Corresponding author: Sunhee Cho, Department of Nursing, Mokpo National University, 61 Dorim-ri Cheonggye-myeon, Muan 534-729, Korea
Tel: +82-61-450-2676, E-mail: [email protected] Received August 15, 2012, Revised August 15, 2012 Accepted September 10, 2012
Influencing Factors of Psychosomatic and Psychological Symptoms of Stress in Korean Adults
*The Research Institute of Nursing Science, College of Nursing, Seoul National University, Seoul,
†
Department of Nursing, Mokpo National University, Muan, Korea,
‡
Department of Human Services, New York City College of Technology, City University of New York, NY, USA
Yang-Sook Hah*, Sunhee Cho
†, Myungae Choe*, Keum-Soon Kim*, Myungsun Yi*, Soyeon Cho
‡The purpose of this study was to examine predictors of somatic symptoms and psychological symptoms of stress among Korean adults. A cross-sectional descriptive survey was conducted. A sample size of 815 male and 1,554 female adults residing in South Korea completed the instruments of perceived stress, symptoms of stress, and way of coping. Data was analyzed by multivariate regression. Influencing factors for eleven symptoms of stress were as follows: a) subjective health status, having disease, perceived stress level were significant influencing factors for all symptoms of stress; b) problem-focused coping was a significant influencing factor for psychological symptoms of stress; c) emotional-focused coping was significant influencing factor for both psychosomatic and psychological symptoms of stress; d) age, gender, subjective health status, having disease, and perceived stress level were significant influencing factors for psychosomatic symptoms of stress; e) emotion-focused coping predicted psychosomatic symptoms of stress. Feeling healthier and perceiving a lower stress level predicted more psychological symptoms of stress. In contrast, using more emotion-focused coping was significantly associated with more psychosomatic symptoms of stress. The findings suggest that community health providers need to develop interventions to aware coping strategies and to enforce problem-focused coping skills for community-dwelling Korean adults with psychosomatic complaints. (Korean J Str Res 2012;20:179∼186)
Key Words: Coping skills, Emotional stress, Life stress, Physiological stress
INTRODUCTION
Stressful life events are known to have a negative influence on physical and mental health. Mental disorders such as depression and anxiety disorder, for example, may be triggered by stressful
life events (Brown, 1998). Among physical and psychological symptoms reported during outpatient encounters, the somatic account for more than half and at least one third of these somatic symptoms are medically unexplained (Hartz et al., 2000). Further, the majority (70∼90%) of patients with psychological symptoms complain of somatic symptoms, with again at least one third them left unexplained, (Simon et al., 1999). Such results suggest the need to examine potential predicting factors for somatic symptoms of stress.
Traditionally in explaining the stress process, coping is considered
as one of the major mediator/moderators (Folkman et al., 1986).
Coping is defined as the person’s cognitive and behavioral efforts to manage specific demands that are appraised as exceeding the person’s resources (Lazarus et al., 1984). Adaptations to stress life events depend heavily on coping strategies evoked in response to the impending stress. This is because coping is capable of mediating the emotional outcome, that is, it can change the emotional state (Lazarus, 1993). Coping has two widely recognized forms: emotion-focused coping and problem-focused coping (Folkman et al., 1986). In previous studies, avoidance coping was found to play a mediating role in the relationship between stressful life events and negative affect (Lee K et al., 2009), and emotional coping and avoidance coping were significantly related to symptoms of stress (Hah YS et al., 2010).
The recent Korean research on stress addresses the relation between symptoms of stress and ways of coping (Han KS et al., 2000; Han KS, 2002; Seo JY et al., 2006; Kim HJ et al., 2007;
Hah YS et al., 2010). That is, ways of coping are related to somatic symptoms (Seo JY et al., 2006), and the coping pattern is a predictor of symptoms of stress (Han KS et al., 2000; Han KS, 2002; Hah YS et al., 2010). In spite of relatively consistent results among those studies, there is limited empirical evidence to clarify whether specific coping patterns influence differently on specific types of stress symptoms, especially psychosomatic symptoms and psychological symptoms. For instance, only a few Korean studies have examined specific coping patterns influencing on specific symptoms of stress because previous studies did not present specific symptoms of stress (e.g., Han KS et al., 2000;
Han KS, 2002; Hah YS et al., 2010), or used multivariate regression (Seo JY et al., 2006; Kim HJ et al., 2007). Moreover, the subjects of most previous studies were limited in certain age groups of community population (Seo JY et al., 2006; Hah YS et al., 2010) or in certain illness groups (Han KS et al., 2000;
Han KS, 2002). The bottom line is that nationally representative research on symptoms of stress and coping is very scarce in South Korea.
