서 론
부신피질 종양, 특히 호르몬을 분비하는 종양은 고알도스 테론증(hyperaldosteronism) 을 일으켜 혈중 칼륨 농도를 저하시켜 주기마비와 비슷한 근력약화를 유발 할 수 있다.
중증근무력증 역시 간헐적 근위약을 일으키나 주로 흉선종
을 동반한 자가면역질환이다. 몇몇 저자들은 고알도스테론 혈증을 동반한 중증근무력증을 보고하였으나 우연한 동반 인지 서로 연관된 병인지 밝히지는 못하였다.1,2
저자들은 복시를 주소로 방문하여 중증근무력증 검사도중 우연히 부신피질종양을 발견하고, 종양 제거 수술 후 호전된 환자 1례를 경험하였기에 보고하는 바이다.
증 례
55세 남자가 2년 전부터의 복시를 호소하며 방문하였다.
환자는 피곤할 때 신호등이 겹쳐 보인다 하였다. 환자는 10 여년 전부터 조절되지 않는 고혈압으로 3가지 이상의 항 고 혈압제를 사용하였으며 이뇨제는 사용하지 않고 있었다. 3년
부실피질 종양과 동반된 중증근무력증 -증례 보고-
이채영, 김보희, 최 봄, 황보송, 민양기
한림대학교 강남성심병원 신경과
Myasthenia Gravis Accompanied by Adrenal Gland Tumor -A Case Report -
Chae-Young Lee, Bo-Hee Kim, Boem Choi, Song Hwangbo, Yang-Ki Minn
Department of Neurology, Kangnam Sacred Heart Hospital, Hallym University, Seoul, Korea
Received August 13, 2015
Revised (1st) August 27, 2015, (2nd) September 9, 2015, (3rd) September 10, 2015
Accepted September 10, 2015 Corresponding Author: Yang-Ki Minn
Department of Neurology, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, 1 Shingil-ro, Yeoungdeungpo-gu, Seoul 07441, Korea
Tel: 82-2-829-5125, Fax: 82-2-847-1617, E-mail: [email protected]
It is unknown that hormone secreting adrenal gland can cause myasthenia gravis. Case: 55 year old man visited our clinic due to episodic diplopia which aggravated at evening. He had long standing uncontrolled hypertension and taken antihypertensive drug without thiazide. One and 3 year before visiting, he had history of transient quadriparesis with hypokalemia (Potassium level 1.9 mmol/L). Antiacethycholinereceptor antibody test was negative. Repetitive nerve stimulation showed generalized decremental response. Left adrenal gland mass was detected at chest CT scan incidentally. Hormonal test was compatible with primary hyperaldosteronism. Left adrenalectomy was done. Repetitive nerve stimulation test which was taken after surgery did not show decremental response. Active hormone secreting adrenal tumor may be cause of secondary myasthenia gravis. More extensive chest CT scan for cover adrenal glands must need in myasthenia with uncontrolled hypertension.
Key Words: hypokalemic periodic paralysis, myasthenia gravis, primary hyperaldosteronism
Copyright © by Korean Association of EMG Electrodiagnostic Medicine
This is an Open Ac cess article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
CASE REPORT
ISSN 1229-6066 http://dx.doi.org/10.18214/jkaem.2015.17.2.86 J Korean Assoc EMG Electrodiagn Med 17(2):86-88, 2015
J Korean Assoc
Electrodiagn Med EMG
87
Chae-Young Lee, et al. Myasthenia Gravis Accompanied by Adrenal Gland Tumor
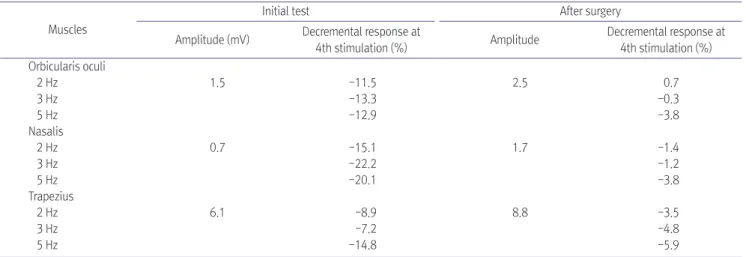
전과 1년 전 2차례 저칼륨혈증을(K 1.9 mmol/L) 동반한 일시적인 사지 근력 위약이 있었다. 중증근무력증 의심 하 에 항아세칠콜린수용체항체 검사, 반복신경자극검사. 흉부 CT 촬영을 시행하였다. 항아세칠콜린수용체항체는 검출되 지 않았으나 눈둘레근(oricularis oculi), 비근(nasalis), 등세 모근(trapezius)에서 실시한 반복신경자극검사에서 저 빈도 자극 감소반응을 보여 중증근무력증으로 진단하였다(Table 1). 흉선종 감별을 위해 촬영한 흉부 CT 촬영상 흉선종은 관 찰되지 않았으나 우연히 2 cm 크기의 좌측 부신 종양이 발견 되었다(Fig. 1). 이어 시행한 부신정맥채혈(adrenal venous sampling), 식염수부하검사(saline loading test), 레닌자극 검사에서 원발성고알도스테론증으로 진단받아 부신제거술 을 시행하였다. 병리조직검사결과 부신피질선종(adrenal cortical adenoma) 소견이 관찰되었다. 수술 후 저칼륨혈증 은 호전되었으며(4.0 mmol/L) 수술 후 1개월째 시행한 반복 신경자극검사에서 기존에 보이던 저 빈도자극 감소반응은 관 찰되지 않았으며 복시도 호소하지 않고 있다(Table 1).
