한국 소아청소년 기면증의 임상양상 및 수면다원검사의 특징
성균관대학교 의과대학 삼성서울병원 소아청소년과학교실1, 신경과학교실2
이지원
1・박유진
1・주은연
2・이지훈
1Submitted: 22 August, 2016 Revised: 19 September, 2016 Accepted: 19 September, 2016 Correspondence to Jeehun Lee, MD, PhD
Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-Ro, Gangnam-Gu, Seoul 06351, Korea Tel: +82-2-3410-0910, Fax: +82-2-3410-0043 E-mail: [email protected]
Clinical and Polysomnographic Characteristics of Childhood Narcolepsy in Korea
Purpose: Diagnosis of narcolepsy in childhood is challenging because of ambiguous expression of symptoms and various clinical presentations. The purpose of this study is to delineate the clinical and polysomnographic characteristics of childhood narcolepsy.
Methods: This study included 78 patients who were diagnosed with narcolepsy by clinical history and polysomnography (PSG) between February 2002 and June 2015 at Samsung Medical Center. Their medical records were reviewed retrospectively and analyzed between two groups; age of symptom onset and the presence of cataplexy.
Results: The age at diagnosis and symptom onset was 15.51±2.73 years and 13.03±
2.79 years. Forty-one patients (52.6%) were diagnosed with narcolepsy with cata- plexy. All exhibited excessive daytime sleepiness as the first symptom. In the multiple sleep latency test (MSLT), short sleep latency and more than 3 episodes of mean sleep onset of rapid eye movement were observed. The coexisting sleep disorders varied according to age of onset. There was no significant difference in sleep para- meters between the two age groups. The patients with cataplexy had higher scores on the Epworth Sleepiness Scale and shorter mean sleep latencies in the MSLT than those without cataplexy (P<0.05).
Conclusion: Pediatric narcolepsy presents with excessive daytime sleepiness and has different co-existing sleep disorders according to age of onset. The degree of sleepiness is higher in the patients with cataplexy. Narcolepsy may be suspected in children with excessive daytime sleepiness even if they do not have cataplexy. This should be confirmed using appropriate sleep questionnaires and PSG with MSLT.
Key Words: Narcolepsy, Children, Polysomnography, Cataplexy
Jiwon Lee, MD1, Eu Gene Park, MD1, Eun Yeon Joo, MD2, Jeehun Lee, MD, PhD1
1Departments of Pediatrics and 2Neurology, Sam
sung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Copyright © 2016 by The Korean Child Neurology Society
http://www.cns.or.kr
Introduction
Narcolepsy is a chronic sleep disorder characterized by the abnormal regula
tion of the sleepwake cycle. The pathophysiology of narcolepsy involves the loss of hypocretin (orexin)producing neurons in the hypothalamus and it is considered to be an autoimmune disease associated with the human leukocyte antigen (HLA) DQB1*06021,2). The four main symptoms of narcolepsy are exces
sive daytime sleepiness, cataplexy, hypnagogic hallucination, and sleep paralysis.
In clinical practice, less than half of all patients show all four symptoms3). This fraction is even lower in pediatric patients4,5). The most common symptom is
excessive daytime sleepiness, which can appear beginning at young ages and may be a clue for the diagnosis of the disease in the initial stages5,6).
The reported incidence of pediatric narcolepsy has increased from 0.26 per 100,000 children in 2009 to 5.3 per 100,000 child
ren in 20107,8). The incidence of this disease in children may be underestimated due to by underdiagnosis. Symptom onset pre
cedes diagnosis by 5 to 10 years in most adult cases. This indi
cates that these patients may have already had a symptom of narcolepsy during childhood9). Recently, narcolepsy has been shown to interfere with the psychosocial aspects of life and affect learning ability, behavior, and mood control10). As the importance of these aspects of the disease has been recog nized, its early diagnosis and prevalence appear to be rising. However, the early diagnosis of narcolepsy in childhood is still challenging due to the ambiguous expression of disease symptoms and daytime sleepiness due to other causes mimicking narcolepsy11). Further
more, narcolepsy without cataplexy may be a big burden for diagnosis without the multiple sleep latency test (MSLT) and there are opinions about this disorder as an arbitrary condition having a different pathologic mechanism12). There is a paucity of studies that have systema tically described the characteristics of child
hood narcolepsy in large numbers of patients. We tried to de
lineate the clinical and polysomnographic characteristics of pe
diatric narcolepsy in Korea. In addition, we attempted to identify distinct features that can be used for early diagnosis by analyzing the differences between groups divided based on age of symp
tom onset and the presence of cataplexy.
