Vol. 47, No. 5, pp. 646 - 656, 2006
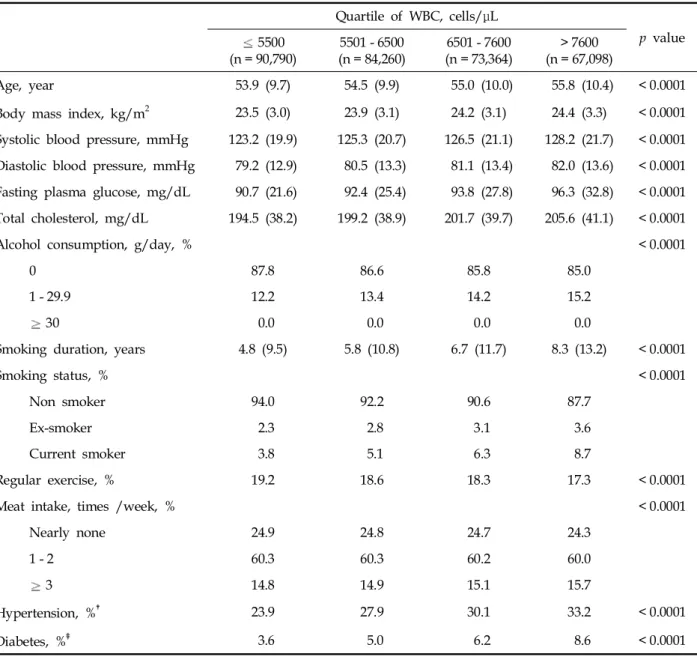
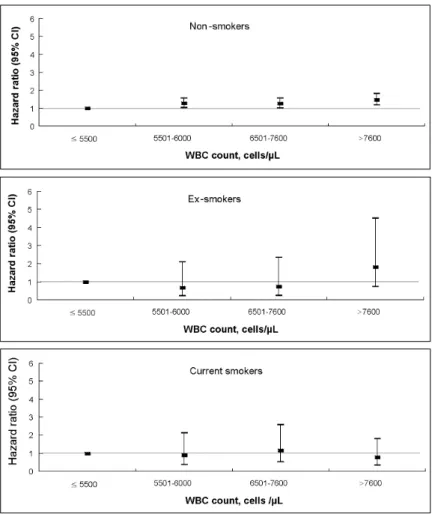
Inflammation may be linked to the pathogenesis of colorec- tal cancer. However, two conflicting observational results were recently reported on the relationship between the inflammatory marker C-reactive protein (CRP) and the risk of colorectal cancer. Few epidemiologic studies have examined the associa- tion between inflammatory markers and the risk of colorectal cancer. We prospectively examined the mortality and incidence risk for colon and rectal cancers among 424,419 Koreans (108,907 men and 315,512 women). The subjects were 40 to 95 years of age and from the Korean Cancer Prevention Study (KCPS) cohort. All subjects received medical examination from the National Health Insurance Corporation in 1993 and 1995. The maximum follow-up period was 10 years, and the follow-up periods began in January 1, 1994 and ended in December 31, 2003. An elevated white blood cell count (WBC) was associated with a higher mortality risk of colon cancer (highest versus lowest quartile: men, 1.55, 95% CI 1.10-2.18, p for trend = 0.0014; women, 1.51, 95% CI 1.12- 2.03, p for trend = 0.0049). Similarly, an elevated WBC was associated with a higher incidence risk of colon cancer (highest versus lowest quartile: men, 1.38, 1.09-1.76, p for trend = 0.0017; women, 1.46, 95% CI 1.20-1.78, p for trend=
0.0003). A positive linear trend was also observed in non- smokers. There was no significant association between WBC and the risk of rectal cancer. Our findings demonstrate that an elevated WBC is associated with an increase in both the mor- tality and incidence rates of colon cancer. These results support our hypothesis that inflammation increases the risk of colon cancer.
Key Words: White blood cell count, inflammation, colon cancer
INTRODUCTION
The proportion of colorectal cancer has been gradually increasing during the past several dec- ades in Korea. In 1980, when the Central Cancer Registry began, colorectal cancers accounted for 5.8% of total cancers.
1In 1990 and 2002, this figure increased to 6.9% and 11.2%, respectively. With estimates of 11,000 new cases annually, colorectal cancer is the fourth most common cancer and the fourth leading cause of cancer-related deaths in Korea.
1,2In 1983, the death rate of colorectal can- cers accounted for 1.6 per 100,000 person-years, and rapidly increased to 10.6 per 100,000 person- years in 2002.
2Considerable studies have examined factors that influence the development of colorectal cancer.
Family histories of colorectal cancer,
3obesity,
4animal fat intake,
5alcohol,
6cigarette smoking,
7physical inactivity,
8and insulin resistance
9have been regarded as predisposing factors of colo- rectal cancer.
Increasing evidence suggests that inflammation may be linked to the pathogenesis of colorectal cancer. Many studies have suggested a relation- ship between colorectal cancer and chronic in- flammation. The risk of colorectal cancer increases in patients with long-standing inflammatory bowel diseases.
10In addition, several studies have con- sistently shown a risk reduction for the incidence of colorectal adenoma and cancer among regular and prolonged users of aspirin or other non- steroidal anti-inflammatory drugs (NSAIDs).
11,12However, two conflicting observational results were recently reported on the relationship between the inflammatory marker C-reactive protein (CRP)
White Blood Cell Count and the Risk of Colon Cancer
Yong-Jae Lee,
1Hye-Ree Lee,
1Chung-Mo Nam,
2Ue-Kyoung Hwang,
3and Sun-Ha Jee
41
Department of Family Medicine, Yong-dong Severance Hospital, Yonsei University College of Medicine, Seoul, Korea;
2
Department of Preventive Medicine, Yonsei University College of Medicine, Seoul, Korea;
3
Department of Family Medicine, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea;
4