Vol. 9, No. 3, September, 2002
COX-2 특이적 억제제와 인지기능에 대한 예비 연구
한양대학교 의과대학 내과학교실, 류마티스병원, 정신과학교실*
최연수․오승일․이장환*․김태환․전재범 정성수․유대현․배상철
= Abstract =
COX-2 Specific Inhibitor and Cognitive Function: a Pilot Study
Yeon-Soo Choi, M.D., Ph.D., Seung-Il Oh, M.D., Jang-Whan Lee, Ph.D.*, Tae-Hwan Kim, M.D., Ph.D., Jae-Bum Jun, M.D., Ph.D., Sungsoo Jung, M.D., Ph.D.,
Dae-Hyun Yoo, M.D., Ph.D., Sang-Cheol Bae, M.D., Ph.D., MPH
Department of Internal Medicine, The Hospital for Rheumatic Disease, Department of Psychiatrics*, Hanyang university, Seoul, Korea
Objective: New nonsteroidal anti-inflammatory drugs (NSAIDs) with highly selective cyclooxy- genase-2 (COX-2) inhibition afford protection against gastropathy, but their acute and long-term effects on the central nervous system are unclear. Our aim was to investigate the influence of COX-2 specific inhibitor (celecoxib) on cognitive function.
Methods: Within the context of a randomized controlled parallel trial of NSAIDs for osteoar- thitis (OA), we performed a battery of neuropsychological tests in consecutive 10 osteoarthritis patients with celecoxib (200 mg/day) and 13 osteoarthritis patients with diclofenac (100 mg/day) before and after 4 weeks by clinical psychologists who were not involoved in the study and unaware of study protocols and treatment allocation. The tests were performed randomly in sequence in order to minimize learning effect. The examed cognitive domains included memory, reasoning/problem solving, simple and complex attention, visual-spatial processing, and psyc- homotor speed.
Results: Demographic characteristcs (age, sex, disease duration, functional status measured by patient's and physician's global assessment and KWOMAC, CES depression score, education level) were not significantly different between both treatment groups. In all cognitive domains,
ꠏ ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
<접수일:2002년 1월 21일, 심사통과일:2002년 3월 15일>
※통신저자:배 상 철
서울특별시 성동구 행당동 산 17 한양대학교 의과대학 류마티스병원
Tel:02) 2290-9203, FAX:02) 2298-8231, E-mail:[email protected]
*본 연구는 2000년 한양대학교 일반연구비 지원으로 연구되었음.
서 론
비스테로이드성 항염제(Nonsteroidal anti-inflammatory drugs, NSAIDs)는 류마티스 질환뿐 아니라 신경질환, 종양, 알츠하이머병과 같은 질환에도 널리 사용되며1) 미국의 경우만 3천만 명 이상이 사용하고2) 전 세계 적으로는 60억 달러 이상의 매출을 올리는 가장 많 이 사용되는 약제 중 하나이다3). 1998년 국민건강․
영양조사에 의하면 우리나라 국민 중 45세 이상 성 인에서 관절염은 가장 흔한 만성질환으로 NSAIDs 는 우리나라에서도 가장 많이 소모되는 약제 중 하 나이다4).
NSAIDs의 주요 작용기전은 cyclooxygenase (COX) 을 억제하여 arachidonic acid로부터 prostaglandin (PG) 의 합성을 차단함으로써 항염증 효과를 나타낸다1). COX는 1991년 내재적(constitutively) 형태의 COX-1 과 염증성 자극에 의해 유도되는 COX-2의 두 가지 동종효소(isoform)가 있음이 밝혀진 바 있다1,5). COX-1 은 위점막, 중추 신경계, 신장, 단핵구-거대세포, 혈 소판, 기타조직 등에 발현되어 주로 생리적 기능 (housekeeping role)을 담당하며6) COX-2는 염증성 자 극에 의해 그 작용이 증가하므로1) NSAIDs와 관련된 부작용은 주로 COX-1의 억제로 인해 발생되며 항염 효과는 COX-2의 억제에 기인한다7,8). 그러나 COX-2 가 염증과 무관하게 중추신경계(대뇌 피질, 해마, 편 도체), 난소, 신장, 기타조직 등에서도 내재적으로 발현됨이 밝혀져 COX-2 역시 COX-1와 같이 생리적 기능을 일부 담당하리라 추측하고 있다 9-11).