Stress is a common experience in our daily lives causing or exacerbating many diseases such as heart disease, asthma, GI disturbances, the common cold, and perceived health status also affect perceived stress (Park HS et al., 2007; Yoon SH et al., 2006). Moreover, stress can influence health behaviors such as drinking and smoking (Yoon SH et al., 2006), yet we have very
little idea of those factors may influence symptoms of stress.
The present study was conducted to examine the factors influencing the expressions of psychosomatic and psychological symptoms that are often associated with stress exposure, among community-dwelling adults in South Korea. To explore the influencing factors, socio-demographic characteristics, health behaviors such as drinking and exercise, perceived stress, and ways of coping were included in each steps of regression analysis.
The purpose of this study was to examine predictors of psychosomatic symptoms and psychological symptoms of stress among community-dwelling Korean adults.
MATERIALS AND METHODS
1. Sampling and data collection
A cross-sectional, descriptive survey study design was used. The subjects were 815 male (34.4%) and 1,554 (65.5%) female adults from Seoul and 6 other metropolitan cities and from 9 provinces.
They were recruited utilizing quota sampling based on the cities and provinces population ratio. Structured questionnaires were returned by subjects between May 1 and June 30, 2007. Out of the 2,515 returned questionnaires (return rate=93.3%), 2,372 (94.3%) effective ones were analyzed. This sample size was sufficient to analysis, given that the minimal sample size was estimated to be 103 subjects based on the power analysis by Cohen(1988) for regression models the significance level set at .05, power (1-β) at .80, R
2of .15 and the seven independent variables. Considering ethical issues of the research, the researchers explained the subjects’ autonomy to participate to and drop out of the research, the purpose of the research, the subjects’
anonymity and confidentially before getting consent following approval of a University’s Institute of Review Board (Protocol No. 2007-10).
2. Measurement
The Korean version of the Brief Encounter Psychosocial Instrument
(BEPSI-K) was used to measure perceived stress. BEPSI was originally
developed by Frank et al.(1988) based on a stress-model. BEPSI-K
was translated by Bae JM et al.(1992) and modified by Yim JH et
al.(1996). BEPSI-K was a 5-item short form with responses
scored from 1 (none) to 5 (always) points. Higher scores indicate
higher level of stress. The internal consistency was .80 in Yim JH et al.(1996)’s study. The internal consistency in this study was .83.
A Symptoms of Stress (SOS) Inventory was used to measure the physical and mental health symptoms often associated with stress exposure. The SOS was originally developed by Leckie et al.(1979), and translated into Korean by Lee SW(1992). The SOS is a 94-item scale with items scored from 1 (none) to 5 (very frequently) points. The 11 subscales included in this scale are:
peripheral manifestations, cardiopulmonary symptom, upper airway symptom, central- neurological symptom, gastrointestinal symptom, muscle tension, habitual patterns, depression, anxiety, emotional irritability, and cognitive disorganization. Mean scores of total and sub-scales were computed. Higher scores indicate more frequently experienced symptoms. Lee SW(1992) reported internal consistency of the total SOS was .97, with subscale consistency ranging from .74 to .90. In this study, the internal consistency of the total SOS was very similar to original reports: .93 for the total score and .77 to .90 for the subscales.