Materials and Methods
1. Patients
This study was conducted in a tertiary university hospital in Korea between February 2002 and June 2015. The inclusion criteria of this study were as follows: (1) an age of 19 years or less at the time of polysomnography (PSG), and 2) diagnosis with narcolepsy with or without cataplexy using International Classification of Sleep Disorders, Second Edition (ICSD2) criteria
13). ICSD2 criteria of narcolepsy were as follows: the patient has a complaint of excessive daytime sleepiness for at least 3 months.
And there are short sleep onset latencies less than 8 minutes and more than 2 episodes of sleep onset rapid eye movement (SOREM) of five naps in nocturnal PSG and serial MSLT. The diagnosis of narcolepsy with or without cataplexy depends on a definite history of cataplexy of the patient. Of the 629 patients that under
went PSG for complaints of excessive daytime sleepiness for at
least 3 months, 78 patients (12.4%) were diagnosed with narco
lepsy based on PSG and their clinical characteristics. Clinical data and polysomnographic results of the participants were reviewed retrospectively. These data included gender, age at diagnosis, age at symptom onset, body scales, and questionnaires regarding sleepiness, depression, and sleep habits. The patients were clas
sified into two groups according to the age at symptom onset (before/after puberty [10 years of age]). The age of puberty was based on the 20th edition of the Nelson Textbook of Pediatrics14). The patients were also grouped based on the presence of cata
plexy (with or without cataplexy). Excessive daytime sleepiness was defined based on subjective reports or according to prior studies. Specifically, excessive daytime sleepiness was considered to be present when the parent answered “yes” to “Does your child have a problem with sleepiness during the day?” and/or “Has another supervisor commented that your child appears sleepy during the day?”15)
2. Polysomnography and Questionnaires
All patients or their parents were asked to complete the Ep
worth Sleepiness Scale (ESS), which is a questionnaire composed of eight items scored from 03 (0=never, 1=slight chance, 2=
moderate chance, 3=high chance) used to evaluate the degree of sleepiness16). The Children’s Depression Inventory (CDI) (<13 years) or the Beck Depression Inventory (BDI) (≥13 years) was used to assess the depressive feelings of the patients. The CDI and the BDI are scored from 0 to 54 and 0 to 63, respectively, with more depressive feelings indicated by higher scores. Sleep habits were determined through questionnaires regarding bed
time, wake time, sleep latency, and total sleep time on school nights and weekend nights.
All subjects were evaluated by a onenight PSG using the Embla N7000 and the RemLogic system (Embla Systems, Amsterdam, Netherlands). Patients’ sleep was monitored throughout the night using an electroencephalogram (C3A2, C4A1, O1A2, and O2
A1), bilateral electrooculograms, a chin electromyogram, a singlelead electrocardiogram in a modified V2 lead, a bilateral leg electromyogram, and body position. Sleep and arousal scores were assigned using standard criteria17,18). Sleep and sleep
disorder breathing events were scored according to the 2007 guidelines of the American Academy of Sleep Medicine19).
The MSLT was performed on the day after the overnight PSG.
If patients were taking medications that influenced sleep latency or rapid eye movement (REM) latency, they were advised to stop taking these medications 2 weeks prior to the study. Five nap opportunities were provided, with each nap lasting for 20 mi
nutes and separated by intervals of at least 2 hours20). SOREM
was defined when REM sleep occurred within 15 minutes after sleep onset.
Because the study period was February 2002 to June 2015, all sleep disorders were diagnosed based on the definitions of ICSD2. This study was approved by the institutional review board of Samsung Seoul Hospital (IRB number 201506035002).
3. Statistical Analysis
Quantitative variables were expressed as mean and standard deviation (SD) or numbers with percentage. Comparisons bet
ween the two groups based on age at symptom onset and the presence of cataplexy were performed using Fisher’s exact test or logistic regression analysis. The statistical level for significance was set at 0.05. Statistical analysis was performed using SPSS for Windows, Version 23 (SPSS, Inc., Chicago, IL).