COX-1과 COX-2를 동시에 억제하는 기존의 NSAIDs 는 특히 위장관 부작용이 문제시되며1) 현재 증가 추 세에 있는 노인인구에서 인지기능과의 관련성에 대
해 여러가지 논란이 많은 상태이다. 또한 COX-2 특 이적 억제제(COX-2 specific inhibitor)는 위장관 부작 용면에서 많이 개선되었으나12,13) 노인들에게 사용할 경우 그들의 인지기능에 어떤 영향을 초래할 것인지 에 대해서는 아직 연구된 바 없다.
저자들은 기존의 NSAIDs와 달리 위장관 부작용을 줄이면서 항염증 및 진통작용을 발휘하는 COX-2 특 이적 억제제가14,15) 인지기능에 미치는 영향을 보고 자 예비 연구(pilot study)를 하였으며 더불어 기존의 NSAIDs와 COX-2 특이적 억제제가 인지기능에 미치 는 영향을 비교하여 보았다.
대상 및 방법
한양대학교 류마티스병원에서 골관절염으로 치료 받고 있는 환자들 중 본 연구에 동의한 53명의 환자 에서 무작위로 선택한 26명에게 celecoxib (200 mg/
일)를, 27명에게 diclofenac (100 mg/일)을 4주간 투여 하였다. 각 대상집단은 약물투여 전과 약물투여 4주 후의 인지기능을 평가받았다. Celecoxib을 투여한 군 에서는 26명 중 10명이 약물투여 후의 인지기능을 평가 받았고 diclofenac을 투여한 군에서는 27명 중 13명이 인지기능을 평가받았다. 또한 인지기능에 영 향을 줄 수 있는 대상집단의 나이, 질병기간, 교육정 도와 골관절염 정도을 평가하기 위한 도구로서 Korean Western Ontario and McMaster Univerities Osteoar- thritis Index (KWOMAC)16) 및 우울증의 동반여부를 평가하기 위한 도구로 The Korean version of the Center for Epidemiologic Studies Depression Scale (CES-D, Korean version)17)을 조사하였다.
we did not find out significant cognitive decline before and after treatments either with celecoxib or diclofenac. There was no difference in the change of cognitive function between both treat- ment groups.
Conclusion: The short-term use of COX-2 specific inhibitor as well as conventional NSAID may not impair cognitive function. The long-term follow up study using large number of patients is in progress.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: COX-2 specific inhibitor, Cognition, Nonsteroidal anti-inflammatory drug, Osteoar-
thritis
1. 인지기능 평가
인지기능 검사는 본 연구의 연구계획 및 약물사용 여부에 대해 모르는 임상 심리사 2명이 시행하였고 같은 환자는 같은 임상 심리사가 평가하였다.
인지기능은 기억력(Memory), 문제 해결능력(Reason- ing/Problem solving), 주의력(Attention), 시공감각 처 리능력(Visual-Spatial processing), 정신운동 속도(Psy- chomotor speed) 다섯 개의 영역으로 분류하여 펑가 하였다. 인지기능 영역을 평가하는 도구로는 한국판 Rey-Kim 기억 검사를 이용하여 언어성 기억과 시각 기억의 일치도를 측정한 후 전체 기억지수를 산출하 였고18) 한국판 웩슬러 지능검사(Korean Wechsler Intel- ligence Scale, KWIS)19)를 이용하여 문제 해결능력 (Reasoning/Problem solving)을 측정하는 이해문제, 주 의력(Attention)을 측정하는 숫자문제, 시공감각 처리 능력(Visual-Spatial processing)을 측정하는 토막짜기, 정신운동 속도(Psychomotor speed)를 측정하는 바꿔 쓰기를 선택하여 실시하였다.
2. 우울증 평가
우울증은 인지기능에 영향력을 줄 수 있는 중요한 변수로서 대상 환자들의 우울증 여부를 측정하였다.
우울증의 측정도구로는 문항들이 매우 간결하여 지 역사회 군에서의 역학용 연구에 특히 적절하다고 알 려진 CES-D 한국어 판17)을 사용하여 대상환자들의 우울증을 평가하였다.
3. KWOMAC
대상환자들의 골관절염 정도를 평가하기 위해 배 등16)이 발표한 한국판 WOMAC를 사용하여 통증 점 수범위: 0∼20, 강직정도 점수범위: 0∼8, 신체적 기능 점수범위: 0∼68, 총 점수범위: 0∼96으로 평가하였다.
