<접수일:2007년 12월 28일, 심사통과일:2008년 2월 21일>
※통신저자:이 영 호
서울시 성북구 안암동 5가 126-1번지 고려대학교 안암병원 류마티스내과
Tel:02) 920-5645, Fax:02) 922-5974, E-mail:[email protected]
Diagnostic Accuracies of Anti-cyclic Citrullinated Peptide Antibody and Rheumatoid Factor in Korean Patients with Rheumatoid Arthritis:
A Meta-analysis
Young Ho Lee, M.D., Jin Hyun Woo, M.D., Seong Jae Choi, M.D., Jong Dae Ji, M.D., Gwan Gyu Song, M.D.
Division of Rheumatology, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea
= Abstract =
한국인 류마티스관절염 환자에서 항CCP항체와 류마티스인자의 진단정확성에 대한 메타분석연구
고려대학교 의과대학 류마티스내과학교실 이영호ㆍ우진현ㆍ최성재ㆍ지종대ㆍ송관규
목적: 한국인 류마티스관절염 환자에서 항CCP항체와 류마티스인자의 민감도와 특이도, 진단정 확성에 대해 연구하였다.
방법: 문헌검색은 Medline과 Koreamed, 대한류마티스학회지를 이용하였고 논문들의 참고문헌도 조사하였다. Random-effects 모델을 이용하여 메타분석을 시행하였으며 항CCP항체와 류마티스인 자의 민감도, 특이도, positive와 negative likelihood ratios (PLR, NLR), diagnostic odds ratio (DOR)와 summary receiver-operating characteristic curve (SROC 커브)를 구하였다.
결과: 항CCP항체와 류마티스인자의 민감도와 특이도를 연구한 7개의 논문의 류마티스관절염 환자 1,041명과 대조군 970명이 메타분석에 포함되었다. 항CCP항체의 민감도와 특이도, PLR, NLR, DOR은 76.7% (95% confidence interval [CI] 74.0∼79.2), 95.1% (93.8∼96.3), 14.837 (11.567∼
19.031), 0.244 (0.202∼0.294)과 59.235 (43.806∼80.097)이었고 류마티스인자의 수치는 78.2% (0.756
∼0.807), 80.5% (78.1∼82,6), 3.687 (3.027∼4.492), 0.298 (0.218∼0.406)과 12.915 (8.427∼19.771)이 었다. 항CCP항체의 area under the curve (AUC)와 Q* index는 0.9453과 0.8842이었고 류마티스인자
의 수치들은 0,8583과 0.7891이었다. 항CCP항체는 류마티스인자와 비교하여 특이도와 PLR, DOR, AUC, Q* index가 높았으며 민감도와 NLR은 유사하였다. 항CCP항체와 류마티스인자가 모두 양성 인 경우 특이도와 AUC가 류마티스인자에 비해 현저히 증가하였다(특이도 96.5% vs. 80.5%, AUC 0.9864 vs. 0.8583).
결론: 한국인에서 항CCP항체는 류마티스인자와 비슷한 민감도를 보이나 특이도와 진단 정확성 은 더 높았고 항CCP항체와 류마티스인자를 같이 검사하는 경우 항CCP항체나 류마티스인자보다 진단정확성이 증가하여 한국인 류마티스관절염 진단에 유용할 것으로 보인다.
Key Words: Rheumatoid arthritis, Anti-CCP, RF, Meta-analysis
INTRODUCTION
Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized by chronic inflammation of the synovial joints that leads to disability and loss of quality of life (1). The early diagnosis of RA is important, because joint damage can be prevented and prognosis can be improved by early treatment (2).
Currently, RA is diagnosed using the classification criteria of the American College of Rheumatology (ACR) (3), but these criteria are unsuitable for the early diagnosis of RA (4).
Rheumatoid factor (RF) is an antibody directed against the Fc portion of IgG, which has been used as a diagnostic marker for RA. Although RF is the only serological test in the ACR criteria, it is nonspecific and may be present in healthy individuals or in those with other autoimmune diseases (5). The most specific RA autoantibody system known is directed against citrullinated antigens (6). However, several new anti- bodies have been studied in RA, such as, the anti- bodies of filaggrin, keratin, and fibrin, but not all have been successfully incorporated into routine clinical practice despite their high specificities, because their detections are technically demanding (7). The epitopes of their antigens are arginyl residues citrullinated by peptidyl arginine deiminase (8). To improve RA diagnostic sensitivity, assays based on cyclic citrulli- nated peptide (CCP) were developed to detect anti- CCP antibody, which appears to be useful for diag- nosing RA (9). Although previous meta-analyses have
shown that anti-CCP antibody has similar sensitivity to and higher specificity than RF for diagnosing RA (10,11), it remains unclear if the diagnostic values of these antibodies are dependent on ethnicity.
