J Korean Soc Transplant
2006;20:227-233 □ 원 저 □
227
INTRODUCTION
Salvage liver transplantation has been performed for recurrent hepatocellular carcinoma (HCC) or deterioration of liver function after primary liver resection. Initial liver resections in salvage transplant recipients are usually minor in its extent, and thus do not induce serious distortion of gross liver structures or extensive perihepatic adhesion. In performing deceased-donor whole liver graft implantation, a previous history of minor hepatectomy is not regarded as a contraindication for liver transplantation. In contrast, prior performance of a major liver resection such as right a lobectomy makes subsequent recipient hepatectomy technically difficult, due to perihepatic adhesion and distorted liver structures. Thus, only a small number of salvage transplantation cases after major liver resection have been reported.(1,2)
Living donor liver transplantation (LDLT) can also be per- formed as salvage transplantation. Although initial minor hepatec- tomy may be acceptable for salvage LDLT, there are no reports of salvage LDLT following major hepatectomy. Theoretically, salvage LDLT after major liver resection can involve all 4 combinations of prior right or left lobectomy and right or left lobe graft implantation. In practice, we have experienced 3 of these combinations, with the only one not performed being left lobe graft implantation after right lobectomy. We analyzed the technical feasibility of these prior major hepatectomy-graft combinations, with detailed description of perihepatic dissection and hepatic vein reconstruction.
METHODS 1) Patient selection
From February 1997 to March 2006, 1,049 cases of adult 주요 간절제 후 시행하는 구조 생체간이식의 기술
적 타당성 평가
울산대학교 의과대학 서울아산병원 외과
김태영․황 신․이승규․문덕복․안철수․김기훈 박광민․이영주․하태용․송기원․정동환․김범수 문기명
목적: 구조간이식은 간세포암에 대한 1차적인 간절제 후 발생한 재발이나 간기능부전에 대해 시행하는 간이식이 다. 이전에 주요 간절제를 받은 병력은 생체간이식을 시행 하는 데 있어 명확히 불리한 조건이다. 이 연구에서는 구 조 생체간이식 시 이전의 주요 간절제 병력과 이식간절편 의 조합에 대한 기술적인 타당성을 평가하였다. 방법: 저 자들이 시행한 17예의 구조 생체간이식 중 5예는 주요 간 절제 후 시행되었다. 결과: 이전에 좌엽절제술을 받았던 2명은 우엽간절편을 이식받았다. 우엽절제술을 받았던 3 명 중 2명에서는 우엽간절편이 이식되었고 1명에서는 좌 엽간절편이 이식되었다. 수혜자 수술 중 간박리 시 이전 간절단면의 조심스런 박리가 가장 중요한 부분이었다. 일 단 하대정맥이 완전히 박리된 이후에는 다양한 방법의 간 정맥문합이 가능하였다. 문맥, 간동맥 및 담도 문합은 잔 존 구조물을 이용하였다. 결론: 결론적으로, 이전의 좌엽 또는 우엽 절제의 주요 간절제와 좌엽 또는 우엽 생체 부 분 간절편의 모든 조합이 실제적으로 시행 가능하게 보이 기 때문에, 구조 생체간이식의 기술적인 제한은 없다고 생 각된다. (J Korean Soc Transplant 2006;20:227-233) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 중심 단어: 구조간이식, 생체간이식, 간세포암
책임저자:이승규, 서울시 송파구 풍납동 388-1
울산대학교 의과대학 서울아산병원 외과, 138-736 Tel: 02-3010-3485, Fax: 02-474-9027
E-mail: [email protected]
Assessment of Technical Feasibility of Living Donor Liver Transplantation after Prior Major Liver Resection for
Hepatocellular Carcinoma
Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Tae-Young Kim, Shin Hwang, Sung-Gyu Lee, Deok-Bog Moon, Chul-Soo Ahn, Ki-Hun Kim, Kwang-Min Park, Young-Joo Lee, Tae-Yong Ha, Gi-Won Song, Dong-Hwan Jung, Bum-Soo Kim and Ki-Myung Moon
228 대한이식학회지:제 20 권 제 2 호 2006
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
LDLT have been performed in our institution,(3,4) of which 342 recipients (32.6%) were diagnosed as having HCC. Among the latter, 17 (5%) had undergone prior liver resection as treatment for HCC. Major liver resection (resection of 3 seg- ments or more; right or left lobectomy) was performed in 5 patients and minor liver resection (resection of 2 segments or fewer; sectionectomy, segmentectomy or partial hepatectomy) in 12 (Table 1).