Results
1. Clinical and polysomnographic findings
The patients who participated in this study consisted of 39 females (50%) and 39 males (50%). Their mean total sleep time was 7 hours and 23 minutes on weekdays and 8 hours and 52 minutes on weekends. The age at diagnosis was 15.51±2.73 years (mean±SD, range 5.218.9 years). Symptom onset occurred about 2.5 years prior to diagnosis (13.03±2.79 years). The youn
gest patient was 5.2 years old at diagnosis and her symptom started beginning at the age of 3. The first symptoms were cata
plexy and daytime sleepiness. The patient had difficulty holding her head up. This was accompanied by laughter. The patients expressed higher depressive feelings compared to the normal population (with BDI scores of <10 points). This was indicated by an elevated mean BDI score of 17.74±12.11. The patients also
exhibited subjective daytime sleepiness and an elevated ESS of 11.58±4.01. All patients complained of excessive daytime sleepi
ness as the first symptom of narcolepsy and half of the patients (n=41, 53%) had cataplexy. Specific HLA genotyping was perfor
med in 15 patients (19.2%). Seven of these patients were positive for HLADQB1*0602.
The PSG results indicated that mean sleep latency was shorter than 10 minutes and the arousal index was elevated to 10.62±
4.78 per hour. Sleep efficiencies of less than 80% were recorded in 12 patients (15.4%). All subjects performed the MSLT and showed two or more SOREMs satisfying the diagnostic criteria of narcolepsy. The MSLT results definitively indicated the pre
sence of short sleep latencies. Detailed demographics and sleep study data are summarized in Tables 1 and 2.
2. Treatments
Among the patients who were treated with medications, 67 patients (85.9%) were followed up for more than 3 years (3.23±
3.68 years). Effective medical treatment was reported in 44 pati
ents (65.7%). The most commonly used medication was modafinil (n=20, 29.9%). Other medications employed included methyl
phenidate (n=10, 14.9%) and combination therapy (n=14, 20.9%) using multiple drugs, including modafinil, methylphe nidate, fluo
xetine, and clomipramine. Table 1 details the clinical characteri
stics and polysomnographic data of the patients with narcolepsy.
3. Comparison between the early-onset and late-onset groups The comparisons of clinical and polysomnographic variables between the two age groups are summarized in Table 3. There was no difference in sex distribution between the two groups.
Patients in the earlyonset group exhibited their first symptom at 7.70±1.64 years of age and were diagnosed at 11.26±3.81 years
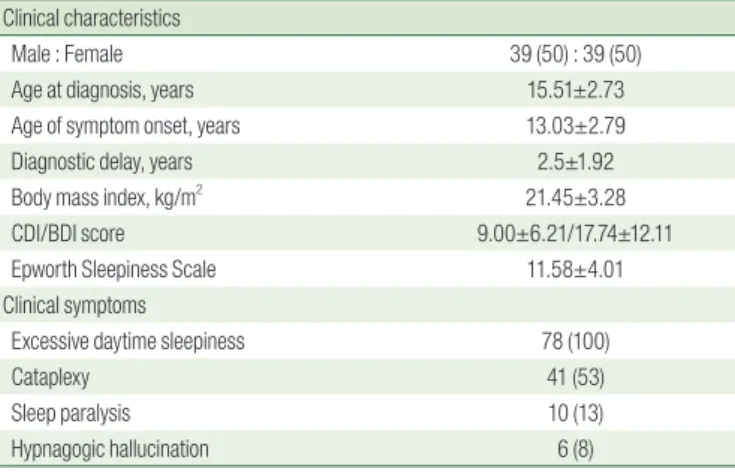
Table 1. Demographics for Children with Narcolepsy Clinical characteristics
Male : Female 39 (50) : 39 (50)
Age at diagnosis, years 15.51±2.73
Age of symptom onset, years 13.03±2.79
Diagnostic delay, years 2.5±1.92
Body mass index, kg/m2 21.45±3.28
CDI/BDI score 9.00±6.21/17.74±12.11
Epworth Sleepiness Scale 11.58±4.01
Clinical symptoms
Excessive daytime sleepiness 78 (100)
Cataplexy 41 (53)
Sleep paralysis 10 (13)
Hypnagogic hallucination 6 (8)
Data are mean±standard deviation or n (%) values.
CDI, Children’s Depression Inventory, reference 0-54; BDI, Beck Depression Inventory, re- ference 0-63; Epworth sleepiness score, reference 0-24.
Table 2. Sleep Descriptors for Children with Narcolepsy Polysomnographic data
Total sleep time, minutes 438.00±43.72
Sleep latency, minutes 8.36±13.24
Arousal index, /hour 10.62±4.78
Sleep efficiency, % 89.77±8.25
REM latency, minutes 75.83±72.18
N1 sleep, % 10.84±7.49
N2 sleep, % 46.60±9.16
Slow wave sleep, % 21.85±7.46
REM sleep, % 20.72±5.09
Multiple Sleep Latency Test
SOREM frequency, n 3.3±1.28
Mean sleep latency, minutes 4.89±3.74
REM latency, minutes 3.94±3.27
Data are mean±standard deviation or n (%) values.