To assess the diagnostic accuracies of anti-CCP antibody and RF for the diagnosis of RA in a Korean population, we performed this meta-analysis using published data, on the sensitivities and specificities of anti-CCP antibody and RF for the diagnosis of RA in Koreans.
MATERIALS AND METHODS
1. Identification of eligible studies and data ex- traction
We performed an exhaustive search for studies that examined anti-CCP antibody, RF, or both for the diagnosis of RA in Koreans. This analysis concerned Korean patients with RA, control populations of healthy subjects, and patients with other rheumatic diseases. We searched Medline and Koreamed and the Journal of Korean Rheumatism Association to identify suitable articles in which anti-CCP antibody and/or RF were determined in Korean RA patients and controls.
Furthermore, all cited references in these studies were reviewed to identify additional works not indexed by electronic databases. The following key words and subject terms were searched: ‘anti-cyclic citrullinated peptide', ‘CCP', ‘rheumatoid factor', ‘RF', ‘rheumatoid arthritis', ‘RA', ‘Korea', and ‘Korean'. We included studies that provided sufficient data to allow sensitivity and specificity for a diagnosis of RA to be calculated.
Fig. 1. Flow diagram of study selection. Articles reported the diagnostic value of anti-CCP antibody and RF testings for RA.
We extracted author, publication year, and the demo- graphic characteristics of participants (total subject numbers, ages, and the percentages of female patients) from each study. Anti-CCP antibody and RF raw data were extracted from all primary studies to fill the four cell values of a diagnostic 2×2 table (true positives, false positives, true negatives, and false negatives).
2. Evaluation of statistical associations
We used 2 meta-analysis methods to assess the overall diagnostic of anti-CCP antibody and RF. A random-effects model was used to combine sensitivity, specificity, positive and negative likelihood ratios (PLR, NLR) and diagnostic odds ratio (DOR) estimates and summary receiver-operating characteristic curves (SROC) were analyzed. DOR is a unitary measure of diagnostic performance that encompasses both sensi- tivity and specificity or both PLR and NLR, and DOR is regarded as a suitable global measure of accuracy for comparing the overall diagnostic accuracies of different tests (12). Because sensitivity and specificity are inter-dependent variables, independent calculations may sometimes underestimate both. SROC curve analysis is more appropriate because it accounts for this mutual dependence. SROC analysis is used for a summary estimate of the performance of a diagnostic test. This technique can overcome some of the
limitations associated with pooling the sensitivities and specificities of published studies. The SROC curve is initially constructed by plotting the sensitivity (true positivitiy) and false positivity (1-specificity) of each study. After mathematical manipulation of the true and false positivities, linear regression is performed to calculate the slope and y-intercept. These coefficients are then entered into the SROC equation to generate SROC. Area under the curve (AUC) (in this case, area under the SROC curve) presents an overall summary of test performance and displays the trade-off between sensitivity and specificity, and an AUC of 1.0 (100%) indicates perfect discriminatory ability for a diagnostic test (13). In addition, the Q* index is another useful global estimate of test accuracy for comparing SROC curves. The Q* index, is defined at that point where sensitivity equals specificity on an SROC curve, and is the point on a SROC curve intersected by the anti- diagonal. A Q* value of 1.0 indicates 100% accuracy (i.e., sensitivity and specificity of 100%) (13).