4. 통계분석
통계분석은 SAS (Statistical Analysis System) ver- sion 8.1을 이용하였고 유의수준은 p값이 0.05 미만 인 경우를 통계학적 유의성이 있는 것으로 보았다.
나이, 교육정도, 유병기간, 질병정도, 우울증 동반여 부 등 인지기능에 영향을 줄 수 있는 인자와 약물사 용 전후의 인지기능과의 관계는 paired t-test를 시행
하였고, 두 약물(celecoxib, diclofenac) 간의 인지기능 변화에 대한 비교는 t-test을 시행하였다.
결 과 1. Celecoxib군에서의 인지기능 평가
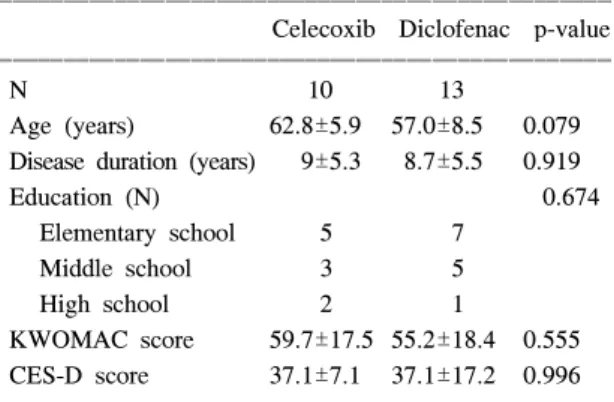
Celecoxib (COX-2 specific inhibitor)를 투여한 10명 의 대상환자들은 52∼69세로 평균연령은 62.8±5.9 세, 질병의 유병기간은 9±5.3년, 학력은 초등학교 5 명, 중학교 3명, 고등학교 2명이었고 골관절염 정도 (KWOMAC) 점수는 59.7±17.5, 우울증 점수(CES-D score)는 37.1±7.1이었다(표 1).
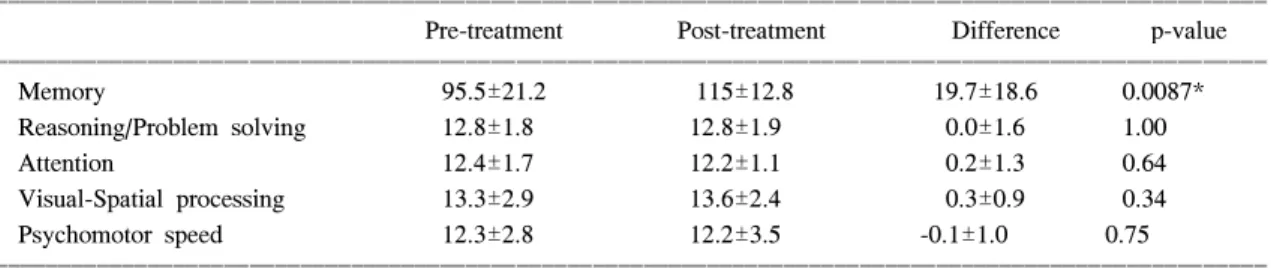
Celecoxib를 4주 동안 투여 후 환자들로부터 약물 을 사용하기 전과 후의 기억(Memory)지수 차이와 이해력 및 문제해결 능력(Reasoning-Problem solving), 주의력(Attention), 시공감각 처리능력(Visual-Spatial pro- cessing), 정신운동 속도(Psychomotor Speed)의 연령별 기준 환산점수 차이를 조사한 결과 기억력(Memory) 의 향상을 보였으나(p<0.01) 나머지 인지기능 영역 에서는 약물 투여 전과 후의 각 인지기능 영역에서 통계학적 유의성을 관찰할 수 없었다(표 2).
또한 인지기능에 영향을 줄 수 있는 인자들(나이, 유병 기간, 교육 정도, 질병 정도, 우울증 동반 여부) 와 각 인지기능 영역과의 관계를 paired t-test를 이용
Table 1. Baseline characteristics in osteoarthritis with celecoxib and diclofenac
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Celecoxib Diclofenac p-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
N 10 13
Age (years) 62.8±5.9 57.0±8.5 0.079 Disease duration (years) 9±5.3 8.7±5.5 0.919
Education (N) 0.674
Elementary school 5 7 Middle school 3 5
High school 2 1
KWOMAC score 59.7±17.5 55.2±18.4 0.555 CES-D score 37.1±7.1 37.1±17.2 0.996 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Data presented are mean±SD, N; number, p<0.05.