REM, rapid eye movement; SOREM, sleep onset rapid eye movement.
of age. The diagnostic delay was not significantly different bet
ween the early and lateonset groups (P=0.996). Subjective sleepiness propensity was similar in the two groups assessed by ESS. Symptoms associated with sleep paralysis or hypnagogic hallucination were not found in the earlyonset group. Seventeen adolescents had coexisting sleep disorders, such as periodic limb movement disorder (PLMD) or delayed sleep phase disorder (DSPD). Three young children had REM sleep behavior disorders.
There were no significant differences in sleep latency, REM sleep latency, wake after sleep onset (WASO), or SOREM frequency between the age groups (Table 3).
4. Comparison between the narcolepsy with and without cataplexy groups
We divided the patients into two groups based on the presen
ce of cataplexy (n=41 with cataplexy, n=37 without cataplexy) and compared their clinical and polysomnographic variables (Table 4). The sex ratio was different between the two groups.
There were more males in the without cataplexy group, while there were more females in the with cataplexy group. There were no significant differences in mean age of onset and diagnosis, or the time gap from symptom onset to diagnosis of disease. Patients with cataplexy had higher complaints of subjective daytime sleepiness (P<0.05). Specific HLA genotyping was performed in some of the patients in each group (eight cases of narcolepsy
Table 3. Differences between Two Groups according to Age of Symp
tom Onset
Early onset (n=10)
Late onset
(n=68) P-value Clinical characteristics
Male : Female 4 (40) : 6 (60) 35 (51.5) : 33 (48.5) NS
Age at diagnosis, years 11.26±3.81 16.13±1.89 NS
Age of symptom onset, years 7.70±1.64 13.86±1.84 NS
Diagnostic delay, years 3.58±3.05 2.34±1.66 NS
Body mass index, kg/m2 20.40±4.01 21.60±3.16 NS
CDI/BDI score 8.00±1.83 / NA NA / 17.28±12.16 NA
Epworth Sleepiness Scale 11.40±4.22 11.60±4.02 NS
Clinical symptoms
Excessive daytime sleepiness 10 (100) 68 (100) NS
Cataplexy 7 (70) 34 (50.0) NS
Sleep paralysis None 10 (14.7) NA
Hypnagogic hallucination None 6 (8.8) NA
Coexisting sleep disorder
PLMD None 14 (20.6) NA
REM behavior disorder 3 (30) None NA
DSPD None 3 (4.4) NA
Polysomnographic data
Total sleep time, minutes 449.25±44.50 436.35±43.69 NS
Sleep latency, minutes 4.41±3.66 8.95±14.03 NS
REM latency, minutes 57.20±96.35 78.57±68.42 NS
Arousal index, /hour 11.62±2.38 10.48±5.04 NS
Sleep efficiency, % 87.35±8.55 90.13±8.21 NS
N1 sleep, % 13.88±6.78 10.39±7.54 NS
N2 sleep, % 41.20±8.66 47.40±9.02 NS
Slow wave sleep, % 26.32±6.29 21.19±7.43 NS
WASO, % 12.07±8.71 8.26±7.91 NS
Multiple Sleep Latency Test
SOREM frequency, n 4.10±0.74 3.11±1.30 NS
Mean sleep latency, minutes 3.02±1.95 5.17±3.87 NS
Data are mean±standard deviation or n (%) values.
NS, not significance; CDI, Children’s Depression Inventory, reference 0*54; BDI, Beck De- pression Inventory, reference 0-63; NA, not available due to small number of samples;
Epworth sleepiness score, reference 0-24; PLMD, periodic limb movement disorder; REM, rapid eye movement; DSPD, delayed sleep phase disorder; WASO, wake after sleep onset;
SOREM, sleep onset rapid eye movement.
