Journal of Minimally Invasive Surgery
□
Case Report
□Vol. 15. No. 1, 2012
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
후복막에서 발생한 기관지원성 낭종의 복강경 절제
을지대학교 의과대학 노원을지병원 외과, 소화기내과1, 병리과2
김광순ㆍ조윤주1ㆍ홍영옥2ㆍ이병석ㆍ김동희
Laparoscopic Resection of a Bronchogenic Cyst Presenting as a Retroperitoneal Tumor
Kwang Soon Kim, M.D., Yun Ju Jo, M.D.
1, Yong Ok Hong, M.D.2,Byung Seok Lee, M.D., Dong Hee Kim, M.D.
Departments of Surgery,
1Gastroenterology and
2Pathology, Eulji General Hospital, Eulji University School of Medicine, Seoul, Korea
A bronchogenic cyst is regarded as a developmental abnor- mality of the primitive foregut, which typically occurs in the mediastinum. The cystis normally diagnosed in relation to res- piratory problems or recurrent infections in children. In adult- hood, it is a rare pathology, and its diagnosis is usually incidental. Moreover, subdiaphragmatic and retroperitoneal lo- cations are exceptionally rare. A 60-year old woman presented with an incidental left retroperitoneal mass that was suspected of being a non-functioning retroperitoneal tumor. After evalu- ating the general radiologic and endocrinologic work up for
a retroperitoneal tumor, a laparoscopically complete resection was performed with primary repair of the attached diaphragm.
The surgically resected cyst measured 7×5×5 cm and was filled with mucin material. Histologically, the cyst wall was lined by a ciliated pseudostratified or tall columnar epithelium with- out dysplastic changes. The diagnosis of a bronchogenic cyst in the retroperitoneum was confirmed. We present this case with a review of the relevant literature.
Key words: Bronchogenic cyst, Retroperitoneum, Laparoscopy
Received October 10, 2011, Revised 1st, March 3, 2012; 2nd, March 8, 2012, Accepted March 9, 2012
※ Corresponding author:Dong Hee Kim
Department of Surgery, Eulji General Hospital, Eulji University School of Medicine, 14, Hangeulbiseok-gil, Nowon-gu, Seoul 139-872, Korea
Tel:+82-2-970-8243, Fax:+82-2-970-1577 E-mail:[email protected]
서 론
전장 기원의 낭종은 기관지성, 식도성, 위장성, 심막성으 로 나뉘어 진다. 이중 기관지원성 낭종은 상피 기원의 전장 발달 이상으로 생겨나는 것으로 알려져 있으며, 점액을 분 비하는 섬모성 상피와 연골로 구성 되어 있다.
1대부분 소아 기에 반복성 호흡기 감염으로 진단이 되지만, 성인의 경우 에는 단층 촬영을 통해서 우연히 발견되는 경우가 대부분 이다.
2가장 많이 발견되는 장소는 종격동이고 이외에도 목, 피부, 위장, 식도, 횡격막에 생기는 것으로 알려져 있으나, 후복막강에 생기는 것은 매우 드문 것으로 보고되고 있 다.
3-5이에 저자들은 좌측 부신 주변에서 발생한 거대 기관 지원성 낭종에 대하여 성공적으로 복강경 절제를 시행하였 기에 문헌 고찰과 함께 보고하고자 한다.