In our institution, the indication criteria for salvage LDLT were basically the same as those for primary adult LDLT. In most patients, the extent of recurrent HCC was within the Milan criteria. HCC workup routinely involved positron emission tomo- graphy, radioisotope bone scan, magnetic resonance imaging and chest computed tomography (CT).(5) Recipient hepatic vascular structures were evaluated through dynamic CT with angiographic and other 3-dimensional reconstructions. No patient was excluded during pretransplant evaluation due to prior major liver resection per se.
When deciding the type of partial liver graft from a living donor as salvage LDLT, graft size-to-recipient matching was the most important factor. We tried to make the graft-recipient weight ratio greater than 0.8. Abdominal status following prior liver resection was empirically estimated and simulated using dynamic CT and 3-dimensional reconstruction. Prior liver re- section did not change the type of liver grafts, but dual-graft implantation was not attempted after major liver resection.
2) Surgical techniques for patients with prior major liver resection
In patients who underwent right lobectomy, the hypertrophied left liver was usually heavily adhered to the diaphragm, adrenal, Gerota's fascia, and transverse colon. Meticulous sharp dis- section of the previous liver cut surface was mandatory to attain full mobilization. Blunt dissection was avoided because it induced massive diffuse bleeding from the widely dissected surface. It was especially difficult to control bleeding during dissection around the middle hepatic vein (MHV) trunk at the liver cut surface. The running course of MHV was confirmed by pretransplant CT images and intraoperative ultrasonography.
In patients prone to bleeding, alternating dissection of the right- and left-side perihepatic areas was effective for both bleeding control and time-saving; temporary packing to one side could cease or ameliorate the diffuse bleeding, while dissection of the other side continued. Cavitron ultrasonic aspirator was also a useful tool to detach the heavy or stony-hard adhesions while lowering the risk of iatrogenic injury to the major hepatic veins.
In patients with prior left lobectomy, the right liver was usually heavily adhered to the stomach, duodenum, omentum and transverse colon. Meticulous sharp dissection of the previous liver cut surface was the initial step during recipient hepatectomy. Since the MHV trunk was also exposed at the liver cut surface, patients were at risk of bleeding.
Once the cut surface adhesion was fully severed, the remaining mobilization procedures were the same as during ordinary LDLT. Hepatic hilar adhesion was usually not severe because the hepatic hilum had usually not been dissected extensively during prior hepatectomy for HCC. To accommodate a sizable liver graft, either the right or left subphrenic space was extensively dissected, depending on the graft type.
For secure hepatic venous reconstruction, the recipient inferior vena cava (IVC) was fully isolated, as during ordinary adult LDLT. Various methods of graft hepatic vein reconstruction were performed (Fig. 1).(6)
3) Statistical analysis
Mean values with standard deviation and median values with range were used for numeric data. The significance of differen- ces was assessed by chi-square, Fisher's exact test and t-test.
Survival curves were estimated by the Kaplan-Meier method and compared by the log-rank test. Statistical significance was set at P<0.05.
Table 1. Profiles of patients who underwent living donor liver transplantation after prior major and minor liver resections for hepatocellular carcinoma
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Prior major liver Prior minor liver
P-value resection (n=5) resection (n=12)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Patient profiles
Age (years) 52.4±9.3 52.4±61 0.349 Male sex 2 (40%) 10 (83.3%) 0.116 MELD score 11.6±2.8 12.7±7.0 0.749
GRWR 1.06±0.22 1.05±0.21 0.941
Within the Milan
3 (75%) 9 (75%) 0.756
criteria*
Graft
Right lobe graft 4 (80%) 8 (66.7%) Left lobe graft 1 (20%) 2 (16.7%) Dual grafts 0 (0%) 2 (16.7%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*2 patients had no evidence of recurrence. MELD = Model for end-stage liver disease; GRWR = graft-recipient weight ratio.
