Abstract : Opioid analgesics strongly act on opioid receptors without any ceiling effect*.
However, if such modality suddenly stops, it represents dependence and withdrawal symptoms.
Therefore, this drug should be tapered to quit. In the intensive care unit where patients from moderate to severe pain are hospitalized, opioid analgesics are widely used for adequate pain control and sedation.
At the Severance Hospital’ s ICU, there is opioid analgesic protocol that includes fixed dilution rate and the fixed initial dose. However, for matters related to drug discontinuation, they are entirely determined by the clinical decision. As such, there are many occasions when the reiniti- ating of the opioid analgesics is needed due to withdrawal symptoms. Therefore, this study investigated the tendency of tapering opioid analgesics used in surgical intensive care unit (SICU). This study is targeting patients who were hospitalized at the Severance Hospital’ s SICU and were treated with opioid analgesics for more than 3 days during March 1st ~ August 31st of 2011. Patients under the age of 7 were excluded. A total of 147 patients’opioid analgesic tapering trends were analyzed via medical records and clinical observation records. The frequency of opi- oid analgesics used at the Severance Hospital SICU appeared to be as follows: Fentanyl 114 cases
원내 외과계 중환자실 재원 환자의 마약성 진통제 tapering현황 분석
연세대학교 세브란스병원 약무국
Tapering of Opioid Analgesics Injected to the Patients Hospitalized in Surgical Intensive Care Unit
Kyung A Lee, Soo Hee Kim, Joo Hee Jo, Ji Hyune Ahn, Eun Sun Son, Sung Eun Kim and Hyun Ju Seok
Department of pharmacy, Yonsei University Healthcare system, 50 Yonsei-ro, Seodeamun-gu, Seoul, 120-752, Korea
회원학술보고
연구 배경 및 목적
마약성 진통제는 opioid 수용체에 작용해 강력한 효 과와 더불어 증량에 따른 지속적인 효과 상승을 나타 내는 약물로, 중등도 이상의 통증을 호소하는 환자가 많은 중환자실에서 빈번히 사용되고 있다
1,2). 본 약제 는 급격하게 사용을 중단할 경우 의존성 및 중추신경 계의 흥분, 자율신경계의 조절이상, 위장관계의 이상, 호흡부전, 비정상적인 움직임과 같은 금단증상을 나 타내며, 증상의 심각도에 따라 약물 중단 속도를 느리 게 하거나 약물의 재투여가 권고되기도 한다
1, 3-5).
따라서 금단증상의 발현을 예방하고 불필요한 추가 주입을 막기 위해서는 약물 중단 시점에 마약성 진통 제의 tapering이 이루어져야 한다.
세브란스병원 외과계 중환자실(SICU)에서는 마약 성 진통제 사용 protocol을 정립하여 약물의 희석 비 율을 일정하게 유지하고 초기 주입량을 규격화하였 다. 하지만 약물 중단과 관련된 사항은 protocol로 규격화되지 않아 전적으로 임상적 판단에 의해 이루 어지고 있으며 그로 인해 마약성 진통제가 tapering 없이 중단되어 금단증상으로 인한 약물 재 투여가 필 요한 경우도 발생하고 있다
5). 이에 본 연구에서는 (78.1%), Remifentanyl 29 cases (19.9%) and Morphine 3 cases (2.1 %). According to the result, tapering was applied in 86 cases (59.6%). The number of each drug applied to tapering was Fentanyl 68 cases (59.7%), Remifentanyl 16 cases (55.2%) and Morphine 2 cases (66.7%). The median value of medication days and the mean dose tended to be high in the tapering group. The median tapering time of each drug was as follows: Fentanyl 46 hour, Remifentanyl 29.5 hour and Morphine 114 hour.
A number of cases that occur re-administration of opioid analgesics among the non-tapering group was as follows: Fentanyl 28 cases (60.9%) and Remifentanyl 9 cases (69.2%). Morphine was not re-administrated because the patient died during Morphine was administered. Moreover, the incidence of withdrawal syndrome among the non-tapering group was as follows: Fentanyl 22 cases (47.8%), and Remifentanyl 4 cases (30.8%). Therefore, this study emphasizes the pharma- cists’role of mediating inappropriate drug discontinuation and encourages appropriate drug use through the survey.