증 례
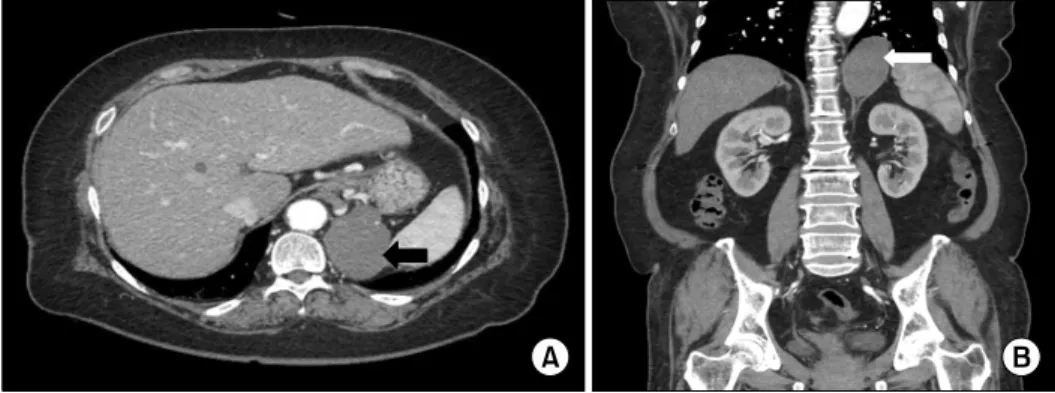
65세 여자환자로 내원 3일전부터 발생한 상복부 동통과 설사양상의 흑색변이 지속 되어 본원 응급실 통해 소화기 내과에 입원하였다. 과거력상 당뇨와 고혈압으로 약물 복 용 중 이었으며, 과거 개복하 자궁적출술을 시행 받은 경력 이 있는 환자였다. 내원시 시행한 상부 위내시경 검사상 십 이지장 궤양 소견이 보여 약물 치료를 시작하였으며, 정밀 검사를 위하여 복부 단층 촬영을 시행하였다. 영상 소견상 정상적인 부신을 확인할 수 있었으며, 부신의 상방 좌내측 방향으로 횡격막하 직경 8 cm 정도의 석회화 및 주변에 조 영 증강이 동반되는 낭종성 종괴가 관찰되었다(Fig. 1A, B).
수술 전 시행한 전해질 검사는 정상소견을 보였으며 내분
비 검사에서 혈중 cortisol은 오전 7시에 15.72 mg/dl, 오후
8시에 21.87 mg/dl (정상 범위 6∼18)로 약간 상승하였으나
24시간 소변검사상 cortisol 21.4 μg/day (정상 범위 ∼150)
로 정상 범위 내였다. 그 외에 24시간 소변에서 VMA 2.4
mg/day (정상 범위 1.5∼7.5), Metanephrine 0.5 mg/day (정상
범위 0∼1.2), Epinephrine 5.5 μg/day (정상 범위 5∼20),
Norepinephrine 64.1 μg/day (정상 범위 15∼80)로 정상 범위
내의 수치를 보였다. 이상의 내분비 기능 검사 및 영상 소견
을 종합한 결과 비기능성의 후복막 낭성 종양으로 비록 증
상이 없다 할지라도 거대한 크기로 감염, 출혈 및 암성화
Kwang Soon Kim et al.: Laparoscopic Resection of a Bronchogenic Cyst Presenting as a Retroperitoneal Tumor 17
Fig. 1. Abdominal computed tomo-
graphy scan. (A) Axial CT finding. There is a 8 cm sized cystic mass with calcifications and peripheral enhancement in the left retroperitoneal space (black arrow). (B) 3D MD CT finding. The tumor is abutted to the diaphragm (white arrow).Fig. 2. Gross pathologic appearance of the tumor. The tumor is
a 7×5×5 cm sized oval shaped and severe attached to a part of diaphragm. The mass is composed of multilocated cyst containing grayish brown mucin materials.Fig. 3. Microscopic finding. The cyst wall is composed of
pseudostratified, ciliated columnar epithelium, resting on fibrous connective tissues, fulfilling the histologic criteria of a bronchogenic cyst.과정에 대한 위험성을 배제할 수 없으므로 복강경을 이용 한 종양 절제술을 계획하여 외과로 전과되었다. 수술은 전 신마취하에 환자를 우측면 와위로 위치한 후 경복강 부신 절제술과 같은 방법으로 좌측 늑골하연을 따라 4개의 10 mm 투관침을 삽입한 후 환자의 우측에서 비장 및 췌장을 복막 연으로 부터 박리를 하였다. 종양은 좌측 부신보다 내상방 에 위치하였으며 분엽성 낭성 종양으로 내용물은 점액을 포함하고 있었고 부신과는 쉽게 박리가 가능하였다. 그러 나 종양의 측벽 및 횡격막과의 심한 유착으로 인접한 횡격 막을 동반 절제하였다. 횡격막 결손부위는 5×5 cm 정도로 prolene 2.0을 사용하여 단순봉합을 시행하였고 흉관 삽입 은 하지 않았다. 수술 중 부분 환기 등의 조치 없이 봉합이 가능하였으며 수술 후 기흉 등의 소견은 없었다. 수술 시간 은 약 200분 가량 소요되었으며 출혈량은 100 cc 미만이었 고, 수술 중 수혈은 하지 않았다. 육안적 병리 소견상절제된 낭종은 약 7×5×5 cm 크기의 경계가 좋은 종괴이나, 횡격막 과의 인접면은 박리가 불가능할 정도로 유착이 되어 있었 고 전체 무게는 약 40 gm 정도였다. 종양의 절단면은 회색 빛의 갈색 끈적끈적한 점액질로 가득 찬 다발성 분엽을 형 성한 낭종으로 구성하고 있었다(Fig. 2). 현미경 소견상 호 흡기 양상의 가성 중층 섬모양 원주 상피가 점액성 분비선 을 포함하고 있는 결체 조직에 지지되고 있는 기관지원성 낭종에 합당한 소견을 보여주고 있었다. 또한 이들 상피세 포는 비정형화를 보이지는 않았으며 그밖에 호흡기 실질 조직이나 기형종 양상은 보이지 않았다(Fig. 3). 수술 후 환 자는 특이 합병증 없이 7일째에 퇴원을 하였다.