KWOMAC: Korean Western Ontario and McMaster Uni- verities Osteoarthritis Index, CES-D: The Korean version of the Center for Epidemiologic Studies-Depression scale
하여 통계적 유의성을 평가하였다(표 3). Celecoxib를 투여한 65세 이상, 교육수준 6년 이상, 우울증 점수 (CES-D score) 37점 이하, 골관절염 정도(KWOMAC) 점수 55.5 미만인 경우에서 약물투여 전보다 투여 후의 기억지수가 향상되었음을 보여주었다. 반면 65세 미만, 교육수준 6년 미만, 골관절염 정도 (KWOMAC) 점수 55.5 이상, 우울증 점수(CES-D score)
38점 이상인 환자 군에서는 약물투여 전과 투여 후 의 각 인지기능과의 상관관계에서 통계적 유의성이 없었고 골관절염의 유병기간도 인지기능과의 상관관 계에서 통계적 유의성이 없었다.
2. Diclofenac군에서의 인지기능 평가
Diclofenac을 투여한 13명의 대상환자들은 52∼66 Table 2. Cognitive function change between post-treatment and pre-treatment of celecoxib
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Pre-treatment Post-treatment Difference p-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Memory 95.5±21.2 115±12.8 19.7±18.6 0.0087*
Reasoning/Problem solving 12.8±1.8 12.8±1.9 0.0±1.6 1.00
Attention 12.4±1.7 12.2±1.1 0.2±1.3 0.64
Visual-Spatial processing 13.3±2.9 13.6±2.4 0.3±0.9 0.34
Psychomotor speed 12.3±2.8 12.2±3.5 -0.1±1.0 0.75
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
* p<0.05
Table 3. Mean and standard deviation for 5 dimensions of the cognitive function according to age, disease duration, education, disease severity and depression in osteoarthritis patients on celecoxib
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Reasoning/
Visual-Spatial Psychomotor Factors n Memory** problem Attention† processing‡ speed††
solving***
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Age 65 yrs> 5 17.8±22.20 0.0±2.12 0.0±1.58 0.8±0.84 0.0±0.71
65 yrs≤ 5 21.6±16.83* 0.0±1.22 -0.4±1.14 -0.2±0.84 -0.2±1.30 Disease duration 8.3 yrs> 5 17.0±20.53 -0.6±2.07 -0.4±1.51 0.0±0.70 -0.4±0.54 8.3 yrs≤ 5 22.4±18.58 0.6±0.89 0.0±1.22 0.6±1.14 0.2±1.30 Education 6 yrs> 5 16.6±22.61 0.8±1.30 0.2±1.48 0.6±0.89 -0.2±0.84
6 yrs≤ 5 22.8±15.80* -0.8±1.64 -0.6±1.14 0.0±1.00 0.0±1.23 KWOMAC score‡‡Low 5 22.8±15.80* -0.8±1.64 -0.6±1.14 0.0±1.00 0.0±1.23 High 5 16.6±22.61 0.8±1.30 0.2±1.48 0.6±0.89 -0.2±0.83 CES-D score§ 37≥ 5 16.0±1.22* -0.6±1.95 0.0±1.00 0.4±1.34 0.2±1.10
37< 5 23.4±27.37 0.6±1.14 -0.4±1.67 0.2±0.45 -0.4±0.89 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ n; number, *p<0.05
** memory difference between post-treatment & pre-treatment
*** age adjusted reasoning/problem solving difference between post-treatment & pre-treatment
† age adjusted attention difference between post-treatment & pre-treatment
‡ age adjusted visual-spatial processing difference between post-treatment & pre-treatment
†† age adjusted psychmotor speed difference between post-treatment & pre-treatment
‡‡ celecoxib median value 55.5≤(High), 55.5>(Low)
§ depression score median value
세로 평균연령 57.0±8.5세, 질병의 유병기간은 8.7±
5.5년, 교육수준은 초등학교 7명, 중학교 5명, 고등학 교 1명이었고 골관절염 정도(KWOMAC) 점수는 55.2
±18.4, 우울증 점수(CES-D score)는 37.1±17.2이었 다(표 1).
