36
Copyright 2020 The Korean Society of Neuro-Ophthalmology https://neuro-ophthalmology.co.krUnilateral Abducens Nerve Palsy in Multifocal Acquired Demyelinating Sensory and Motor Neuropathy
Sooyoung Kim, MD1, Nathan Jo, MD2, Kee Hong Park, MD3, Seong-Hae Jeong, MD, PhD2,4
1Department of Neurology, Seoul National University Bundang Hospital, Seongnam; 2Department of Neurology, Chungnam National University Hospital, Daejeon; 3Department of Neurology, Chungnam National University Sejong Hospital, Sejong; 4Department of Neurology, Chungnam National University School of Medicine, Daejeon, Korea
We report a 28-year-old woman with right abducens nerve palsy and monoparesis of right arm with an abnormal finding in a nerve conduction study that included a conduction block. After oral steroid treatment, her diplopia improved completely, but the monoparesis of right arm did not change. Numbness of the bilateral arm was newly observed in six months after discharge, and a follow-up nerve conduction study showed additional involvement of sensory nerves. In multifocal acquired demyelinating sen- sory and motor neuropathy, cranial nerve palsies are relatively common, but abducens nerve palsy has not been reported.
Keywords: Multifocal acquired demyelinating sensory and motor (MADSAM) neuropathy; Cranial nerve palsy; Abducens nerve palsy
The most important issue in a patient with abducens nerve palsy is whether the palsy is truly isolated. If other neurological signs are present, the patient should undergo an appropriate workup that evaluates the ob- served signs without delay. It has been reported that the incidence of cra- nial nerve involvement in Guillain-Barre syndrome (GBS) and chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) accounts for 45-75% and 3-15%, respectively.
1,2The facial nerve is the most com- monly involved cranial nerve in CIDP.
2Rare involvement of the oculo- motor, trigeminal, and hypoglossal nerves has also been reported.
2How- ever, abducens nerve palsy is very rarely reported in CIDP and has not been reported in multifocal acquired demyelinating sensory and motor (MADSAM) neuropathy, which is considered a variant of atypical form of CIDP. Herein, we present a patient with right abducens nerve palsy and monoparesis of right arm with an abnormal finding in the nerve conduction study (NCS) that included a conduction block (CB).
CASE REPORT
A 28-year-old woman visited the emergency room with first-ever bin-
ocular horizontal diplopia that occurred three days earlier. She did not note ocular pain and diurnal variation. She reported no preceding ill- nesses, recent infectious events, or trauma. However, she had a history that she could not walk independently due to the right sided weakness for a month and resolved completely without specific treatment five years ago. At that time, no detailed evaluations were conducted, and the diagnosis for those symptoms was unclear. Neurological examination revealed a 75% abduction limitation of her right eye (Fig. 1A). Even though she did not feel any motor weakness, mild monoparesis of right shoulder abduction (Medical Research Council grade 4) and decreased biceps jerk of right arm were observed. All the other examinations were normal. Brain magnetic resonance imaging (MRI)/MR angiography and repetitive nerve stimulation tests were normal. Cerebrospinal fluid (CSF) examination showed elevated protein (99 mg/dL, normal range of protein in CSF: 15-45 mg/dL) without pleocytosis. All serologic tests for binocular diplopia were normal, including anti-ganglioside antibodies.