고 찰
기관지원성 낭종은 발생학적으로 임신 3주에서 7주사이
에 발달하는 원시적인 전장(primitive foregut)에서 형성된 기
관과 기관지로 생성되는 싹(tracheobronchial tree)의 비이상
적인 발달 장애로서, 원시적인 전장과의 연결이 지속될 경
우 낭종은 식도나 기관지와의 연결이 유지된 상태로 존재
하나, 완전한 분리가 이루어지면 단순 낭종의 형태로 체내
에 여러 곳으로 이동하여 발생하는 것으로 알려져 있다.
618
Journal of Minimally Invasive Surgery Vol. 15. No. 1, 2012
특히 후복막에서 발생하는 기관지원성 낭종에 대하여 Sumiyoshi 등
7은 임신 3주에서 7주사이에 심막-복막관 (pericardioperitoneal channel)의 폐쇄가 이루어지지 않아 기 관과 기관지로 생성되는 싹(tracheobronchial tree)이 횡격막 하방으로 이동하여 후복막 낭종을 형성하는 것으로 보고하 였다.
후복막에서 발생한 기관지원성 낭종의 발생 빈도는 남녀 간 차이가 없으며, 다양한 연령대에서 발견이 된 것으로 증 례 보고를 하고 있다.
7특히 3세의 유아에서 발견된 경우가 있으며, 이는 출생 전 산전 초음파를 통하여 진단된 경우였 다.
8대부분의 경우 좌측 부신과 췌장 상방에 위치하고 있 다. 크기는 5 cm 미만으로 우연히 발견된 경우가 대부분이 며, 7 cm 이상이면 상복부 통증을 호소한 경우가 흔하였으 며, 10 cm 이상의 경우도 보고 하고 있다.
9본 증례의 경우 도 60대 여성에서 좌측 후복막에서 발생한 경우이며, 7 cm 이상으로 십이지장 궤양이 있었으나 모호한 상복부 불편감 을 호소한 경우로 문헌 보고상 일치한 소견을 보였다.
진단은 대부분의 경우 후복막 종양으로 표현하게 되며 전형적인 후복막에서 발생하는 낭성 종양인 림프종, 점액 성 낭종, 상피양 낭종, 가성 점액종, 기형종과의 감별 진단 이 필요하다.
10,11영상 진단으로 복부 단층 촬영이 가장 효 과적인 방법으로 단발성의 낭종으로 주변과 경계가 잘 이 루어진 모양을 띠며, 때때로 석회화 모양이 관찰되는 것으 로 알려져 있다.
12그러나 이러한 소견은 상기한 후복막 낭 종의 예에서도 관찰되므로 오직 조직 병리학적 진단만이 기관지원성 낭종의 확진이 가능하다.
후복막에서 발생한 기관지원성 낭종의 치료 원칙은 수술 적 절제이다. 대부분의 경우 무증상의 우연히 발견된 경우 이나, 낭종이 충분히 커서 증상을 유발할 수 있으며 감염, 출혈 등의 합병증 및 악성변화의 가능성을 배제 할 수 없기 때문이다.
13Coselli 등
6은 감염은 기관지원성 낭종의 가장 잘 알려진 합병증으로, 감염된 기관지원성 낭종을 절제할 경우 수술 후 합병증 발생율 및 사망률을 높인다고 하였으며 더 욱이 양성의 기관지원성 낭종에서 상피암이나 섬유육종이 발생한다고 보고하였다. 본 증례에서와 같이 복강경 수술 중 횡격막 손상은 대부분의 경우 부신절제술등의 횡격막과 인접한 후복막 장기의 수술에서 발생할 수 있으나, 수술 중 안전하게 체내에서 복강경 단순 봉합이 가능하며, 수술 후 이산화탄소 기흉의 발생 위험은 매우 드물며 흉관 삽입등의 처치가 필요없는 것으로 보고하고 있다.