Tae-Young Kim, et al:Salvage Living Donor Liver Transplantation 229 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
RESULTS
1) Patient profiles
Patient profiles are summarized at Table 1. In 15 of 17 patients, recurrent HCC was the main problem of salvage LDLT; other 1 patient experienced progressive deterioration of the liver function without HCC recurrence 7 years after right lobectomy, and 1 patient was in a state of acute hepatic failure after partial hepatectomy that was performed 1 month earlier.
The mean interval between initial liver resection and LDLT was 3.1±2.2 years (1 month to 7 years).
2) Surgical profiles of salvage LDLT after major liver resection
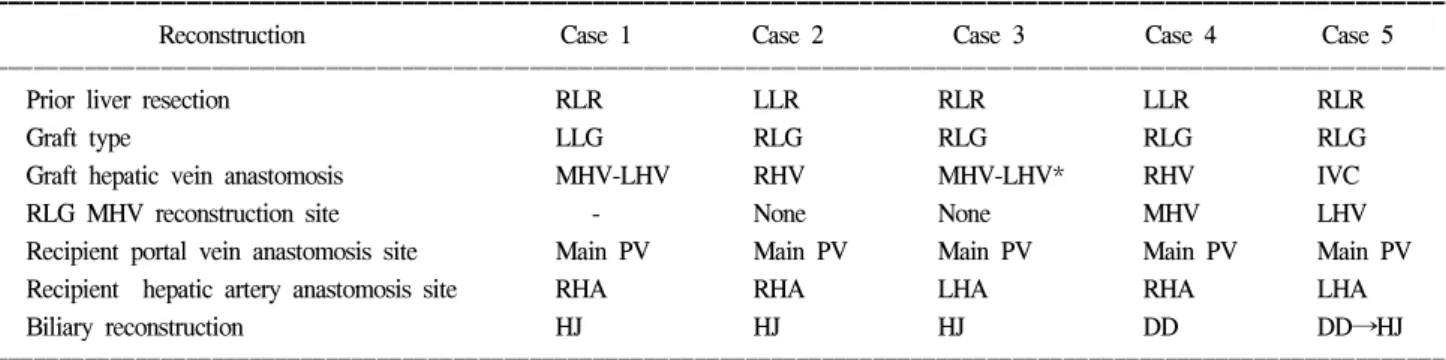
Graft reconstruction in 5 patients with prior major resection were summarized at Table 2.
3) Comparison of operation profiles and posttransplant complications
Operation profiles and posttransplant complications are summarized in Table 3. Operation time was not significantly prolonged in the salvage LDLT group after major liver resection. Additional operation time for dissection of the liver cut surface was about 2 hours each in 2 patients who underwent prior right lobectomy. The number of units of packed red blood cells transfused was variable whether or not autotransfusion system was used. The incidences of various posttransplant comp- lications other than bleeding were similar in the prior major and minor liver resection groups. There was no disturbance of hepatic inflow or outflow in the 4 surviving patients who received right lobe grafts after major liver resection (Fig. 2).
4) Patient survival and HCC recurrence
With median follow-up of 31 months, 1-, 3-, 5-year overall Fig. 1. Sequence of hepatic vein reconstruction in a patient with prior right lobectomy (case 5). (A) The retrohepatic inferior vena cava (IVC) was fully dissected. (B) The IVC was side-clamped and a longitudinal incision was made. (C) An autologous saphenous vein patch was attached along the periphery of the graft right hepatic vein orifice at the back table. This cuff was sutured to the newly-made IVC orifice. (D) Middle hepatic vein tributaries of the graft were reconstructed to the left hepatic vein trunk using a cryopreserved iliac artery graft.