We assessed within- and between-study variations or heterogeneities by applying Cochran's Q-statistic (14), and the effect of heterogeneity was quantified by using a recently developed measure, i.e., I2=100%×(Q−df)/Q (15). I2 measures the degree of inconsistency between studies by calculating whether the percentage of total variation across studies is due to heterogeneity rather
T1
Table 1. Characteristics of individual studies included in meta-analysis NumbersMean age, yrs (range)Female (%)Anti-CCPRF Author Year RAControlRAControlRAControlSensitivity*Specificity* Sensitivity*Specificity* Song2007 48OA52.251.089.6860.8960.9600.7710.880 et al 50(0.773∼0.965)(0.863∼0.995)(0.627∼0.880)(0.757∼0.995) Park2007262NRANANA80.973.80.8090.9100.9080.721 et al 122(0.756∼0.855)(0.844∼0.954)(0.867∼0.940)(0.633∼0.799) Kim2006114NRA51.1NA83.3NA0.6750.9600.6580.847 et al 202(23∼80)(0.581∼0.760)(0.923∼0.983)(0.563∼0.744)(0.789∼0.893) Choi2005324NRA/HC5153.4 (4∼90)/84.983.7/0.7280.9570.8060.821 et al 251/28(22∼83)50.4 (1∼72)53.8(0.676∼0.776)(0.936∼0.973)(0.758∼0.847)(0.786∼0.853) Kim2005110NRA/HC50.0NA81.8NA0.8000.9470.7180.829 et al 30/46(17∼78)(0.713∼0.870)(0.871∼0.985)(0.624∼0.800)(0.725∼0.906) Kim HR2005 49NRA/HCNANANANA0.8160.9550.9640.755 et al 104/51(0.680∼0.912)(0.909∼0.982)(0.546∼0.817)(0.679∼0.820) Kang2003134NRA/HCNANANANA0.7610.9420.6720.744 et al 53/33(0.680∼0.831)(0.870∼0.981)(0.585∼0.750)(0.639∼0.832) Total1,041970 RA: rheumatoid arthritis, OA: osteoarthritis, NRA: non-RA rheumatic diseases, HC: healthy control, NA: not available *1 means 100% in sensitivity and specificity
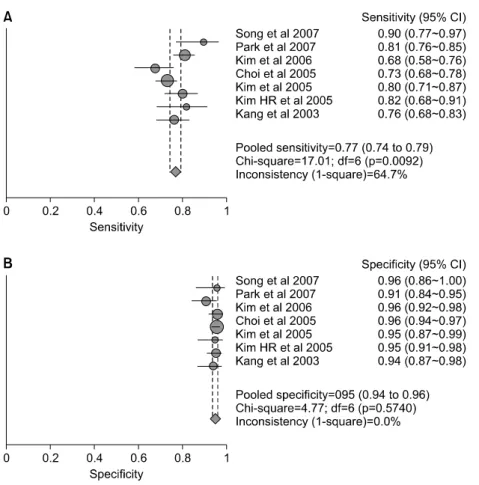
Fig. 2. Sensitivity (A) and specificity (B) estimates for anti-CCP antibody for the diagnosis of RA. Circles and lines represent point estimates and 95% CIs, respectively. Circle areas represent relative study sizes. 1 means 100% in sensitivity and specificity.
than chance. I2 ranges between 0 % and 100% and represents the proportion of between-study variability that can be attributed to heterogeneity rather than chance. I2 values of 25%, 50%, and 75% were des- cribed as low, moderate, and high estimates. Statistical manipulations for this meta-analysis were undertaken using MetaDiSc, version 1.4 (Hospital Universitario Ramony Cajal, Madrid, Spain) (16).
RESULTS
1. Studies included in the meta-analysis
We identified 19 studies by electronic and manual
searching, and 10 were selected for full-text review based on title and abstract. However, three were excluded; one was a review (no case-control study), another had no control data, and the third contained duplicated data (17) (Fig. 1). The seven studies met our study inclusion criteria, included 1,041 patients and 970 controls, and reported on the diagnostic accuracies of anti-CCP antibody and RF (17-23). Mean ages of RA patients ranged from 50.0 to 52.2 yrs and percentages of female patients from 80.9% to 89.6%.
The characteristics of the control groups varied. Two used patients with non-RA rheumatic diseases (NRA), 1 osteoarthritis (OA) patients, and 4 enrolled a mix of
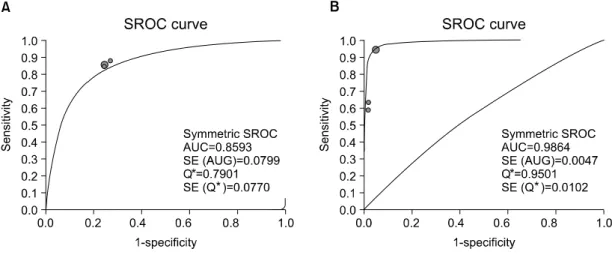
Table 2. Summary results of meta-analysis in RA vs. NRA
(A)
Study
Antibody Comparison Sensitivity* Specificity* PLR NLR DOR
No.