* Ceiling effect : referring to the level at which an independent variable no longer has an effect on a dependent variable.
[Key words] ICU (Intensive Care Unit), opioid analgesics, tapering
투고일자 2012. 5. 2; 심사완료일자 2012. 8. 1; 게재확정일자 2012. 11. 9마약성 진통제의 tapering 현황 및 그에 따른 진통 제 재투약 여부와 withdrawal syndrome 발생 비 율을 분석함으로써 부적절한 약물 중단에 대한 중재 활동의 바탕으로 삼아 환자에게 보다 나은 약료서비 스를 제공하고자 한다.
연구 방법 1. 기준
1) 원내 기준
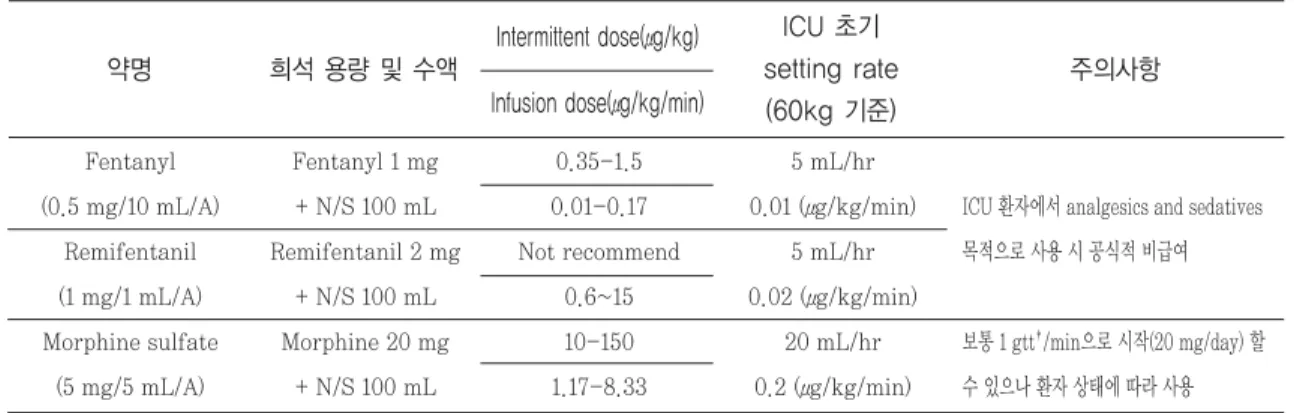
원내 마약성 진통제 사용에 관한 ICU protocol�
은 다음과 같다.(Table 1)
2) 연구 내 기준
본 연구에서 규정한 마약성 진통제의 tapering 여 부의 판단은 최종 약물 중단시점을 기준으로 하였으 며, 시간당 약물 주입량이 감소하거나 투여 간격이 늘어나는 경우를 tapering으로 판단하였다. with- drawal syndrome은 약물 중단 이후 발생한 5가지 항목(중추신경계의 흥분, 자율신경계의 조절이상, 위 장관계의 이상, 호흡부전, 비정상적인 움직임)
1)으로 정의하여 분석하였다.