The Ways of Coping (WOC) Checklist originally developed by Lazarus et al.(1984) and translated into Korean and modified by Kim JH(1987) was used to identify the stress coping types. The WOC is a 62-item scale with items scored from 1 (do not use) to 4 (use very frequently) points. The 4 subscales included in this checklist are: active problem solving, social support seeking, emotional relieving, and wishful thinking. Active problem solving and social support seeking are classified in problem- focused coping and emotional relieving and wishful thinking are classified in emotion-focused coping. The mean of subscale scores stands for each stress coping type. Higher scores of certain subscale indicate that the coping type is used more often. Kim JH(1987) reported internal consistency of the subscales was ranged from .87 to .95.
In present study, the internal consistency of the total items was .88 and those of subscales ranged from .75 to .88.
Perceived health status, amount of drinking and smoking were measured by asking “How is your health in general?”, “How often do you drink?”, and “How often do you smoke cigarettes?”.
3. Data analysis
Data analyses were conducted in two steps using SPSS 19.0.
First, descriptive statistics were examined for demographic
variables, health behavior variables (exercise, smoking, and drinking), subjective health and disease variables, and coping style variables. Next, to analyze predictors of each set of health symptoms (RP=peripheral manifestations, RC=cardiopulmonary symptoms, RU=upper airway symptoms, RN=central neurological symptoms, RD=gastrointestinal symptoms, RT=muscle tension, RB=habitual patterns, RDE=depression, RA=anxiety, ANG=anger, COG=cognitive disorganization), multivariate regression analysis was used. Demographic variables, health variables, subjective health and disease, and coping style variables were entered, in successive steps. The 11 symptoms of stress, then, were combined into two computed variables based on the characteristics of the symptom.
One computed variable was a somatic variable which combined physical-related symptoms of stress. Another computed variable combined psychological-related symptoms of stress. Our main focus was to examine coping style and its relation to symptoms of stress. Therefore, coping style variables were entered after controlling for the effects of other variables such as demographic variables, health behaviors, and subjective health and disease.
RESULTS
1. Sample characteristics
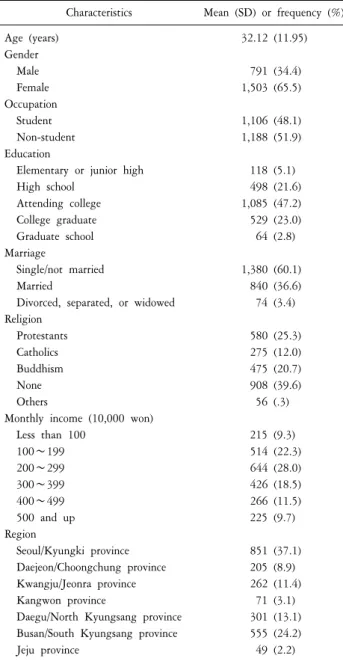
Initially, a total of 2,372 participants were recruited. However, due to a few missing information, only 2,294 participants were included in the analyses. The demographic characteristics of the sample are shown in Table 1. The mean age for the participants was 32.12 years (SD=11.95) old. About one third (34.4%) of the participants were male and 65.5% were females. Almost half of the participants (47.2%) had college degree. Twenty two percent of the participants earned 1,000,000∼1,999,999 Korean Won (KW) monthly, and 28% earned 2,000,000∼2,999,999 KW.
Table 2 shows descriptions of outcome variables.
2. Influencing factors of symptoms of stress Before conducting the regressions we examined zero-order correlations among all the variables to identify possible problems with collinearity among predictors. All the intercorrelations were in the low to moderate ranges, with none exceeding .59, and so no variables were excluded from the subsequent analysis.
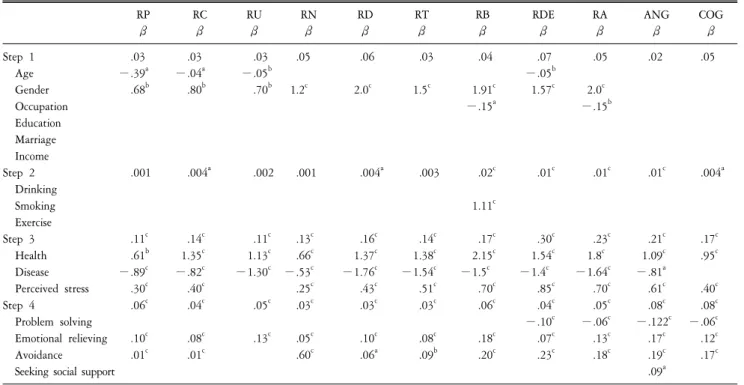
Table 3 shows the four steps in the multivariate regression for
Table 1. Socio-demographic characteristics of participants (N=2,294).