Diclofenac을 4주 동안 투여 후 환자들로부터 약물 을 사용하기 전과 후의 기억(Memory) 지수 차이와 이해력 및 문제해결 능력(Reasoning-Problem solving),
주의력(Attention), 시공감각 처리능력(Visual-Spatial pro- cessing), 정신운동 속도(Psychomotor Speed)의 연령별 기준 환산점수 차이를 조사한 결과 약물투여 전과 투 여 후의 각 인지기능 영역에서 통계학적 유의성을 관 찰할 수 없었다(표 4).
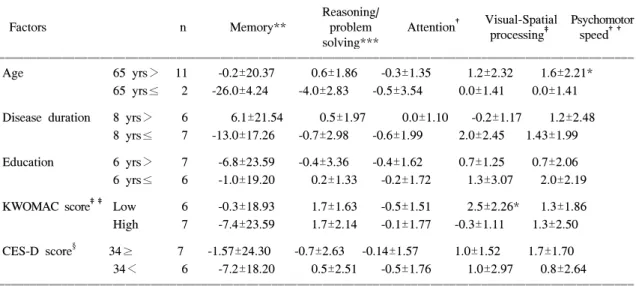
또한 인지기능에 영향을 줄 수 있는 인자들(나이, 유병기간, 교육정도, 질병정도, 우울증 동반여부)과 각 인지기능 영역과의 관계를 paired t-test를 이용하
Table 5. Mean and standard deviation for 5 dimensions of the cognitive function according to age, disease duration, education, disease severity and depression in osteoarthritis patients on diclofenac
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Reasoning/ Visual-Spatial Psychomotor
Factors n Memory** problem Attention† processing‡ speed††
solving***
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Age 65 yrs> 11 -0.2±20.37 0.6±1.86 -0.3±1.35 1.2±2.32 1.6±2.21*
65 yrs≤ 2 -26.0±4.24 -4.0±2.83 -0.5±3.54 0.0±1.41 0.0±1.41 Disease duration 8 yrs> 6 6.1±21.54 0.5±1.97 0.0±1.10 -0.2±1.17 1.2±2.48
8 yrs≤ 7 -13.0±17.26 -0.7±2.98 -0.6±1.99 2.0±2.45 1.43±1.99 Education 6 yrs> 7 -6.8±23.59 -0.4±3.36 -0.4±1.62 0.7±1.25 0.7±2.06 6 yrs≤ 6 -1.0±19.20 0.2±1.33 -0.2±1.72 1.3±3.07 2.0±2.19 KWOMAC score‡‡ Low 6 -0.3±18.93 1.7±1.63 -0.5±1.51 2.5±2.26* 1.3±1.86 High 7 -7.4±23.59 1.7±2.14 -0.1±1.77 -0.3±1.11 1.3±2.50 CES-D score§ 34≥ 7 -1.57±24.30 -0.7±2.63 -0.14±1.57 1.0±1.52 1.7±1.70
34< 6 -7.2±18.20 0.5±2.51 -0.5±1.76 1.0±2.97 0.8±2.64 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ n; number, *p<0.05
** memory difference between pre & post-treatment
*** age adjusted reasoning/problem solving difference between pre & post treatment
† age adjusted attention difference between pre & post treatment
‡ age adjusted visual-spatial processing difference between pre & post treatment
†† age adjusted psychmotor speed difference between pre & post treatment
‡‡ diclofenac median value 56≤(High), 56>(Low)
§ depression score median value
Table 4. Cognitive function change between post-treatment and pre-treatment of diclofenac
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Pre-treatment Post-treatment Difference p-value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Memory 103±12.9 12.7±23.2 -4.1±21.0 0.49
Reasoning/problem solving 12.8±2.3 12.7±2.2 -0.2±2.5 0.83
Attention 11.3±2.1 11.0±2.0 -0.3±1.6 0.50
Visual-Spatial processing 12.3±2.8 13.3±3.2 1.0±2.2 0.12
Psychomotor speed 13.5±3.8 13.5±3.8 1.3±2.1 0.05
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ p<0.05
여 평가한 결과 diclofenac을 투여한 65세 미만인 경 우에서 정신운동 속도(Psychomotor Speed)는 약물투 여 전보다 투여 후에 향상되었고 골관절염 정도 (KWOMAC) 점수 56점 미만인 경우에서 시공감각 처리능력(Visual-Spatial processing)은 약물투여 후에 향상되었음을 관찰할 수 있었다.