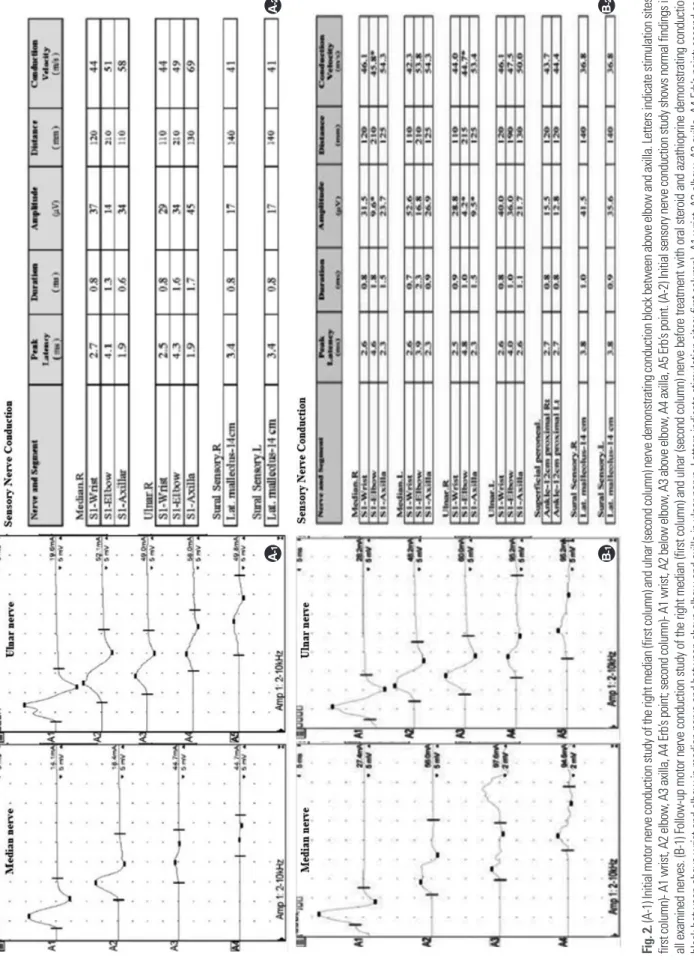
An NCS showed a definite CB at the axilla-elbow segment of the right median and ulnar nerves, and their conduction velocities were signifi- cantly decreased (Fig. 2A-1). Sensory conduction studies were normal
Correspondence to: Seong-Hae Jeong, MD, PhD
Department of Neurology, Chungnam National University Hospital, Chungnam National University School of Medicine, 282 Munhwa-ro, Jung-gu, Daejeon 35015, Korea Tel: +82-42-280-8057, Fax: +82-42-252-8654, E-mail: [email protected]
Received: Oct. 5, 2020 / Accepted: Oct. 15, 2020
CASE REPORT
ISSN: 2234-0971 대한안신경의학회지: 제10권 제2호
Clin Neuroophthalmol 10(2):36-39, December 2020
Unilateral Abducens Nerve Palsy in Multifocal Acquired Demyelinating Sensory and Motor Neuropathy•Kim S, et al.
Clin Neuroophthalmol 10(2):36-39, December 2020 https://neuro-ophthalmology.co.kr
37
(Fig. 2A-2). PMP22 gene mutation was not detected. Diplopia was im- proved with 1 mg/kg of oral prednisolone for seven days (Fig. 1B). How- ever, the monoparesis of the right arm did not change. Intravenous im- munoglobulin (IV Ig) administration was recommended, but the pa- tient refused at that time because she did not feel the symptom of right arm. However, numbness of the bilateral arm was newly observed in six months after discharge. A follow-up NCS showed additional involve- ment of sensory nerves. Chronic demyelinating neuropathy, such as CIDP or MADSAM neuropathy, can be considered as a diagnosis in a patient with recurrent sensorimotor symptoms and abnormal NCS findings suggestive of demyelination. Our patient initially suffered from unilateral abducens nerve palsy and monoparesis of right arm without sensory symptoms, and there was only an abnormality of motor nerves in the initial NCS. We thought multifocal motor neuropathy (MMN) was likely to be diagnosed. However, further observation and follow-up were required because cranial nerve (CN) palsies are rare in MMN. Dur-
ing the follow-up period, sensory symptoms and involvement of sensory NCS were newly observed (Fig. 2B-1, 2B-2). Therefore, it was finally diag- nosed with MADSAM neuropathy, which is considered a variant of CIDP. She started treatment with oral prednisolone and azathioprine.
After 1month, the monoparesis and numbness of right arm were fully recovered, and the numbness of left arm was partially improved.