Table 4. Differences between Narcolepsy with and without Cataplexy With cataplexy
(n=41)
Without cataplexy (n=37)
P- value Clinical characteristics
Male : Female 14 (34.1) : 27 (65.9) 25 (67.6) : 12 (32.4) 0.003
Age at diagnosis, years 14.95±3.20 16.13±1.95 NS
Age of symptom onset, years 12.41±3.09 13.76±2.20 NS
Diagnostic delay, years 2.60±1.89 2.39±1.98 NS
Body mass index, kg/m2 21.72±3.12 21.14±3.47 NS
CDI/BDI score 9.63±7.19 /
18.10±11.22
NA/17.48±12.93 NA/NS
Epworth Sleepiness Scale 12.73±3.85 10.30±3.84 0.027 HLA typing
DQB1*0602 positive 6 (75.0)/8† 1 (14.3)/ 7 NA
Treatments
Medical therapy 35 (85.4) 33 (89.2) NS
Effective 22 (65.7) 24 (72.7) NS
No effect 4 (11.4) 3 (9.1) NS
Unknown‡ 8 (22.9) 6 (18.2) NS
Polysomnographic data
Total sleep time, minutes 440.41±43.26 435.35±44.66 NS
Sleep latency, minutes 9.09±16.26 7.56±8.93 NS
REM latency, minutes 55.94±67.50 97.86±71.63 NS
Arousal index, /hour 11.24±4.51 9.94±5.04 NS
Sleep efficiency, % 89.50±7.01 90.07±9.53 NS
N1 sleep, % 12.83±7.94 8.64±6.37 NS
N2 sleep, % 44.74±9.89 48.66±7.90 NS
Slow wave sleep, % 22.00±6.96 21.69±8.07 NS
REM sleep, % 20.43±5.29 21.04±4.91 NS
WASO, % 8.83±7.25 8.65±8.97 NS
Multiple Sleep Latency Test
SOREM frequency, n 3.35±1.42 3.09±1.12 NS
Mean sleep latency, minutes 3.64±3.87 6.24±3.82 0.048
REM latency, minutes 3.46±3.50 4.48±2.95 NS
Data are mean±standard deviation or n (%) values.
NS, not significant; CDI, Children’s Depression Inventory, reference 0-54; BDI, Beck Depres- sion Inventory, reference 0-63; NA, not available due to small number of samples; Epworth sleepiness score, reference 0-24; REM, rapid eye movement; WASO, wake after sleep onset;
SOREM, sleep onset rapid eye movement.
†Number of patients with positive result (%) / total number of patients who performed HLA genotyping. ‡Unknown, impossible to assess the effect of treatment due to follow-up loss.
with cataplexy and seven cases of narcolep sy without cataplexy).
Six of the seven positive results were found in patients with cata
plexy. Medical treatments were established in more than 85% of the patients in both groups. The effectiveness of the treatments was not different. Sixtyfive percent and 73% of the patients in the group with cataplexy and without cataplexy had effective treatment, respectively. The mean frequency of SOREM and mean sleep latency were not different between the two groups.
Discussion
In this study, a considerable number of pediatric patients who had undergone PSG with the complaint of excessive daytime sleepiness (n=629), were diagnosed as narcolepsy (12.4%). Cata
plexy was found in 53% of the patients. Depressive feelings were reported in 36% of the patients. The patients had more than 3 episodes of SOREM on average and their sleep latency was reduced to a mean of 4.89 minutes. There were no signifi cant differences in clinical characteristics and sleep parameters based on age of onset or the presence of cataplexy.
Narcolepsy is chronic hypersomnia presenting as overwhel
ming sleepiness during the daytime and muscle weakness asso
ciated with emotional stimuli. According to previous studies, the peak age of incidence is approximately 15 years21,22). In this study, the mean age at diagnosis was 15.5 years and age at symptom onset was 13.0 years. There were 2.5 years of diagno stic delay, which was shorter than the 510 years reported in other studies
23). Delayed diagnosis of narcolepsy can be negative effect on school performance, quality of life, social function, and economic status4,11). The clinical importance of early diagnosis has been emphasized and various related factors were revealed. The diag
nostic delay has been reported to be associated with age at symptom onset and presenting symptomsinitial absence of cataplexy and number of initial symptoms9). However, another study found that there was no relationship between diagnostic delay and cataplexy, which is consistent with our results24).
The tetrad of symptoms associated with narcolepsy is exces
sive daytime sleepiness, cataplexy, sleep paralysis, and hypna
gogic/hypnopompic hallucination. Of these, excessive daytime sleepiness has been reported to be the most common symptom.
