VOL. 13, NO. 2, 2014
CLINICAL PAIN 103 접수일 : 2014 년 10 월 4 일 , 게재승인일 : 2014 년 12 월 7 일
책임저자 : 이상헌 , 서울시 성북구 안암동 5 가
136-705, 고려대학교 안암병원 재활의학과
Tel: 02-920-6471, Fax: 02-929-9951 E-mail: [email protected]
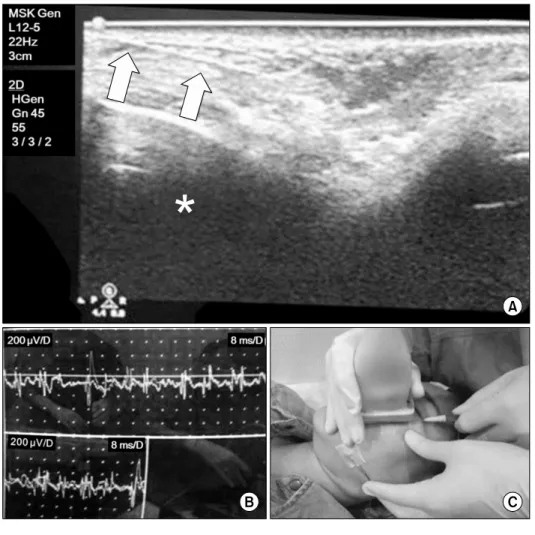
안면신경마비 후 안면연축에 대한 새로운 치료적 접근: 초음파와 근전도 검사의 동시 사용 방법
증례 보고
고려대학교 안암병원 재활의학과
한아름ㆍ김승민ㆍ이상헌