Characteristics Mean (SD) or frequency (%) Age (years)
Gender Male Female Occupation Student Non-student Education
Elementary or junior high High school
Attending college College graduate Graduate school Marriage
Single/not married Married
Divorced, separated, or widowed Religion
Protestants Catholics Buddhism None Others
Monthly income (10,000 won) Less than 100
100∼199 200∼299 300∼399 400∼499 500 and up Region
Seoul/Kyungki province Daejeon/Choongchung province Kwangju/Jeonra province Kangwon province
Daegu/North Kyungsang province Busan/South Kyungsang province Jeju province
32.12 (11.95)
791 (34.4) 1,503 (65.5)
1,106 (48.1) 1,188 (51.9)
118 (5.1) 498 (21.6) 1,085 (47.2) 529 (23.0) 64 (2.8)
1,380 (60.1) 840 (36.6) 74 (3.4)
580 (25.3) 275 (12.0) 475 (20.7) 908 (39.6)
56 (.3)
215 (9.3) 514 (22.3) 644 (28.0) 426 (18.5) 266 (11.5) 225 (9.7)
851 (37.1) 205 (8.9) 262 (11.4)
71 (3.1) 301 (13.1) 555 (24.2) 49 (2.2)
Table 2. Description of outcome variables (N=2,294).
Variables Mean (SD) or frequency (%) Total perceived stress score
Problem solving coping Emotional relieving coping Avoidance coping
Seeking social support coping Psychosomatic symptoms Psychological symptoms No
Yes
5.99 (3.69) 29.22 (9.45) 27.57 (9.16) 18.07 (5.97) 7.76 (3.37) 43.21 (26.11)
2,186 (95.3) 108 (4.7)
each stress symptom. Subjective health status was a significant predictor for all eleven health symptoms. The worse the subjective health status was, participants tended to experience more stress symptoms all types. Similar to subjective health status, having disease was a significant predictor for almost all health indicators except those reflecting cognitive disorganization. Having disease was related to having higher level of health-related symptoms.
Perceived stress level was another significant predictor for almost all health symptoms except upper respiratory symptoms. Emotional coping style was a significant predictor for all 11 health
symptoms. Participants who use more emotional coping style tended to experience higher levels of stress symptoms. Using more social coping style was only significantly predicting higher level of anger symptoms of stress.
Next, eleven symptoms of stress were computed into two variables-psychosomatic symptoms, and psychological symptoms.
Another series of multivariate regressions was then run for these two computed outcomes (Table 4). Age and gender were significant predictors for psychosomatic symptoms. Being younger and women were related to experiencing more somatic symptoms.
In addition, worse in subjective health, having disease, and higher perceived stress level were significantly predicting more psychosomatic symptoms of stress. Among four coping styles, using more emotional and hope-use coping styles predicted more psychosomatic symptoms of stress.
The pattern of predictors for psychological symptoms of stress was different. In predicting psychological symptoms, feeling healthier and perceiving less stress level predicted more psychological symptoms of stress. In addition, using less emotional and hope-use coping styles were significantly related to more psychological symptoms of stress.
DISCUSSION
The current study investigated patterns of predictors for physical and mental health symptoms often found to be associated with stress exposure. Past research on health predictors had found social characteristics and health behaviors as potential predictors of symptoms of stress (Schulz et al., 2000; Bouteyre et al., 2006;
Schnider et al.2007). Prior work also found significant relations
among coping styles and symptoms of stress (Dyson et al., 2006;
Table 3. Multivariate regression analyses for eleven symptom of stress (N=2,294).