All patients included in this study had excessive daytime sleepi
ness as their first symptom and this was the major cause of the sleep study25,26). Cataplexy, which is a pathognomonic finding in this disorder, was observed in 53% (n=41) of the patients. The reported prevalence of cataplexy diversely ranges from 38% to 75% of all narcolepsy patients27,28). Sleep paralysis and hypna
gogic hallucination was observed in a few patients. It has been postulated that these symptoms are agedependent, with in
creasing incidences in older age29). The short sleep latency indi
cated by the polysomnographic data confirmed that patients with narcolepsy fall asleep easily. The MSLT results were used to confirm the diagnosis of narcolepsy in patients with more than 2 episodes of SOREM. Inocente et al. compared depressive feelings in children with narcolepsy. They compared girls and boys aged 10 years or older. Twentyfive percent of all patients with narco
lepsy were revealed to have depressive feelings as through the evaluated by the CDI. This tendency was more prevalent in girls
10). Disturbances of sleep can negatively affect daily activity, school performance, and mood. We found that approximately onethird (n=28, 36%) of the patients subjectively expressed depressive feelings on the questionnaires. We can assume that sleep dis
orders lead to emotional problems. There were also misdiagnosed cases due to the influence of comorbid conditions, such as con
version disorder, major depressive disorder, and attention deficit hyperactivity disorder30). Therefore, it is necessary that narcolepsy is considered as a differential diagnosis to other psychologic disorders accompa nying excessive daytime sleepiness.
Cataplexy is a distinctive feature of narcolepsy and one of its diagnostic criteria. Many investigators have studied the meaning of cataplexy in narcolepsy patients. In previous studies, patients with cataplexy were shown to have more REM sleep disorders and REMrelated symptoms than those without cataplexy6). In our study, higher ESS scores and shorter mean sleep latencies in the MSLT were observed in the patients having cataplexy (P<
0.05). Similar findings were reported in a previous study31). Mean sleep latency and mean REM latency in the MSLT were signifi
cantly shorter in patients with narcolepsy with cataplexy, and the frequency of SOREM in the MSLT was higher in patients with narcolepsy with cataplexy than in those without cataplexy32).
This study included a large number of pediatric patients diag
nosed with narcolepsy without cataplexy (n=37, 47%). Patients with narcolepsy without cataplexy are considered to be a hete
rogeneous group in terms of clinical presentation and etiology.
Current diagnostic tools, such as PSG with MSLT cannot comple
tely distinguish whether it is narcolepsy or not. According to previous studies, some of these patients have hypocretin defici
encies in their cerebrospinal fluid (CSF) or develop cata plexy after several years and finally were confirmed to the diagnosis with narcolepsy33). The present study had a limitation that the level of hypocretin in the CSF was not measured because it was not available in our institution. According to the previous study, there are patients with borderline of diagnoses and cases in which the diagnosis changes34). The patients in the present study
have potential possibility of being changed the diagnosis of narcolepsy during followup. Therefore, further evaluations is required to establish the diagnoses of these patients and to as
sess their clinical courses by performing followup PSG with MSLT, checking the level of hypocretin in their CSF, and by per
forming HLA genotyping.
In conclusion, narcolepsy frequently arises in adolescence and its diagnosis is started from the clinical suspicion of excessive daytime sleepiness. However, childhood narcolepsy may have atypical presentations different from those observed in adults and is often misdiagnosed as another disorder, such as depres
sion, epilepsy, or a psychologic disorder. Delayed diag nosis of narcolepsy has been shown to affect emotional control, daily ac
tivity, and learning ability in many studies. Our findings revealed distinctive clinical and polysomnographic characte ristics of child
hood narcolepsy and favorable response to medical treatment in more than 65% of the patients. We suggest that PSG accompanied by MSLT examination helps to diagnose patients with narcolepsy and the proper treatments are necessary in the early stages of the disease to decrease socioeconomic burdens. In the future, a longitudinal study including objective diagnostic tools, such as followup MSLT, HLA genotyping, and assessment of the level of hypocretin in the CSF, are needed to provide a better under
standing of childhood narcolepsy.
요약
목적: 소아청소년에서의 기면증은 다양한 양상으로 나타날 수 있 고 환자들이 증상을 모호하게 표현할 수 있어 진단하기 까다로운 질 환이다. 본 연구는 소아청소년의 기면증의 임상 양상 및 수면검사의 특징을 기술하고 발병나이와 탈력발작의 유무에 따른 차이점을 알아 보고자 하였다.
방법: 2002년 2월부터 2015년 6월까지 삼성서울병원에서 병력청취 와 수면다원검사를 통해 기면증을 진단받은 78명의 소아청소년 환자 를 대상으로 의무기록과 수면다원검사 결과를 발병나이와 탈력발작 의 유무에 따라 후향적으로 고찰하였다.