반면 65세 이상, 골관절염 정도(KWOMAC) 점수 56점 이상인 경우와 골관절염의 유병기간, 교육정도, 우울증 동반여부는 약물사용과 상관없이 인지기능에 유의한 변화가 없는 것으로 조사되었다(표 5).
3. 두 약물(celecoxib, diclofenac)에서의 인지기능 변화비교
Celecoxib와 diclofenac 두 약물 간의 인지기능 변화 를 비교한 결과 celecoxib를 사용한 군에서 diclofenac 을 사용한 군보다 기억력(Memory)은 향상되는 것으 로 나타났으나(p<0.01) 나머지 인지기능 영역에서는 두 약물 간의 통계학적 유의성을 관찰할 수 없었다.
고 찰
노인에서 치매를 유발하는 흔한 원인 중 하나인 알츠하이머병(Altzheimer's disease)은 진행성 신경변 성 질환으로 65세 이후 유병률이 급속히 증가하는 것으로 알려져 있다. 알츠하이머병은 심한 인지기능 저하, 행동장애 및 일상생활을 수행할 수 있는 능력 이 감소하는 것을 특징으로 하며 인지기능의 중심부 가 되는 뇌의 해마(hippocampus)와 대뇌피질(cortex) 에서 COX-2의 발현이 증가되는 것으로 보고된 바 있다20).
Cyclooxygenase-2 (COX-2)는 다양한 생리학적, 병 태생리학적 기능을 가지고 있으며 일반적으로 염증 과 생리학적 자극에 의해서 유도되는 효소로 알려져 있다. COX-2는 체내에 광범위하게 분포되어 있으며 특히 뇌, 신장의 발달과정에서 내재적(constitutively) 으로 발현되며 뇌의 대뇌피질(cortex), 해마(hippocam- pus), 편도체(amygdala)에 존재하고9-11) 다양한 자극 즉 경련, 통증, 스트레스 등에 의해 발현이 증가하는 것으로 알려져 있다21). Lipsky 등은 COX-2가 기억형 성에 영향을 주는 시냅스 후 신호(postsynaptic signal- ing)에 관여한다고 보고하였다22). 그러나 COX-2가
뇌의 발달, 기억형성 및 인지기능에 관여하며 다양 한 자극에 발현정도가 증가된다는 것은 동물실험을 기초로 한 연구이며 사람을 대상으로 한 연구에서는 아직 입증되지 않은 상태이다20).
임상적으로 흥미로운 사실은 NSAID를 투여함으로 써 알츠하이머병의 진행을 지연시킬 수 있다는 것이 다. Rich 등은 1995년 210명의 알츠하이머 환자들을 대상으로 NSAID을 투여한 결과 투여하지 않은 환자 에 비하여 질환의 경과가 지연되었음을 보고하였고23) Roger 등도 경증-중등증의 알츠하이머 환자들 44명 에게 6개월 동안 NSAID 투여 후 투여하지 않은 환 자들에 비하여 인지기능이 감소되는 것을 예방할 수 있었다고 보고하였다24). 또한 Stewart 등은 알츠하이 머병의 상대위험도(relative risk)는 NSAID의 사용기 간에 비례하여 감소한다고 하였다25). 알츠하이머 병 의 원인이 완전히 규명되진 않았으나 최소한 세포손 상 중 한 가지 기전은 염증성 과정으로 NSAID를 사 용함으로써 인지기능 저하의 예방과 치료에 중요한 역할을 하는 것으로 인식되고 있다26-28).
알츠하이머병과는 달리 치매증상이 없는 노인들을 대상으로 한 Goodwin 등의 연구를 살펴보면 65세 이상 노인 8명에게 NSAID사용 후 인지기능 저하와 성격 변화를 가져왔고 약물중단 2주 후 인지기능 및 성격 변화가 회복되었음을 보고하였다29). Joseph 등 도 도시 거주 노인 2,765명을 대상으로 3년 추적 검 사 후 NSAID사용이 노인들의 인지기능에 실질적으 로 예방효과가 없을 뿐 아니라 고용량의 NSAID사용 이 오히려 기억력의 저하를 초래한다고 보고하였으 며30), 그 외에도 NSAID사용으로 노인들의 인지기능 이 저하됨을 보고한 문헌들이 다수 있다31-33). 그러나 Wysenbeek 와 Frankline 등은 NSAID와 인지기능과는 상관관계가 없음을 주장하고 있어서34,35) 대체적으로 NSAID가 알츠하이머병에서는 치매를 예방하고 질환 의 진행을 늦출 수 있다는 견해가 받아들여지고 있 으나 치매증상이 없는 노인들의 인지기능에 미치는 영향에 대해서는 논란이 많은 상태이다.