Anti-CCP RA vs NRA 7 0.767 0.951 14.837 0.244 59.235
(0.740∼0.792) (0.938∼0.963) (11.567∼19.031) (0.202∼0.294) (43.806∼80.097)
RF RA vs NRA 7 0.782 0.805 3.687 0.298 12.915
(0.756∼0.807) (0.781∼0.826) (3.027∼4.492) (0.218∼0.406) (8.427∼19.771)
Anti-CCP RA vs NRA 3 0.852 0.745 3.374 0.197 17.565
or RF (0.818∼0.882) (0.703∼0.784) (2.868∼3.970) (0.158∼0.245) (12.462∼24.758)
Anti-CCP RA vs NRA 3 0.794 0.965 22.230 0.212 158.46
and RF (0.752∼0.832) (0.944∼0.980) (13.727∼36.001) (0.056∼0.810) (52.804∼475.54) RA: rheumatoid arthritis, NRA: non-RA rheumatic diseases, HC: healthy control, PLR: positive likelihood ratio, NLR: negative likelihood ratio, DOR: diagnostic OR
*: 1 means 100% in sensitivity and specificity
(B)
Antibody Comparison Study No. AUC SE (AUC) Q* SE (Q*)
Anti-CCP RA vs NRA 7 0.9453 0.0204 0.8842 0.0266
RF RA vs NRA 7 0.8583 0.0179 0.7891 0.0172
Anti-CCP or RF RA vs NRA 3 0.8593 0.0799 0.7901 0.0770
Anti-CCP and RF RA vs NRA 3 0.9864 0.0102 0.9501 0.0102
NRA: non-RA rheumatic diseases, AUC: area under the curve, SE: standard error healthy persons and patients with other diseases. The
characteristic features of study participants included studies in the meta-analysis are given in Table 1.
Studies on anti-CCP antibody and RF showed a wide range of sensitivities and specificities.
Enzyme-linked immunosorbent assay (ELISA) was used to measure anti-CCP antibody in all studies, but the laboratory techniques used for measuring RF varied across studies; 4 studies used immunoturbididometry, 1 a latex fixation test, 1 immuno-nephelometry, and 1 ELISA. Of the 7 RF studies, 5 studies measured RF levels and two tested IgM RF.
2. Diagnostic accuracy of anti-CCP antibody and RF in RA vs NRA
When all 7 studies were considered together, sensitivity estimates of anti-CCP antibody ranged from
68% to 90% and the specificity estimates from 91% to 96% (Table 1). On the other hand, the sensitivity estimates of RF ranged from 66% to 96% and speci- ficity estimates from 72% to 88% (Table 1). The pooled sensitivity and specificity of anti-CCP antibody were 76.7% (95% confidence interval [CI] 74.0∼79.2) and 95.1% (93.8∼96.3), respectively, and for RF were 78.2% (75.6∼80.7) and 80.5% (78.1∼82.6) (Fig. 2).
We found heterogeneity among studies for RF sen- sitivity and specificity and for anti-CCP antibody sen- sitivity but not its specificity. Summarizing, for anti- CCP antibody PLR, NLR, and DOR were 14.837 (11.567∼19.031), 0.244 (0.202∼0.294), and 59.235 (43.806∼80.097), respectively, for RF were 3.687 (3.027∼4.492), 0.298 (0.218∼0.406), and 12.915 (8.427∼19.771), respectively (Table 2). Fig. 3 shows the performance of anti-CCP antibody and RF testings
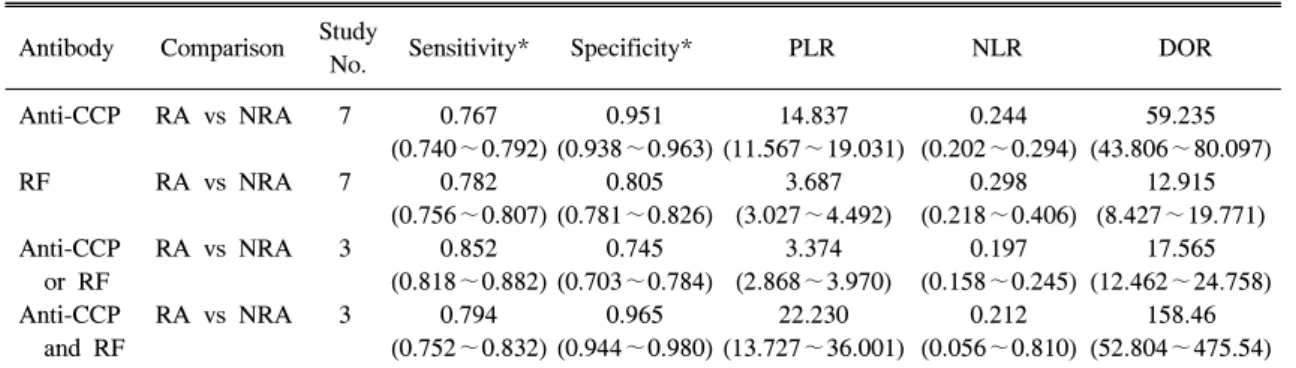
Fig. 3. SROC curves for anti-CCP antibody (A) and for RF (B) for the diagnosis of RA Solid circles represent individual studies included in this meta-analysis. The curve shown is a regression line that summarizes overall diagnostic accuracy. SE (AUC), standard error of AUC, Q*, an index defined by the point on the SROC curve where the sensitivity and specificity are equal; SE (Q*), Q* index standard error.