DISCUSSION
The term MADSAM neuropathy is defined as slowly progressive asymmetric sensorimotor demyelinating neuropathy. MADSAM neu- ropathy is considered as atypical variant form of CIDP. CIDP is an im- mune-mediated sensorimotor polyneuropathy, characterized with sym- metric limb weakness, involving proximal as well as distal limbs. CIDP showed relapsing-remitting course and evidence of peripheral nerve de- myelination.
3MMN is characterized by slowly progressive asymmetric
A
B Fig. 1. (A) Initial nine gaze photographs show abduction limitation of the right eye (arrow). (B) Improved abduction of the right eye is noted in nine gaze photographs at seven days after oral prednisolone treatment.
Kim S, et al.•Unilateral Abducens Nerve Palsy in Multifocal Acquired Demyelinating Sensory and Motor Neuropathy
Clin Neuroophthalmol 10(2):36-39, December 2020
38
https://neuro-ophthalmology.co.krFig. 2. (A-1) Initial motor nerve conduction study of the right median (first column) and ulnar (second column) nerve demonstrating conduction block between above elbow and axilla. Letters indicate stimulation sites: first column)- A1 wrist, A2 elbow, A3 axilla, A4 Erb’s point; second column)- A1 wrist, A2 below elbow, A3 above elbow, A4 axilla, A5 Erb’s point. (A-2) Initial sensory nerve conduction study shows normal findings in all examined nerves. (B-1) Follow-up motor nerve conduction study of the right median (first column) and ulnar (second column) nerve before treatment with oral steroid and azathioprine demonstrating conduction block between above wrist and elbow in median nerve and between above elbow and axilla in ulnar nerve. Letters indicate stimulation sites: first column)- A1 wrist, A2 elbow, A3 axilla, A4 Erb’s point; second col- umn)- A1 wrist, A2 below elbow, A3 above elbow, A4 axilla, A5 Erb’s point. (B-2) Follow-up sensory nerve conduction study shows reduction in amplitude and conduction velocity of right median nerve above elbow.
A-1A-2 B-1B-2
Unilateral Abducens Nerve Palsy in Multifocal Acquired Demyelinating Sensory and Motor Neuropathy•Kim S, et al.
Clin Neuroophthalmol 10(2):36-39, December 2020 https://neuro-ophthalmology.co.kr
39
motor weakness without upper motor neuron signs, with minimal or no sensory symptoms. MADSAM neuropathy is distinguished from MMN by the presence of sensory involvement, and distinguished from CIDP by the multifocal, asymmetric pattern.
4,5CN palsies are observed more commonly in MADSAM neuropathy than in MMN.
6CN palsies can be involved in up to 15% of patients with MADSAM neuropathy and this is similar in CIDP.
7Although the pathophysiology of higher incidence of cranial nerve involvement in MADSAM neuropathy than in MMN is unclear, the cause is presumed to be related to anti-GM1 antibody. Anti- GM1 antibodies are often present up to 50% in MMN, but rarely in MADSAM neuropathy and CIDP. Unlike the anti-GQ1b antibodies, which target the cerebellum, oculomotor nerve, trochlear nerve, and ab- ducens nerve, anti-GM1 antibodies target the gray matter and surface of motor neuron in spinal cord.
8In a previous study on GBS, anti-GM1 an- tibody positivity was strongly correlated with findings such as the pres- ence of preceding gastrointestinal infections, absence of sensory symp- toms or signs, and lack of cranial nerve involvement.
9The cause may also be associated with high levels of CSF protein in MADSAM neuropathy.
CSF protein is usually elevated in MADSAM neuropathy and CIDP, but usually normal in MMN.
8Levels higher than normal indicate a patho- logic process in or near the ependyma or meninges.
10Although CN pal- sies are more common in MADSAM neuropathy than MMN, the in- volvement of the abducens nerve has not been reported in MADSAM neuropathy. The mainly involved CNs in MADSAM neuropathy are CNV, VII, IX, and X. There are only a few case reports of oculomotor nerve palsy in MADSAM neuropathy.