고 찰
고알도스테론증은 저칼륨혈증을 일으켜 일시적인 근위약 을 일으키기 때문에 중증근무력증과 감별 할 필요가 있다.
본 환자는 과거력상 두 차례의 저칼륨주기마비를 일으킨 과 거력이 있어 주기마비의 오진으로 생각 할 수도 있다. 그러 나 저칼륨주기마비는외안근 등 얼굴의 근육을 침범하지 않 기 때문에 복시가 나타나지 않으며 반복신경자극 검사에서 도 이상을 보이지 않는다.3 본 증례에서는 복시를 호소하였 고 몸 근육 뿐만 아니라 얼굴 근육들에서도 반복신경자극검
사 감소반응이 보였기 때문에 주기마비의 오진으로 생각하 기는 어렵다. 하나의 근육 뿐만아니라 3개의 근육에서 감소반 응을 보여 반복신경자극검사의 기술적 오류도 가능성이 낮을 것으로 생각된다. 일반적으로 감수성은 떨어지나 기술적 오류 가 적어 신뢰도가 높은 근육으로 알려진 등세모근에서 양성이 나왔기 때문에 더욱 기술적 오류라 생각하기 어렵다.4
고알도스테론증이 어떻게 중증근무력증과 연관되어 있는 지 현재까지 알려지지는 않았다. 고알도스테론증 자체 보다 는 저칼륨혈증으로 인한 근 손상이 중증근무력증을 악화시 켰다는 보고도 있으나 이것은 고알도스테론증이 중증근무 력증을 악화시켰다는 것이지 원인이라는 보고는 아니다.2 부 신피질 종양이 흉선종 혹은 흉선비대와 동반되었다는 보고
Table 1. Repetitiver Nerve Stimulation Test, before and after Surgery Muscles
Initial test After surgery
Amplitude (mV) Decremental response at
4th stimulation (%) Amplitude Decremental response at 4th stimulation (%) Orbicularis oculi
2 Hz 1.5 -11.5 2.5 0.7
3 Hz -13.3 -0.3
5 Hz -12.9 -3.8
Nasalis
2 Hz 0.7 -15.1 1.7 -1.4
3 Hz -22.2 -1.2
5 Hz -20.1 -3.8
Trapezius
2 Hz 6.1 -8.9 8.8 -3.5
3 Hz -7.2 -4.8
5 Hz -14.8 -5.9
Fig. 1. About 2cm sized low density lesion in left adrenal gland (arrow) was seen in CT scan.
88 J Korean Assoc EMG Electrodiagn Med Vol. 17, No. 2, Dec. 2015
들이 있어 흉선과 관련된 자가면역 반응이 주기마비를 일으 켰다는 가설도 있다.2,5,6
정확한 기전은 알 수 없지만 부신피질 종양 제거가 환자를 호전시켰으므로 직간접적으로 고알도스테론증이 중증근무 력증을 일으켰으리라 생각된다. 본 환자에서는 스테로이드 치료나 흉선제거 수술 등 면역치료를 시행하지 않았기 때문 에 자가 면역이 중증근무력증에 영향을 미쳤으리라 생각 되 지 않는다. 가능한 기전으로는 환자가 무증상 중증근무력증 이 있고 여기에 저칼륨혈증으로 인하여 중증근무력증 증상 이 발현 되었을 가능성이 있다. 이 경우 좀더 긴 시간을 가지 고 증상이 다시 재발하는지 관찰 할 필요가 있겠다.
중증근무력증 환자 특히 성인에서는 흉부 CT 촬영이 필수 적인 검사이다. 중증근무력증 환자에서 특히 조절 안 되는 고 혈압을 동반할 경우 흉부CT 촬영 시 가슴세로칸 뿐만 아니라 부수적으로 촬영되는 부신도 면밀히 관찰 할 필요가 있겠다.
References
1. Inada M, Nishikawa M, Oishi M, Kurata S, Ogawa H, Saku- rami T, et al.: Bartter's syndrome associated with graves' disease and myasthenia gravis: Report of a case. Endocrinol Jpn 1978: 25: 485-492
2. Yamashita S-i, Tsuchimochi W, Yonekawa T, Yamaguchi H, Kyoraku I, Shiomi K, et al: Myasthenia gravis complicated with primary aldosteronism and hypokalemic myopathy.
Intern Med 2009: 48: 1465-1469
3. Raja Rayan DL, Hanna MG: Skeletal muscle channelopathies:
nondystrophic myotonias and periodic paralysis. Curr Opin Neurol 2010: 23: 466-476
4. Suh BC, Kim GS, Choi BO, Cheon HW, Kim SM, Sunwoo IN.
Diagnostic sensitivity of repetitive nerve stimulation test on individual muscles analysis of 357 cases with myasthenia gravis. J Korean Association of EMG Electrodiagnostic Medicine 1999: 1: 150-155
5. Khan MF, Binder J, Dogan S, Bentas W, Aybek T, Wimmer- Greinecker G: First report on sequential totally endoscopic thymomectomy and adrenalectomy using computer- enhanced telemanipulation. Surg Endosc 2003: 17: 1496- 1496
6. Yang R, Jurkat-Rott K, Cao J,Wang G, Seeing HP, Yang C, et al.: Hypokalemic periodic paralysis induced by thymic hyperplasia and relieved by thymectomy. JAMA Neurol 2013:
70: 1436-1439