in Asian-American patients with hepa- titis B: results from a community-based clinic. Dig Dis Sci 2010;55:
826-835.
21) Wong GL, Wong VW, Tan GM, Ip KI, Lai WK, Li YW, et al. Surveil- lance programme for hepatocellular carcinoma improves the survival of patients with chronic viral hepatitis. Liver Int 2008;28:79-87.
22) Cucchetti A, Trevisani F, Pecorelli A, Erroi V, Farinati F, Ciccarese F, et al. Estimation of lead-time bias and its impact on the outcome of surveillance for the early diagnosis of hepatocellular carcinoma. J Hepatol 2014;61:333-341.
23) van Meer S, de Man RA, Coenraad MJ, Sprengers D, van Nieuwkerk KM, Klümpen HJ, et al. Surveillance for hepatocellular carcinoma is associated with increased survival: Results from a large cohort in the Netherlands. J Hepatol 2015;63:1156-1163.