A B
D C
230 대한이식학회지:제 20 권 제 2 호 2006
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
patient survival rates after salvage LDLT were 88.2%, 64.8%
and 54%, respectively. When confining to within the Milan criteria, the 1-, 3-, 5-year survival rates were all 80% because there were only two cases of early patient deaths which were unrelated to HCC recurrence.
DISCUSSION
Salvage liver transplantation has been used to treat recurrent HCC or progressive deterioration of hepatic function,(1,2) and LDLT has been used to treat HCC.(7) In our institution, HCC was detected in about 30% of explanted livers after adult LDLT, and 5% of these patients underwent salvage transplan- tation. However, salvage LDLT after major liver resection was rarely performed, even in our institution which has extensive experience with adult LDLT.
We found that the overall operative risk from prior liver resection was not higher than in patients without prior resec- tion. Only 1 patient, the first with prior major liver resection and the 14th adult LDLT case in our series, died from bleeding-
associated multi-organ failure. Our subsequent increased ex- perience in surgical techniques and postoperative management has reduced the surgical risk which was caused by prior liver resection, such that the time in surgery and the number of red cell units transfused were not serious problems. Since the operation profiles and complication rates were very similar between patients with prior major and minor liver resections, these two groups of patients had similar risks. However, the prior performance of major liver resection per se indicates that severe liver cirrhosis was not combined at the time of initial liver resection. We found that pretransplant liver function was relatively favorable in 5 patients with prior major liver resection.
When performing recipient hepatectomy after prior liver resection, especially right hepatectomy, there are two important technical considerations. The first is the technical feasibility of recipient liver isolation with tolerable amount of bleeding. In fact, minor liver resection usually preserved most of the gross liver structures intact. However, following right lobectomy, heavy adhesion frequently develops and minute collaterals could penetrate into the adhesion if there was portal hypertension.
Table 2. Graft reconstruction in 5 patients with prior major liver resection
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Reconstruction Case 1 Case 2 Case 3 Case 4 Case 5
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Prior liver resection RLR LLR RLR LLR RLR
Graft type LLG RLG RLG RLG RLG
Graft hepatic vein anastomosis MHV-LHV RHV MHV-LHV* RHV IVC
RLG MHV reconstruction site - None None MHV LHV
Recipient portal vein anastomosis site Main PV Main PV Main PV Main PV Main PV
Recipient hepatic artery anastomosis site RHA RHA LHA RHA LHA
Biliary reconstruction HJ HJ HJ DD DD→HJ
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*with transverse extension toward the right side and partial closure of the left hepatic vein orifice. IVC = inferior vena cava; LLR = left lobe resection; RLR = right lobe resection; LLG = left lobe graft; RLG = right lobe graft; MHV = middle hepatic vein; LHV = left hepatic vein;
RHV = right hepatic vein; PV = portal vein; RHA = right hepatic artery; LHA = left hepatic artery; HJ = hepaticojejunostomy; DD = duct-to-duct anastomosis; DD→HJ = conversion from DD to HJ.
Table 3. Comparison of operation profiles and complications of patients who underwent living donor liver transplantation after prior major and minor liver resections for hepatocellular carcinoma
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Prior major liver resection Prior minor liver resection
P-value
(n = 5) (n = 12)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Perioperative mortality 1 (20%) 0 (0%) 0.294
Operation time (min) 1,034±283 970±245 0.645
Packed red blood cell transfusion (units)* 13.2±8.8 12.5±9.4 0.888
Bleeding complication 1 (20%) 4 (33.3%) 0.528
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*Regardless autotransfusion.
Tae-Young Kim, et al:Salvage Living Donor Liver Transplantation 231 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Inattentive dissection of such perihepatic adhesion would pro- duce numerous uncontrollable sites of pinpoint bleeding at the dissection surface. This technical difficulty may be one of the reasons many transplant surgeons are unwilling to perform salvage transplantation after major hepatectomy. Similar situations of difficult dissection were encountered during late retrans- plantation after LDLT. Our experience with salvage transplan- tation and late retransplantation indicates that steady meticulous sharp dissection is the only method to successfully determine the adequate dissection plane. Once the cut surface adhesion is fully severed, other mobilization procedures are the same as those in ordinary LDLT. Although our experience of salvage deceased-donor whole liver transplantation is limited, the same principle would be also applicable.