Table 3. Summary results of meta-analysis in RA vs. HC
(A)
Study
Antibody Comparison Sensitivity* Specificity* PLR NLR DO
No.
Anti-CCP RA vs NRA 4 0.755 0.988 52.791 0.252 217.14
(0.719∼0.789) (0.972∼0.996) (23.009∼121.12) (0.218∼0.290) (91.287∼516.49)
RF RA vs NRA 3 0.757 0.847 4.715 0.321 15.714
(0.720∼0.792) (0.805∼0.882) (1.737∼12.802) (0.201∼0.514) (3.596∼68.666) RA: rheumatoid arthritis, NRA: non-RA rheumatic diseases, HC: healthy control, PLR: positive likelihood ratio, NLR: negative likelihood ratio, DOR: diagnostic OR
*: 1 means 100% in sensitivity and specificity
(B)
Antibody Comparison Study No. AUC SE (AUC) Q* SE (Q*)
Anti-CCP RA vs HC 4 0.9382 0.1089 0.8752 0.1365
RF RA vs HC 3 0.8042 0.0868 0.7396 0.0763
HC: healthy control, AUC: area under the curve, SE: standard error
in the form of SROC curves. The AUC of anti-CCP antibody was 0.9453, and its Q* index was 0.8842, which indicated that the diagnostic accuracy of anti- CCP antibody in Korean RA patients is higher than that of RF. For the AUC of RF was 0.8583, and its
Q* index 0.7891, indicating modest accuracy.
3. Diagnostic accuracy of anti-CCP antibody and RF in RA vs HC
Data that were limited to studies of healthy controls
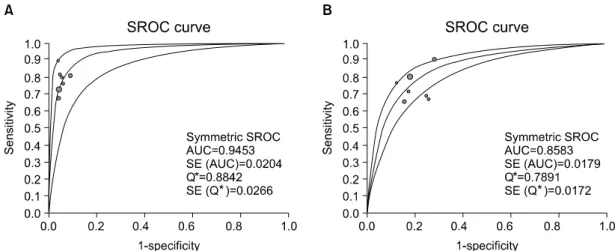
Fig. 4. SROC curves for either anti-CCP or RF (A) and both anti-CCP and RF positivity (B) for the diagnosis of RA Solid circles represent individual studies included in this meta-analysis. The curve shown is a regression line that summarizes overall diagnostic accuracy. SE (AUC), standard error of AUC, Q*, an index defined by the point on the SROC curve where the sensitivity and specificity are equal; SE (Q*), Q* index standard error.
have shown more accurate results compared to those from all 7 studies (Table 3). Sensitivity estimate of anti- CCP antibody in HC was similar to that from NRA, but specificity, PLR and DOR were higher compared to those from NRA (98.8% vs. 95.1%, 52.791 vs. 14.837, 217.14 vs. 59.235, respectively). However, RF data that were limited to studies of healthy controls were similar to those from all 7 studies.
4. Diagnostic accuracy of anti-CCP antibody or/and RF positivity
For studies that considered a result positive if either anti-CCP antibody or RF was detected (17,20,23), the sensitivity and the specificity were 85.2% (81.8∼
88.2) and 74.5% (70.3∼78.4) (Table 2). Although the specificity was decreased, the sensitivity of either anti- CCP antibody or RF was higher than that of anti-CCP antibody or RF alone (Table 2). The PLR, NLR, DOR, AUC, Q* index were not remarkable (Table 2, Fig. 4). For both anti-CCP antibody and RF positi- vity, the specificity, PLR and DOR were remarkably increased compared to those of RF alone (96.5% vs 80.5%, 22.230 vs. 3.687, 158.46 vs. 12.915, respec-
tively) (Table 2). The AUC for both anti-CCP anti- body and RF positivitity were higher than those than RF alone or either anti-CCP antiboby or RF positivity (Table 2, Fig. 4).
DISCUSSION
Meta-analysis is well known as a method to integrate previous research, providing increased stati- stical power and resolution by combining the results of independent analyses (24). Meta-analysis overcomes the problem of small sample size and inadequate statistical power. A comprehensive metaanalysis for synthesis of the accumulated data may be needed for improving precision and clarifying the inconsistent data from individual studies. A common criticism of meta- analysis is that it pools the results of different studies conceptualized in different ways using different design, different measures, and different treatment. Although this is true, meta-analytic procedures allow the coding of various methodologic and substantive differences.