2. 조사 대상
1) 대상 기준
2011년 3월 1일부터 2011년 8월 31일까지 세브란 스병원 외과계 중환자실에 입원하여 마약성 진통제 를 3일 이상 점적 투여 받은 환자
2) 제외 기준
영유아 (만 6세 미만), 해당 기간 이전에 투약을 시 작한 환자, 기간 내 투약을 완료하지 못한 환자
3. 분석 항목
1) 연구 대상 특성 2) Tapering 이행률 3) Tapering 소요 시간 4) 재원 및 투약 관련 사항
- 총 투약일수 - ICU 재원일수 - Mean dose (㎍/hr) - Peak dose (㎍/hr) - Final dose (㎍/hr) - Total dose (㎍)
Fentanyl (0.5 mg/10 mL/A)
Remifentanil (1 mg/1 mL/A) Morphine sulfate
(5 mg/5 mL/A)
Table 1. Protocols of using opioid analgesics in the Severance hospital’ s surgical intensive care unit
약명
Fentanyl 1 mg + N/S 100 mL Remifentanil 2 mg
+ N/S 100 mL Morphine 20 mg
+ N/S 100 mL
희석 용량 및 수액
0.35-1.5 0.01-0.17 Not recommend
0.6~15 10-150 1.17-8.33
Intermittent dose(μg/kg) Infusion dose(μg/kg/min)
5 mL/hr 0.01 (μg/kg/min)
5 mL/hr 0.02 (μg/kg/min)
20 mL/hr 0.2 (μg/kg/min)
ICU 초기 setting rate (60kg 기준)
ICU 환자에서 analgesics and sedatives 목적으로 사용 시 공식적 비급여
보통 1 gtt�/min으로 시작(20 mg/day) 할 수 있으나 환자 상태에 따라 사용
주의사항
� Reference: Jacobi, J., Fraser, G.L., Coursin, D.B., Riker, R.R., Fontaine, D., Wittbrodt, E.T., Chalfin, D.B., Masica, M.F., Bjerke, H.S., Coplin, W.M., Crippen, D.W., Fuchs, B.D., Kelleher, R.M., Marik, P.E., Nasraway, S.A., Murray, M.J., Peruzzi, W.T., Lumb, P.D. : Clinical Practice Guidelines for the Sustained Use of Sedatives and Analgesics in the Critically Ill Adult, Critical Care Med, 30(1), 119-41(2002)
�원내 기준 수액세트 점적 방울 수 : 20 drops (gtt) = 1 mL
5) Tapering 비적용군의 마약성 진통제 재투약 현황
6) Tapering 비적용군의 withdrawal syndrome 발생 비율
4. 조사 방법
대상 환자군의 투약내역 및 EMR(Electronic medical record) 임상관찰기록을 이용하여 각 분석 항목에 대하여 후향적으로 조사하였다.
5. 분석 방법
데이터 분석 및 통계처리는 SPSS(version 18.0) 프로그램을 이용하였으며, 연구 대상의 특성, tapering 이행률 및 소요 시간, 약물 중단 사유, 재 투약 비율, withdrawal syndrome 발생 비율은 백 분율로 분석하였다. Mean dose, peak dose, final dose, total dose 및 투약일수, ICU 재원일수는 Mann Whitney U test를 이용하여 분석하였다.
연구 결과
1. 연구 대상 특성
2011년 3월 1일부터 8월 31일까지 본원 외과계 중환자실에서 마약성 진통제를 점적 투여받은 환자 는 총 146명으로 남자 102명(69.9%), 여자 44명 (30.1%)으로 나타났다. 대상 환자군의 평균 나이는 57.5세(±SD 16.6) 였으며 점적 투여된 마약성 진 통제는 빈도 별로 Fentanyl 114건(78.1%), Remifentanyl 29건(19.9%), Morphine 3건 (2.1%) 순이었다.
2. Tapering 이행률
연구 결과 총 146건 중 86건(59.6%)에서 taper- ing이 이루어졌으며, 각 약물별 tapering 비율은 Fentanyl 114건 중 68건(59.7%), Remifentanyl
29건 중 16건(55.2%), Morphine 3건 중 2건 (66.7%)으로 나타났다(Fig. 1).
3. Tapering 소요 시간
Tapering 이행군의 각 약물별 약물 중단까지 tapering 소요 시간을 1일 미만, 3일 미만, 5일 미 만, 5일 이상의 4가지로 분류한 결과 Fentanyl 28 건(41.2%), Remifentanyl 9건(56.3%), Morphine 1건(50%)이 1일 이상 3일 미만의 기간 동안 taper- ing이 이루어져 가장 많은 비율을 차지하고 있었으 며, 각각의 median tapering 소요 시간은 Fentanyl 46시간, Remifentanyl 29.5시간, Morphine 114시간이었다(Fig. 2).