결과: 기면증을 진단받은 나이는 15.51±2.7세였고 증상은 13.03±
2.79세에 시작되었다. 10명(12.8%)의 환자가 10세 이전에 증상발현을 보였고 41명(52.6%)은 탈력발작을 동반한 기면증으로 진단되었다. 모 든 환자가 첫 증상으로 과도한 주간 졸림증을 호소하였고, 수면마비 와 입면환각은 13%와 8%에서 보고되었다. 수면잠복기 반복검사에서 는 짧은 평균 수면잠복기와 평균 3회 이상의 입면 렘수면기가 관찰되 었다. 발병나이에 따라 동반 수면질환의 종류가 다양하였으나, 수면지 표간의 차이는 없었다. 탈력발작을 동반한 기면증 환자들의 경우 탈 력발작을 동반하지 않은 환자들보다 Epworth Sleepiness Scale이 유 의하게 높았으며, 수면잠복기 반복검사에서 평균 수면잠복기가 더 짧
았다(P<0.05).
결론: 소아청소년의 기면증은 과도한 주간졸음을 호소하는 소아에 서 고려해야 할 질환으로 탈력발작이 동반되지 않은 환자가 50% 이 상 이었으며 약 2/3의 환자가 약제에 좋은 치료반응을 보였다. 발병연 령에 따라 동반되는 수면질환의 분포가 다르며, 탈력발작이 동반되는 경우 졸림증이 더욱 심한 특징을 보였다. 수면관련 설문지와 수면다원 검사 및 수면잠복기 반복검사를 통한 정확한 진단, 조기 치료, 그리고 장기간의 추적관찰이 필요하다.
References
1) Liblau RS, Vassalli A, Seifinejad A, Tafti M. Hypocretin (orexin) biology and the pathophysiology of narcolepsy with cataplexy.
Lancet Neurol 2015;14:318-28.
2) Tanaka S, Honda Y, Inoue Y, Honda M. Detection of autoanti- bodies against hypocretin, hcrtrl, and hcrtr2 in narcolepsy: anti- Hcrt system antibody in narcolepsy. Sleep 2006;29:633-8.
3) Bang YW, Chae KY. Pediatric narcolepsy - Diagnosis and treate- ment. J Korean Child Neurol Soc 2009;17:107-17.
4) Babiker MO, Prasad M. Narcolepsy in children: a diagnostic and management approach. Pediatr Neurol 2015;52:557-65.
5) Dias Costa F, Barreto MI, Clemente V, Vasconcelos M, Estêvão MH, Madureira N. Narcolepsy in pediatric age - Experience of a tertiary pediatric hospital. Sleep Sci 2014;7:53-8.
6) Nevsimalova S, Pisko J, Buskova J, Kemlink D, Prihodova I, Sonka K,et al. Narcolepsy: clinical differences and association with other sleep disorders in different age groups. J Neuro 2013;260:767-75.
7) Szakács A, Darin N, Hallböök T. Increased childhood incidence of narcolepsy in western Sweden after H1N1 influenza vaccina- tion. Neurology 2013;80:1315-21.
8) Partinen M, Saarenpää-Heikkilä O, Ilveskoski I, Hublin C, Linna M, Olsén P, et al. Increased incidence and clinical picture of child- hood narcolepsy following the 2009 H1N1 pandemic vaccination campaign in Finland. PLoS One 2012;7:e33723.
9) Morrish E, King MA, Smith IE, Shneerson JM. Factors associated with a delay in the diagnosis of narcolepsy. Sleep Med 2004;5:37- 41.
10) Inocente CO, Gustin MP, Lavault S, Guignard-Perret A, Raoux A, Christol N, et al. Depressive feelings in children with narcolepsy.
Sleep Med 2014;15:309-14.
11) Thorpy MJ, Krieger AC. Delayed diagnosis of narcolepsy: charac- terization and impact. Sleep Med 2014;15:502-7.
12) Nakamura M, Nishida S, Hayashida K, Ueki Y, Dauvilliers Y. Dif- ferences in brain morphological findings between narcolepsy with and without cataplexy. PLoS One 2013;28:e81059.
13) Medicine AAoS. International classification of sleep disorders:
diagnostic and coding manual, 2nd ed. Westchester, IL. American Academy of Sleep Medicine. 2005.