The second technical consideration is secure reconstruction of the hepatic vein outflow, which depends on the anatomical characteristics of the partial liver graft and hepatic vein stump at the recipient IVC. During implantation of a right lobe graft, patch venoplasty to the graft RHV stump made the recons-
truction process comfortable because it afforded some redun- dancy.(8,9) We think that any method of hepatic vein recon- struction can be applicable if the recipient IVC is fully dissected.(6)
The main or remaining first-order portal vein can be used for portal vein anastomosis. The left hepatic artery can be used after right lobectomy as well as for primary LDLT using a right lobe graft. If no innate hepatic artery is available, the right gastroepiploic artery becomes the most preferable source of arterial inflow, due to its invariable anatomical location, size, and length. This artery may often appear too small to use for reconstruction of the right hepatic artery, but it can be instantly dilated after clamping for a few minutes.(10,11)
Biliary complications remain the most intractable problem following LDLT.(12,13) Since hilar structures were often dissected during prior liver resection, abnormal hilar adhesion was frequently detected during recipient hepatectomy. In this series, a right lobe graft recipient (case 5) showed unusual segmental stenosis of the recipient bile duct after duct-to-duct Fig. 2. Computed tomography (CT) follow-up of the right lobe graft outflow showing absence of significant anastomotic stenosis. (A) 3-dimensional reconstruction of 2-month CT of the case 2. (B) Right hepatic vein anastomosis on 2-month CT of the case 3.
(C) Right hepatic vein anastomosis site was seen at the 2-month CT of the case 4. (D) Right hepatic vein anastomosis on 2-month CT of the case 5. Reconstructed segment VIII vein was also seen.
A B
D C
232 대한이식학회지:제 20 권 제 2 호 2006
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ anastomosis. Following initial right lobectomy, the native bile
duct was subsequently deviated according to dextro-rotation of the remnant left liver. Retrospective analysis showed that it was not reasonable to align the deviated recipient duct with the ordinary right lobe graft duct opening. Thus, in patients with prior right lobectomy, duct-to-duct biliary reconstruction methods should be prudently selected during salvage LDLT.
Our salvage LDLT cases demonstrated that various combina- tions of recipient prior hepatectomy and graft were possible in practice. Technically, it should be feasible to utilize all 4 combinations of salvage LDLT - right or left lobe graft and prior right lobectomy or left lobectomy - although we did not perform one combination, left lobe graft implantation after right lobectomy. It is also important to prudently plan any salvage LDLT because of the difficulty of dissection of perihepatic adhesions from previous abdominal operation. Lack of experi- ence in our first salvage LDLT after major liver resection may have caused serious postoperative bleeding.
In conclusion, our results indicate that salvage LDLT can be used to treat recurrent HCC or hepatic failure, even after major liver resection. In practice, every combination of recipient prior hepatectomy and living donor liver graft seems to be feasible for salvage LDLT.
REFERENCES
1) Belghiti J, Cortes A, Abdalla EK, Regimbeau JM, Prakash K, Durand F, Sommacale D, Dondero F, Lesurtel M, Sauvanet A, Farges O, Kianmanesh R. Resection prior to liver transplan- tation for hepatocellular carcinoma. Ann Surg 2003;238:885-92.
2) Adam R, Azoulay D, Castaing D, Eshkenazy R, Pascal G, Hashizume K, Samuel D, Bismuth H. Liver resection as a bridge to transplantation for hepatocellular carcinoma on cir- rhosis: a reasonable strategy? Ann Surg 2003;238:508-18.
3) Moon DB, Lee SG. Adult-to-adult living donor liver trans- plantation at the Asan Medical Center. Yonsei Med J 2004;
45:1162-8.