저자들은 최근 증가하는 노인 인구에서 NSAID와 인지기능과의 관계를 다시 재조명하는 것은 중요한 의미를 갖는다고 생각하여 COX-2 특이적 억제제와 기존의 NSAID가 인지기능에 미치는 영향을 조사, 비교하였다. COX-2 특이적 억제제(celecoxib)를 사용
한 환자군은 약물투여 전보다 투여 후에 기억력이 향상된 것으로 나타났으며, 기존의 NSAID (diclofenac) 와 비교 시 celecoxib를 사용한 환자군에서 기억력의 향상을 보였으나 다른 인지기능 영역(문제해결 능 력, 주의력, 시공감각 처리능력, 정신운동 속도)에서 는 의미있는 변화가 관찰되지 않았다.
본 연구는 대상집단의 수가 적고 추적기간이 짧아 통계적 유의성을 평가하는 데 제한점을 갖고 있으나 아직까지 보고된 바 없는 COX-2 특이적 억제제와 인지기능과의 상관관계를 조사한 예비연구로서 의의 가 있으며 앞으로 더 많은 집단을 대상으로 한 장기 간의 추적검사가 필요할 것으로 생각한다.
결 론
Celecoxib는 약물투여 후 기억력의 향상이 있는 것 으로 조사되었고 diclofenac은 인지기능에 영향을 줄 수 있는 변수들을 고려할 때 약물투여 후 시공감각 처리능력과 정신운동 속도에 향상이 있는 것으로 조 사되었다. 두 약물을 비교한 결과 celecoxib가 diclo- fenac에 비해 약물투여 후의 기억력이 향상된 것으 로 나타났으나 기억력 평가는 검사 전과 후의 학습 효과를 완전히 배제하기 어려우므로 저자들은 cele- coxib가 인지기능에 큰 영향을 주는 것으로 보기는 어려우며 또한 diclofenac에 비해서 더 우수하다고 판단하기는 힘들 것으로 간주한다.
REFERENCES
1) Santana-Sabagun E, Weisman MH. Nonsteroidal anti- inflammatory drugs. In: Shaun R, Edward Dh, Cle- mennnt BS, eds. Kelly's Textbook of Rheumatology.
6th ed. P. 799-822, Philadelphia, W.B. Saunders, 2001.
2) Gabriel SE, Febring RA. Trends in the utilization of nonsteroidal anti-inflammatory drugs in the United States. J Clin Epidemiol 1992;45:1041-4.
3) Paulus HE. FDA arthritis advisory committee meet- ings: Post-marketing surveillance of nonsteroidal anti- inflammatory drugs. Arthritis Rheum 1985;28:1168-9.
4) 배상철, 곽은주, 윤정이. 한국인 관절염의 역학적 특성 및 영양요인과의 연관성. 1998 국민건강․영양조사 심 층․연계분석 2000;217-32.
5) Dewitt DL, Meade EA, Smith WL. PGH synthase
isoenzyme selectivity: the potential for safer non- steroidal antiinflammatory drugs. Am J Med 95(suppl 2A) 1993;40S-4S.
6) Crofford LJ. COX-1 and COX-2 tissue expression:
Implications and predictions. J Rheumatol 1997;24:
15-9.
7) Vane HR. Towards a better aspirin. Nature 1994;367:
215-6.
8) Pairet M, Engelhardt G. Distinct isoform (COX-1 and COX-2) of cyclooxygenase: possible physiological and therapeutic implication. Fund Clin Pharmacol 1996;
10:1-15.
9) Breder CD, DeWitt DL, Kraig RP. Characterization of inducible cyclooxygenase in rat brain. J Comp Neurol 1995;355:296-315.
10) Guan Y, Chang M, Cho W. Cloning, expansion, and regulation of rabbit COX-2 in renal medullary inter- stitial cells. Am J Physiol 1997;273:F18-26.
11) Yasojima K, Schsab C, McGeer EG. Distribution of cyclooxygenase-1 and cyclooxygenase-2 mRNAs and proteins in human brain and peripheral organs. Brain Res 1999;830:226-36.