14) Robert MK, Bonita FS, Joseph W St Geme III, Nina FS. Adolescent
development. In: Cynthia H-H, Burstein GR, eds. Nelson Text- book of Pediatrics. 20th ed. Philadelphia: Elsevier, 2015:926.
15) Calhoun SL, Vgontzas AN, Fernandez-Mendoza J, Mayes SD, Tsaoussoglou M, Basta M, et al. Prevalence and risk factors of excessive daytime sleepiness in a community sample of young children: the role of obesity, asthma, anxiety/depression, and sleep. Sleep 2011;34:503-7.
16) Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 1991;14:540-5.
17) Hori T, Sugita Y, Koga E, Shirakawa S, Inoue K, Uchida S, et al.
Proposed supplements and amendments to 'A Manual of Stan- dardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects', the Rechtschaffen & Kales (1968) standard. Psychiatry Clin Neurosci 2001;55:305-10.
18) American Sleep Disorders Association and Sleep Research Society. EEG arousals: scoring rules and examples: a preliminary report from the Sleep Disorders Atlas Task Force of the American Sleep Disorders Association. Sleep 1992;15:173-84.
19) American Academy of Sleep Medicine. The AASM manual for the scoring of sleep and associated events; rules terminology and technical specifications; 2007:1-59.
20) Carskadon MA, Dement WC, Mitler MM, Roth T, Westbrook PR, Keenan S. Guidelines for the multiple sleep latency test (MSLT):
a standard measure of sleepiness. Sleep 1986;9:519-24.
21) Hintze JP, Paruthi S. Sleep in the Pediatric Population. Sleep Med Clin 2016;11:91-103.
22) Dauvilliers Y, Montplaisir J, Molinari N, Carlander B, Ondze B, Besset A, et al. Age at onset of narcolepsy in two large populations of patients in France and Quebec. Neurology 2001;57:2029-33.
23) Parkes JD, Clift SJ, Dahlitz MJ, Chen SY, Dunn G. The narcoleptic syndrome. J Neurol Neurosurg Psychiatry 1995;59:221-4.
24) Frauscher B, Ehrmann L, Mitterling T, Gabelia D, Gschliesser V, Brandauer E, et al. Delayed diagnosis, range of severity, and multiple sleep comorbidities: a clinical and polysomnographic
analysis of 100 patients of the innsbruck narcolepsy cohort. J Clin Sleep Med 2013;9:805-12.
25) Carter LP, Acebo C, Kim A. Patients' journeys to a narcolepsy diagnosis: a physician survey and retrospective chart review.
Postgrad Med 2014;126:216-24.
26) Peterson PC, Husain AM. Pediatric narcolepsy. Brain Dev 2008;
30:609-23.
27) Jambhekar SK, Com G, Jones E, Jackson R, Castro MM, Knight F, et al. Periodic limb movements during sleep in children with narcolepsy. J Clin Sleep Med 2011;7:597-601.
28) Heier MS, Gautvik KM, Wannag E, Bronder KH, Midtlyng E, Kamaleri Y, et al. Incidence of narcolepsy in Norwegian children and adolescents after vaccination against H1N1 influenza A.
Sleep Med 2013;14:867-71.
29) Rocca FL, Pizza F, Ricci E, Plazzi G. Narcolepsy during Childhood:
An Update. Neuropediatrics 2015;46:181-98.
30) Kauta SR, Marcus CL. Cases of pediatric narcolepsy after mis- diagnoses. Pediatr Neurol 2012;47:362-5.
31) Leu-Semenescu S, De Cock VC, Le Masson VD, Debs R, Lavault S, Roze E, et al. Hallucinations in narcolepsy with and without cataplexy: contrasts with Parkinson’s disease. Sleep Med 2011;
12:497-504.
32) Sasai T, Inoue Y, Komada Y, Sugiura T, Matsushima E. Compari- son of clinical characteristics among narcolepsy with and without cataplexy and idiopathic hypersomnia without long sleep time, focusing on HLA-DRB1*1501/DQB1*0602 finding. Sleep Med 2009;10:961-6.
33) Andlauer O, Moore H 4th, Hong SC, Dauvilliers Y, Kanbayashi T, Nishino S, et al. Predictors of hypocretin (orexin) deficiency in narcolepsy without cataplexy. Sleep 2012;35:1247-55F.
34) Šonka K, Šusta M, Billiard M. Narcolepsy with and without cata- plexy, idiopathic hypersomnia with and without long sleep time:
a cluster analysis. Sleep Med 2015;16:225-31.