More than a simple effect size can be obtained and evaluated. Therefore, meta-analysis is an effective tool
for synthesizing research findings and answering clinical questions for practice.
To our knowledge, this study is the first meta- analysis that evaluated the diagnostic accuracy of anti-CCP antibodies and RF for diagnosing RA in Koreans. This meta-analysis of 7 studies (2,011 partici- pants) on the diagnostic value of anti-CCP antibody and RF for the diagnosis of RA shows that the sensitivity of anti-CCP antibody is similar to that of RF, but that the specificity of anti-CCP antibody is higher than that of RF, and that the overall diagnostic accuracy of anti-CCP antibody is better than that of RF for diagnosing RA in the Korean population. When sensitivity and specificity were considered indepen- dently, the sensitivity of anti-CCP antibody was 76.7%
and its specificity was 95.1%, whereas respective values for RF were 78.2% and 80.5%. AUC provides an index of the overall discriminative ability of a test.
When sensitivity and specificity were considered simul- taneously, the AUC for anti-CCP antibodies was 0.9453, whereas that for RF was 0.8583. These results are consistent with those of previous relevant meta- analyses and confirm the value of anti-CCP antibody as a diagnostic marker of RA in Koreans. The PLR and DOR in HC were remarkably increased compared to those from NRA (52.791 vs. 14.837, 217.14 vs.
59.235, respectively). A PLR value of 52.791 suggests that patients with RA have an approximately 53-fold higher chance of being anti-CCP antibody positive compared with healthy controls. The DOR is a single indicator of test accuracy that combines the data from sensitivity and specificity into a single number (25). The DOR of a test is the ratio of the odds of positive test results in the patient with disease relative to the odds of positive test results in the control subjects. The value of a DOR ranges from 0 to infinity, with higher values indicating better discriminatory test performance.
A DOR of 1.0 indicates that a test does not discriminate between patients with the disorder and controls. In the present meta-analysis, we have found that the DOR was 217.14, indicating a high level of
overall accuracy. These findings suggest that anti-CCP antibody has more diagnostic accuracy in discrimi- nating RA from HC than from NRA in Koreans.
Some studies suggested that the diagnostic accuracy of both anti-CCP antibody and RF posibitivity was not markedly better than that of anti-CCP antibody positivity alone. Our result was compatible with the previous known result (10), but the combination of anti-CCP antibody and RF positivity improved both specificity and AUC over RF positivity alone. For studies of either anti-CCP antibody or RF positivity, the specificity was decreased and the sensitivity was higher than that of anti-CCP antibody or RF alone. As a result, combining anti-CCP antibody and RF testings offered a better diagnostic value than anti-CCP antibody or RF alone.
The function of RF is unclear, as it is present in other rheumatic diseases and in healthy controls. In contrast, anti-CCP antibody is detected prior to the onset of RA and its presence seems to be associated with the future development of RA, with an OR of 15.9, which is higher than those of shared epitope and RF (OR of 2.35 and 6.8, respectively) (26). Immunity against citrulline may play a crucial role in the pathogenesis of RA. Moreover, anti-CCP antibody is produced locally in inflamed joints, whereas citrulli- nated fibrin is found in the synovia of RA patients (27). A normal subject with a positive anti-CCP antibody test has a substantial risk of RA development (28). These findings suggest that the initial trigger for the development of RA may occur long before the appearance of symptoms. Thus, anti-CCP antibody monitoring in people with an increased risk of RA development might allow earlier treatment.
Anti-CCP antibody testing offers an additional serological means of diagnosing RA. The sensitivity of anti-CCP antibody is close to that of RF, and anti-CCP antibody has a higher specificity than RF for distinguishing between RA and other rheumatic diseases. The better diagnostic accuracy of anti-CCP antibody was mainly due to its higher specificity, and
thus anti-CCP represents a better serological marker than RF for the diagnosis of RA. Rheumatologists measure serum RF level because it is included in the 1987 ACR criteria (3). To prevent joint destruction, RA must be diagnosed early and treatment started as soon as possible. In clinical practice, most rheumato- logists recommend measuring both anti-CCP antibody and RF, because clinicians try to maximize sensitivity by combining markers. The present study indicates that the usefulness of adding the presence of anti-CCP antibody to the ACR classification criteria for RA requires prompt consideration.