4) Hwang S, Lee SG, Lee YJ, Sung KB, Park KM, Kim KH, Ahn CS, Moon DB, Hwang GS, Kim KM, Ha TY, Kim DS, Jung
JP, Song GW. Lessons learned from 1000 living donor liver transplantations in a single center: how to make living donations safe. Liver Transpl 2006;12:920-7.
5) Teefey SA, Hildeboldt CC, Dehdashti F, Siegel BA, Peters MG, Heiken JP, Brown JJ, McFarland EG, Middleton WD, Balfe DM, Ritter JH. Detection of primary hepatic malignancy in liver transplant candidates: prospective comparison of CT, MR imaging, US, and PET. Radiology 2003;226:533-42.
6) Lee SG. Techniques of reconstruction of hepatic veins in living- donor liver transplantation, especially for right hepatic vein and major short hepatic veins of right-lobe graft. J Hepatobiliary Pancreat Surg 2006;13:131-8.
7) Todo S, Furukawa H. Living donor liver transplantation for adult patients with hepatocellular carcinoma: experience in Japan. Ann Surg 2004;240:451-9.
8) Hwang S, Lee SG, Park KM, Kim KH, Ahn CS, Moon DB, Ha TY. Quilt venoplasty using recipient saphenous vein graft for reconstruction of multiple short hepatic veins in right liver grafts. Liver Transpl 2005;11:104-7.
9) Hwang S, Lee SG, Ahn CS, Park KM, Kim KH, Song GW, Kim DS. Composite clustered reconstruction of multiple middle hepatic vein branches in right lobe graft. Liver Transpl 2005;
11:1144-6.
10) Ahn CS, Lee SG, Hwang S, Moon DB, Ha TY, Lee YJ, Park KM, Kim KH, Kim YD, Kim KK. Anatomic variation of the right hepatic artery and its reconstruction for living donor liver transplantation using right lobe graft. Transplant Proc 2005;37:1067-9.
11) Tannuri U, Maksoud-Filho JG, Silva MM, Suzuki L, Santos MM, Gibelli NE, Ayoub AA, Velhote MC, Pinho-Apezzato ML, Maksoud JG. An alternative method of arterial recons- truction in pediatric living donor liver transplantation with the recipient right gastroepiploic artery. Pediatr Transplant 2006;
10:101-4.
12) Hwang S, Lee SG, Sung KB, Park KM, Kim KH, Ahn CS, Lee YJ, Lee SK, Hwang GS, Moon DB, Ha TY, Kim DS, Jung JP, Song GW. Long-term incidence, risk factors, and mana- gement of biliary complications after adult living donor liver transplantation. Liver Transpl 2006;12:831-8.
13) Fan ST, Lo CM, Liu CL, Tso WK, Wong J. Biliary recons- truction and complications of right lobe live donor liver transplantation. Ann Surg 2002;236:676-83.
Tae-Young Kim, et al:Salvage Living Donor Liver Transplantation 233 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Purpose: Liver transplantation has been performed for recurrent hepatocellular carcinoma (HCC) or deterioration of liver function after prior primary liver resection. Prior major liver resection per se is an unfavorable condition for living donor liver transplantation (LDLT). We analyzed the technical feasibility of prior major hepatectomy-graft combinations for salvage LDLT. Methods: Of the 17 patients who underwent salvage LDLT, 5 underwent prior major liver resection. Results: Two patients with prior left lobectomy received right lobe graft, whereas, of the 3 patients with prior right lobectomy, 2 received right lobe graft and 1 received left lobe graft.
During recipient hepatectomy, it was necessary to perform meticulous sharp dissection of the previous liver cut surface to attain full mobilization. Different methods of hepatic vein reconstruction were applied after the recipient inferior vena cava was fully dissected. Reconstruction of the portal vein, hepatic artery and bile duct were performed on case by case basis depending on the remnant hilar structures. Conclusion: In conclusion, every combination of recipient prior right or left lobectomy and living donor right or left liver graft seems to be feasible for salvage LDLT. (J Korean Soc Transplant 2006;20:227-233)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Salvage liver transplantation, Living donor liver transplantation, Hepatocellular carcinoma