12) Lanza FL, Rack MF, Callison DA. A pilot endoscopic study of the gastroduodenal effects of SC-58635, a novel COX-2 selective inhibitor. Gastroenterology 1997;112(Suppl 4):A194.
13) Geiss GS, Hubbard RC, Callison DA, Yu S, Zhao W.
Safty and efficacy of celecoxib, a specific COX-2 inhibitor. Rheumatol Eur 1998;27(Suppl 1):118.
14) Lane NE. Pain management in osteoarthritis: the role of COX-2 inhibitors. J Rheumatol 1997;24:20-4.
15) Lipsky PE, Isakson PC. Outcome of specific COX-2 inhibiton in rheumatoid arthritis. J Rheumatol 1997;
24:9-14.
16) Bae SC, Lee HS, Yun HR, Kim TH, Yoo DH, Kim SY. Cross-cultural adaptation and validation of Korean Western Ontario and McMaster Universities (WOMAC) and Lequesne osteoarthritis indices for clinical re- search. Osteoarthritis Cartilage (in Press)
17) Cho MJ, Kim KH. Diagnostic validity of the CES-D in the assessment of DSM-III-R major depression. J Korean Neuropsychiatr Asso 1993;32:381-97.
18) 김홍근. Rey-Kim 기억검사. 신경심리 1999.
19) 전용신. KWIS 실시요강 1963.
20) Bauer MKA, Lieb K, Schulze-Oxthoff K. Expression and regulation of cyclooxygenase-2 in rat microglia.
Eur J Biochem 1997;243:726-31.
21) Yamagata K, Andreasson KI, Kaufmann WE. Expres- sion of a mitogen-inducible cyclooxygenase-2 in brain
neuron: regulation by synaptic activity and glucocor- ticoids. Neuron 1993;1192:371-86.
22) Lipsky PE. The clinicla potential of Cyclooxygenase- 2-specific inhibitors. Am J Med 1999;106:51S-7S.
23) Rich JB, Rasmusson DX, Folstein MF. Nonsteroidal anti-inflammatory drugs in Alzheimer's disease. Neu- rology 1995;45:51-5.
24) Rogers J, Kirby LC, Hempelman SR. Clinical trial of indomethacin in Alzheimer's disease. Neurology 1993;
43:1609-11.
25) Stewart WF, Kawas C, Corrada M, Metter J. Risk of Alzheimer's disease and duration of NSAID use. Neu- rology 1997;48:626-32.
26) Aisen PS, Davis KL. Inflammatory mechanism in Alzheimer's disease: Implication therapy. Am J Psy- chiatry 1994;151:1105-13.
27) McGeer PL, Rogers J. Anti-inflammatory agents as a therapeutic approach to Alzheimer's disease. Neurol- ogy 1992;42:447-9.
28) In' Tveld BA, Ruitenberg A, Hofman A, Launer LJ, Van Duijn CM, Stijnen T, et al. Nonsteroidal anti- inflammatory drugs and the risk of Alzheimer's dis- ease. N Engl J Med 2001;345:1515-21.
29) Goodwin JS, Regan M. Cognitive dysfunction associ-
ated with naproxen and ibuprofen in the elderly.
Arthritis Rheum 1982;25:1013-5.
30) Joseph TH, Kenneth ES, Lawrence RL, Ronnie DH, Gerda GF, Carl FP, et al. Relation of prescription nonsteroidal antiinflammatory drug use to cognitive function among community-dwelling elderly. Ann Epidemiol 1997;7:87-94.
31) Lobst WF, Bridges CR, Regan-Smith MG. Antirheu- matic agents: CNS toxicity and its avoidance. Geri- atrics 1989;44:95-102.
32) Hoppman RA, Peden JG, Ober SK. CNS side effects of NSAID. Arch Intern Med 1991;51:1309-13.
33) Larson EB, Kukull WA, Buchner D, Reifler BV.
Adverse drug reactions associated with global cogni- tive impairment in elderly person. Ann Intern Med 1987;107:169-73.
34) Wysenbeek J, Klein Z, Nakar S, Mane R. Assesment of cognitive function in elderly patients treated with naproxen: A prospective study. Clin Exp Rheumatol 1988;6:399-400.
35) Franklin EM, Mavy TM, Ronald BS, William EH.
Lack of association of NSAID use and cognitive decline in the elderly. Gerontology 1992;38:275-9.