Our analysis differed from previous meta-analysis on the diagnostic accuracy of anti-CCP antibody and RF for RA by Nishimura et al (10). They analyzed the published studies regardless of ethnicity. So they included a lot of data, 37 studies of anti-CCP antibody and 50 studies of RF. And the association of the antibodies with radiographic progression was studied in the meta-analysis. In contrast, to assess the diagnostic accuracies of anti-CCP antibody and RF for the diagnosis of RA in a Korean population, we conducted the meta-analysis with the data limited to Koreans.
Only one study included in our meta-analysis was included in the previous meta-analysis (17). The number of studies in the meta-analysis in Koreans was relatively small, but the diagnostic accuracy of anti-CCP antibody was more specific than RF in Koreans like the result from the previous meta- analysis. We could not analysis the association of the antibodies with radiographic progression in our meta- analysis due to limited data, though the previous meta-analysis showed anti-CCP antibody may better predict erosive disease. Another previous meta-analysis evaluated the two generations of anti-CCP antibodies as a diagnostic marker for RA and showed sensitivity of the second generation for anti-CCP is close to that of RF, with a higher specificity (11). However, we could not analyze the diagnostic value according to the two generations of anti-CCP antibodies due to limited data from primary studies.
The present study has limitations that should be considered. First, between-study heterogeneity was encountered in terms of RF specificity, which is probably explained by the different techniques used to measure RF and different clinical statuses. Between- study heterogeneity may have affected the results of this meta-analysis, and this is compounded by the limited information provided on clinical status and disease severity in the populations involved. We tried to overcome this limitation by using a random-effects model that incorporates uncertainties arising due to between-study variations. Second, publication bias or confounding factors may be present, distorting the meta-analysis. We could not draw a funnel plot for each meta-analysis due to the small number of studies.
Analysis of the data stratified by gender, disease activity or duration would have provided more infor- mation, but such information was not available from the studies for meta-analysis.
Nevertheless, this meta-analysis also has its strengths. In particular, ethnic differences may affect antibody accuracy for the diagnosis of RA. It is unclear whether the RF and anti-CCP tests are as sensitive to racial and ethnic differences as genetic variations, such as, the human leukocyte antigen (HLA)-DRB1 or peptidylarginine deiminase 4 (PADI4) polymorphisms (29). The present study was limited to Korean populations, and thus, potential biases associated with such differences were eliminated from this meta-analysis
We conclude that the sensitivities of anti-CCP antibody and RF are similar for diagnosing RA in the Korean population, but that anti-CCP antibody is more specific and has better diagnostic accuracy than RF.
And combining anti-CCP antibody and RF testings offers better diagnostic accuracy than anti-CCP antibody or RF alone.
REFERENCES
1) Lee DM, Weinblatt ME. Rheumatoid arthritis. Lancet
2001;358:903-11.
2) Lard LR, Visser H, Speyer I, vander HorstBruinsma IE, Zwinderman AH, Breedveld FC, et al. Early versus delayed treatment in patients with recent-onset rheumatoid arthritis: comparison of two cohorts who received different treatment strategies. Am J Med 2001;111:446-51.
3) Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheuma- tism Association 1987 revised criteria for the classifi- cation of rheumatoid arthritis. Arthritis Rheum 1988;
31:315-24.
4) Saraux A, Berthelot JM, Chales G, Le Henaff C, Thorel JB, Hoang S, et al. Ability of the American College of Rheumatology 1987 criteria to predict rheumatoid arthritis in patients with early arthritis and classification of these patients two years later. Arthri- tis Rheum 2001;44:2485-91.
5) Dorner T, Egerer K, Feist E, Burmester GR. Rheuma- toid factor revisited. Curr Opin Rheumatol 2004;16:
246-53.
6) Schellekens GA, de Jong BA, van den Hoogen FH, van de Putte LB, van Venrooij WJ. Citrulline is an essential constituent of antigenic determinants recog- nized by rheumatoid arthritis-specific autoantibodies.
J Clin Invest 1998;101:273-81.
7) van Boekel MA, Vossenaar ER, van den Hoogen FH, van Venrooij WJ. Autoantibody systems in rheuma- toid arthritis: specificity, sensitivity and diagnostic value. Arthritis Res 2002;4:87-93.
8) Vossenaar ER, Zendman AJ, van Venrooij WJ, Pruijn GJ. PAD, a growing family of citrullinating enzymes:
genes, features and involvement in disease. Bioessays 2003;25:1106-18.
9) Schellekens GA, Visser H, de Jong BA, van den Hoogen FH, Hazes JM, Breedveld FC, et al. The diagnostic properties of rheumatoid arthritis anti- bodies recognizing a cyclic citrullinated peptide.