RP β
RC β
RU β
RN β
RD β
RT β
RB β
RDE β
RA β
ANG β
COG β Step 1
Age Gender Occupation Education Marriage Income Step 2 Drinking Smoking Exercise Step 3 Health Disease Perceived stress Step 4
Problem solving Emotional relieving Avoidance
Seeking social support .03
−.39
a.68
b.001
.11
c.61
b−.89
c.30
c.06
c.10
c.01
c.03
−.04
a.80
b.004
a.14
c1.35
c−.82
c.40
c.04
c.08
c.01
c.03
−.05
b.70
b.002
.11
c1.13
c−1.30
c.05
c.13
c.05
1.2
c.001
.13
c.66
c−.53
c.25
c.03
c.05
c.60
c.06
2.0
c.004
a.16
c1.37
c−1.76
c.43
c.03
c.10
c.06
a.03
1.5
c.003
.14
c1.38
c−1.54
c.51
c.03
c.08
c.09
b.04
1.91
c−.15
a.02
c1.11
c.17
c2.15
c−1.5
c.70
c.06
c.18
c.20
c.07
−.05
b1.57
c.01
c.30
c1.54
c−1.4
c.85
c.04
c−.10
c.07
c.23
c.05
2.0
c−.15
b.01
c.23
c1.8
c−1.64
c.70
c.05
c−.06
c.13
c.18
c.02
.01
c.21
c1.09
c−.81
a.61
c.08
c−.122
c.17
c.19
c.09
a.05
.004
a.17
c.95
c.40
c.08
c−.06
c.12
c.17
ca
p<.05,
bp<.01,
cp<.001.
RP: peripheral manifestations, RC: cardiopulmonary symptoms, RU: upper airway symptoms, RN: central neurological symptoms, RD: gastrointestinal symptoms, RT: muscle tension, RB: habitual patterns, RDE: depression, RA: anxiety, ANG: anger, COG: cognitive disorganization.
Pina et al., 2008). Very few studies, however, has examined patterns of predictors for different types of symptoms of stress on one study.
As might be expected, the present analysis revealed that regardless of the types of stress symptoms, women experience more health symptoms. However, unlike the other studies, the current study found no relations between health behaviors (drinking, smoking, or exercise) and health symptoms. Instead, self-rated health status, and having disease were significantly related to health symptoms.
When symptoms of stress were analyzed separately, the patterns of predictors were similar for the 11 stress symptoms.
However, when symptoms of stress were combined into two variables (psychosomatic and psychological symptoms of stress), predictor patterns were different. For somatic symptoms, socio-demographic variables (younger, being women), self-rated health, having disease, and higher levels of perceived stress contributed to more somatic symptoms. More importantly, using more emotion-focused coping and avoidance coping styles had
significant influence on experiencing more psychosomatic symptoms. On the other hand, using less emotion-focused and avoidance coping style were related to more psychological symptoms of stress. From the emotion regulation study, Gillanders et al.(2008) found negative relationship between emotion suppression and psychosomatization. Emotion-focused coping could be an instant suppression of emotion regulation. It is considered an instant suppression, because it does not help people to reframe the thoughts or does not help people to reappraise the situation. What it does is to temporarily relieve the arousal of the situation. Hence, when the moment passes, then people have to face with the situation again which could have adverse effect on people’s level of stress symptoms.
Similar to emotion-focused coping, avoidance coping is
considered as one of the disengagement coping (Danhauer et al.,
2009), which focuses on instant avoidance of situation, and the
feeling of distress. Moreover, avoidance coping helps people to
distance themselves from the stressor temporarily, and the denial
creates the discrepancy between the reality and the person’s
Table 4. Multivariate regression analyses for combined symptoms of
stress (N=2,294).
Somatic β Psycho β
Step 1 Age Gender Occupation Education Marriage Income Step 2 Drinking Smoking Exercise Step 3 Health Disease Perceived stress Step 4
Problem solving Emotional relieving Avoidance
Seeking social support
.06
−.15
a6.86
c.003
.202
c6.41
c−6.88
c2.13
c.057
c.54
c.45
c.06
.003 .02
b.018
c−.02
a−.004
b.08
c−.002
b−.003
aa