Fig. 2 Tapering duration
Fig. 1 Ratio of tapering
4. 재원 및 투약 관련 사항
1) 총 투약 일수 및 ICU 재원일수
Tapering 이행 여부에 따른 각 약물의 총 투약일수 및 ICU 재원일수를 비교한 결과 Fentanyl과 Morphine은 tapering 적용군에서 투약일수 및 ICU 재원일수의 median 값이 더 큰 경향을 나타낸 반면 Remifentanyl은 tapering 비적용군에서 투약일수 및 ICU 재원일수가 더 긴 경향을 보여 오랜 기간 투 약 및 재원하였음에도 불구하고 tapering이 잘 이루 어지지 않았던 것을 확인할 수 있었다(Fig. 3, 4).
2) Mean dose 및 peak dose
Tapering 이행 여부에 따른 각 약물의 mean dose에 대해 분석한 결과 모든 약물군에서 taper- ing 적용군의 mean dose가 높은 경향을 나타냈다.
하지만 peak dose의 경우 tapering 여부에 따른 두 군간 차이는 없었다(Fig. 5, 6).
3) Tot al dose
Tapering 이행 여부에 따른 각 약물의 total dose 에 대해 분석한 결과 Fentanyl의 경우 tapering 적 용군의 총 투여 용량이 높은 경향을 보였던 반면 Remifentanyl, Morphine의 경우 tapering 비적
Fig. 4 Length of ICU stay Fig. 6 Peak dose (㎍ /hr)
Fig. 3 Days of medication Fig. 5 Mean dose (㎍ /hr)
용군의 총 투여 용량이 높은 경향을 보여 고용량 투 여에도 불구하고 tapering이 이루어지지 않았던 것 을 확인할 수 있었다(Table 2).
4) Final dose
Tapering 여부에 따른 각 약물의 중단 직전 투여 용량에 대해 분석한 결과 Remifentanyl의 경우 final dose의 차 이 가 없 었 으 나 Fentanyl, Morphine의 경우 tapering 비적용군의 final dose 가 높은 경향을 나타내 tapering 적용군 대비 고용 량에서 약물 중단이 이루어진 것으로 나타났다.
5. Tapering 비적용군의 마약성 진통제 재투약 현황
1) Fentanyl
Fentanyl의 tapering 비적용군 46명을 대상으로 분석한 결과 Fentanyl의 재투약이 이루어진 환자는 12명(26.1%), 타 마약성 진통제의 투약이 이루어진 환자는 16명(34.8%)으로 총 28명(60.9%)에서 마약 성 진통제의 재투약이 이루어졌다. 비마약성 진통제 로 전환된 환자는 9명(19.6%) 이었으며 진통제의 투 약이 이루어지지 않은 환자는 4명(8.7%), 사망한 환 자는 5명(10.9%)였다 (Fig. 7, 8).
2) Remifentanyl
Remifentanyl의 tapering 비적용군 13명을 대상 으로 분석한 결과 Remifentanyl의 재투약이 이루 어진 환자는 3명(23.1%), 타 마약성 진통제의 투약 이 이루어진 환자는 6명(46.2%)으로 총 9명(69.2%)
투약일수 (일)
ICU 재원일수 (일)
Mean dose (㎍/hr)
Peak dose (㎍/hr)
Final dose (㎍/hr)
Total dose (㎍)
Table 2. Analysis of the above factors
Fentanyl Remifentanyl
Morphine Fentanyl Remifentanyl
Morphine Fentanyl Remifentanyl
Morphine Fentanyl Remifentanyl
Morphine Fentanyl Remifentanyl
Morphine Fentanyl Remifentanyl
Morphine
약물
5.5 4 16.5
11 10 38 62.2 133.3 515.1 100 200 1200 40 100 140 6227 8245.3 86590.6
Tapering 적용군
4.5 5 11 8 18 30 56.5 107.6 445.7 100 200 1200
60 100 600 4445 8600 102960
Tapering 비적용군
0.035 0.374 1 0.504 0.045 1 0.712 0.357 1 0.073 0.812 1
<0.01 0.17 0.221 0.054 0.846 0.221