14일단 수술이 결정된다면 복강경 수술의 경험이 풍부한 외 과의 경우 복강경 접근이 개복이나 후복막 접근보다 안전하 고 효과적인 방법으로 알려져 있으며, 여러 증례에서 성공 적으로 복강경 절제를 보고하고 있다.
15,16본 증례의 경우도 종양과 인접한 횡격막의 심한 유착으로 횡격막 절제를 동반 하였으나 성공적으로 복강경적 절제 및 횡격막의 봉합 수술 이 가능하였기에 문헌 고찰과 함께 보고하는 바이다.
참고문헌
1) Liang MK, Yee HT, Song JW, Marks JL. Subdiaphragmatic bronchogenic cysts: A comprehensive review of the literature.
Am Surg 2005;71:1034-1041.
2) Daz Nieto R, Naranjo Torres A, Gmez Alvarez M, Ruiz Rabelo JF, Pérez Manrique MC, Ciria Bru R, et al. Intraabdominal bronchogenic cyst. J Gastrointest Surg 2010;14:756-758.
3) Orellana F, Cárdenas R, Manrquez ME, Ros H, Suárez L, Videla D. Retroperitoneal bronchogenic cyst: Report of one case. Rev Med Chil 2007;135:924-931.
4) Itoh H, Shitamura T, Kataoka H, Ide H, Akiyama Y, Hamasuna R, et al. Retroperitoneal bronchogenic cyst: Report of a case and literature review. Pathol Int 1999;49:152-155.
5) Manz M, Schmeer T, Horcic M, Meier R, Maurer CA.
Bronchogenic cyst: A rare cause of a retroperitoneal mass.
Zentralbl Chir 2009;134:570-572.
6) Coselli MP, de Ipolyi P, Bloss RS, Diaz RF, Fitzgerald JB.
Bronchogenic cysts above and below the diaphragm: Report of eight cases. Ann Thorac Surg 1987;44:491-494.
7) Sumiyoshi K, Shimizu S, Enjoji M, Iwashita A, Kawakami K. Bronchogenic cyst in the abdomen. Virchows Arch A Pathol Anat Histopathol 1985;408:93-98.
8) Bagolan P, Bilancioni E, Nahom A, Trucchi A, Inserra A, Neri M, et al. Prenatal diagnosis of a bronchogenic cyst in an unusual site. Ultrasound Obstet Gynecol 2000;15:66-68.
9) Dogget RS, Carty SE, Clarke MR. Retroperitoneal bronchogenic cyst masquerading clinically and radiologically as a phaeochro- mocytoma. Virchows Arch 1997;431:73-76.
10) Inaba K, Sakurai Y, Umeki Y, Kanaya S, Komori Y, Uyama I. Laparoscopic excision of subdiaphragmatic bronchogenic cyst occurring in the retroperitoneum: report of a case. Surg Laparosc Endosc Percutan Tech 2010;20:199-203.
11) Chu PY, Hwang TI, Teng TH, Lee CC. A retroperitoneal bronchogenic cyst successfully treated by laparoscopic surgery.
Ann Saudi Med 2007;27:199-200.
12) Murakami R, Machida M, Kobayashi Y, Ogura J, Ichikawa T, Kumazaki T. Retroperitoneal bronchogenic cyst: CT and MR imaging. Abdom Imaging 2000;25:444-447.
13) Sullivan SM, Okada S, Kudo M, Ebihara Y. A retroperitoneal bronchogenic cyst with malignant change. Pathol Int 1999;49:
338-341.
14) Castillo OA, Vitagliano G, Moreno M, Diaz MA, Cortes O.
Management of diaphragmatic injury during transperitoneal laparoscopic urological procedures. Int Braz J Urol 2007;33:
323-328.
15) Chung JM, Jung MJ, Lee W, Choi S. Retroperitoneal bronchogenic cyst presenting as adrenal tumor in adult success- fully treated with retroperitoneal laparoscopic surgery. Urology 2009;442:13-15.
16) Ishizuka O, Misawa K, Nakazawa M, Nishizawa OA. Retro- peritoneal bronchogenic cyst: Laparoscopic treatment. Urol Int 2004;72:269-270.