11The pathophysiology for low in- cidence of abducens nerve palsy in MADSAM neuropathy is unclear, but we presume that the pathophysiology of lateral rectus muscle weak- ness innervated by CN VI is probably due to the CB, such as of nerves in- nervating the limb muscles. If sensory symptoms are absent or mild, it is difficult to differentiate between MMN and MADSAM neuropathy at an early stage clinically. It is important to confirm the response to corti- costeroids in distinguishing MADSAM neuropathy from MMN. In MADSAM neuropathy, corticosteroid and IV Ig treatments are effec- tive, whereas IV Ig administrations, but not corticosteroids, are effective in MMN.
4Therefore, either IV Ig or prednisone may be used as the first line of therapy in MADSAM neuropathy unlike in MMN, which the first line of therapy of MMN is IV Ig. Our patient had diplopia treated with high-dose corticosteroids but that treatments were not responsible
for the monoparesis of right arm. Therefore, it was not easy for us to dis- tinguish the two disease by therapeutic responses to steroids. Eventually further observation of progression made the diagnosis possible.
In conclusion, it is easy to focus on the ophthalmologic evaluation of a patient with diplopia, but detailed medical history and neurological ex- amination are important for diagnosis. And abducens nerve palsy can also be observed in MADSAM neuropathy like other CN palsies. We re- port an interesting case of a patient diagnosed with MADSAM neuropa- thy presenting as unilateral abducens nerve palsy, which has not been re- ported.
REFERENCES
1. Nanda SK, Jayalakshmi S, Ruikar D, Surath M. Twelfth cranial nerve in- volvement in Guillian Barre syndrome. Journal of neurosciences in rural practice 2013;4:338.
2. Al-Bustani N, Weiss MD. Recurrent isolated sixth nerve palsy in relaps- ing-remitting chronic inflammatory demyelinating polyneuropathy.
Journal of Clinical Neuromuscular Disease 2015;17:18-21.
3. Shibuya K, Tsuneyama A, Misawa S, Suichi T, Suzuki YI, Kojima Y, et al.
Cranial nerve involvement in typical and atypical chronic inflammatory demyelinating polyneuropathies. J European journal of neurology 2020.
4. Van Schaik I, Bouche P, Illa I, Léger JM, Van Den Bergh P, Cornblath D, et al. European Federation of Neurological Societies/Peripheral Nerve Society guideline on management of multifocal motor neuropathy. Euro- pean journal of neurology 2006;13:802-808.
5. Katz JS, Saperstein DS. Asymmetric acquired demyelinating polyneu- ropathies: MMN and MADSAM. J Current Treatment Options in Neurol- ogy 2001;3:119-125.
6. Saperstein DS, Amato AA, Wolfe GI, Katz JS, Nations SP, Jackson CE, et al. Multifocal acquired demyelinating sensory and motor neuropathy:
the Lewis–Sumner syndrome. Muscle Nerve: Official Journal of the Amer- ican Association of Electrodiagnostic Medicine 1999;22:560-566.
7. Yoo SK, Kim MO, Kim CH, Kim Y-S, Kim S-K, Kang H, et al. Unilateral Hypoglossal neuropathy in multifocal acquired demyelinating sensory and motor neuropathy: differential diagnosis of motor neuron disease.
Journal of the Korean Neurological Association 2018;36:210-214.
8. Lee DK. Multifocal motor neuropathy. J Annals of Clinical Neurophysiol- ogy 2002;4:98-107.
9. Kim JK, Bae JS, Kim D-S, Kusunoki S, Kim JE, Kim JS, et al. Prevalence of anti-ganglioside antibodies and their clinical correlates with Guillain- Barré syndrome in Korea: a nationwide multicenter study. J Journal of Clinical Neurology 2014;10:94-100.
10. Ropper AH, Adams R, Victor M, Samuels MA. Adams and Victor’s prin- ciples of neurology, 10th edition: McGraw Hill Medical, 2005.
11. Oh S, Claussen G, Kim D. Motor and sensory demyelinating mononeu- ropathy multiplex (multifocal motor and sensory demyelinating neurop- athy): a separate entity or a variant of chronic inflammatory demyelinating polyneuropathy? Journal of the Peripheral Nervous System: Jpns 1997;2:
362-369.