Arthritis Rheum 2000;43:155-63.
10) Nishimura K, Sugiyama D, Kogata Y, Tsuji G, Nakazawa T, Kawano S, et al. Meta-analysis: diagno- stic accuracy of anti-cyclic citrullinated peptide anti- body and rheumatoid factor for rheumatoid arthritis.
Ann Intern Med 2007;146:797-808.
11) Avouac J, Gossec L, Dougados M. Diagnostic and predictive value of anti-cyclic citrullinated protein antibodies in rheumatoid arthritis: a systematic litera- ture review. Ann Rheum Dis 2006;65:845-51.
12) Lijmer JG, Bossuyt PM, Heisterkamp SH. Exploring
sources of heterogeneity in systematic reviews of diagnostic tests. Stat Med 2002;21:1525-37.
13) Walter SD. Properties of the summary receiver operating characteristic (SROC) curve for diagnostic test data. Stat Med 2002;21:1237-56.
14) Davey SG, Egger M. Meta-analyses of randomised controlled trials. Lancet 1997;350:1182.
15) Higgins JP, Thompson SG. Quantifying heteroge- neity in a meta-analysis. Stat Med 2002;21:1539-58.
16) Zamora J, Abraira V, Muriel A, Khan K, Coomara- samy A. Meta-DiSc: a software for metaanalysis of test accuracy data. BMC Med Res Methodol 2006;
6:31.
17) Choi SW, Lim MK, Shin DH, Park JJ, Shim SC.
Diagnostic performances of anti-cyclic citrullinated peptides antibody and antifilaggrin antibody in Korean patients with rheumatoid arthritis. J Korean Med Sci 2005;20:473-8.
18) Kim KH, Lee SW, Chung WT. Association of anti-cyclic citrullinated peptide antibodies and func- tional status in rheumatoid arthritis. J Korea Rheu- matism Ass 2006;13:46-51.
19) Kim KH, Kwon JA, Kim YK. Diagnostic performance of the anti-cyclic citrullinated peptide antibodies and rheumatoid factor isotypes in rheumatoid arthritis. J Lab Med Qual Assur 2005;27:195-202.
20) Kang HJ, Seo YI, Lee YK, Cho HC. Diagnostic usefulness of the anti-cyclic citrullinated peptide antibodies for rheumatoid arthritis. J Korea Rheu- matism Ass 2003:10;117-25.
21) Song JS, Park GB, Park AJ. Comparison of anti-mutated citrullinated vimentin with anti-cyclic citrullinated peptide and rheumatoid factors for the diagnostic value of rheumatoid arthritis. Assessment.
J Korea Rheumatism Ass 2007;14:235-41.
22) Park SH, Kim JY, Kim SK, Choe JY, Kim SK, Shin IH. Diagnostic significance of anti-CCP antibody in Korean early rheumatoid arthritis. J Korea Rheuma- tism Ass 2007;14:227-34.
23) Kim HR, Shin JW, Lee JN. Evaluation of the usefulness of anti-cyclic citrullinated peptide anti- bodies measured by an automated enzyme immu- noassay. J Lab Med Qual Assur 2005;27:183-8.
24) Egger M, Smith GD, Phillips AN. Meta-analysis:
principles and procedures. BMJ 1997;3157:1533-7.
25) Glas AS, Lijmer JG, Prins MH, Bonsel GJ, Bossuyt PM. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol 2003;56:1129-35.
26) Berglin E, Padyukov L, Sundin U, Hallmans G,
Stenlund H, Van Venrooij WJ, et al. A combination of autoantibodies to cyclic citrullinated peptide (CCP) and HLA-DRB1 locus antigens is strongly associated with future onset of rheumatoid arthritis. Arthritis Res Ther 2004;6:R303-8.
27) Masson-Bessiere C, Sebbag M, Girbal-Neuhauser E, Nogueira L, Vincent C, Senshu T, et al. The major synovial targets of the rheumatoid arthritisspecific antifilaggrin autoantibodies are deiminated forms of the alpha- and beta-chains of fibrin. J Immunol
2001;166:4177-84.
28) Nielen MM, van Schaardenburg D, Reesink HW, van de Stadt RJ, van der Horst-Bruinsma IE, de Koning MH, et al. Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis Rheum 2004;50:380-6.
29) Lee YH, Rho YH, Choi SJ, Ji JD, Song GG. PADI4 polymorphisms and rheumatoid arthritis susceptibility:
a meta-analysis. Rheumatol Int 2007;27:827-33.