Background : The prevalence of adverse drug reactions (ADRs) in critically ill patients is estimated to be high due to several reasons such as the severity of their underlying diseases, the use of mul- tidrug agents, and the changes in pharmacokinetic parameters. The objectives of this study were to understand the status of ADRs that occurred in the surgical intensive care unit (SICU) and to suggest an optimal monitoring method.
Methods : We studied adult patients who were hospitalized in the SICU of the Seoul National University Hospital, a tertiary care hospital in South Korea, between August 3, 2015 and September 11, 2015. ADRs were detected by prospective monitoring, retrospective monitoring, and signal moni- toring and assessed by a pharmacist in terms of causality, severity, preventability, seriousness, recovery, and types. The sensitivity of each monitoring method and the positive predictive value (PPV) of the signals were also calculated.
외과계 중환자실에서의 약물유해반응 탐색에 대한 방법론적 접근
신진아
a, 류수현
a, 사은영
a, 이은지
a, 서성연
a, 조윤숙
a, 한현주
a, 이진
b, 손혜련
b, 강동윤
b, 강혜련
b,c,�서울대학교병원 약제부
a, 약물유해반응센터
b, 내과
cA Methodological Approach for Detecting Adverse Drug Reactions in the Surgical Intensive Care Unit
Jina Shin
a, Su-Hyun Ryu
a, Eunyoung Sa
a, Eun Ji Lee
a, Sung Yun Suh
a, Yoon Sook Cho
a, Hyeon-Joo Hahn
a, Jin Lee
b, Hyeryeon Son
b, Dong-Yoon Kang
band Hye-Ryun Kang
b,c,�Department of Pharmacy, Seoul National University Hospital
aRegional Pharmacovigilance Center, Seoul National University Hospital
bDepartment of Internal Medicine, Seoul National University Hospital
c101 Daehak-ro, Jongno-gu, Seoul, 03080, Republic of Korea
투고일자 2017.6.13; 심사완료일자 2017.7.27; 게재확정일자 2017.9.8
�교신저자 강혜련 Tel:02-2072-0820 E-mail:[email protected]
Original Article
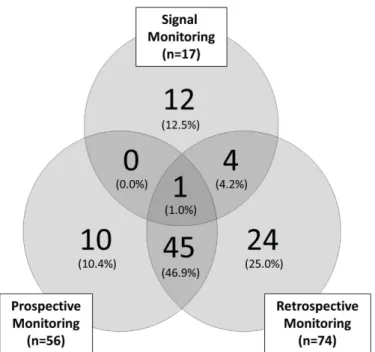
Results : A total of 96 ADRs (36.6%) was identified from prospective monitoring (n=56), retrospective monitoring (n=74), and signal monitoring (n=17). Most ADR cases were either possible or probable, and 56 (58.3%), 29 (30.2%), 11 (11.5%) cases were mild, moderate, and severe, respectively. Only one case was detected by any of the monitoring methods and there was little overlap between the ADR cases found by each of the monitoring strategies. Among the 206 alerts generated by the signal moni- toring, 25 were found to be associated with ADRs and the overall positive predictive value was calcu- lated as 0.12.
Conclusion : The incidence of ADRs was 36.6% in 262 patients hospitalized in the SICU. According to the monitoring methods, there was a difference in the detection of ADRs that occurred in critically ill patients, suggesting that prospective, retrospective, and signal monitoring are complementary.
[Key words] Drug-related side effects and adverse reactions, Adverse drug reaction reporting sys- tems, Intensive care units, Critical care, Postoperative care
연구 배경 및 목적
약물유해반응(adverse drug reaction, ADR)이란 의약품 등을 정상적인 용법에 따라 투여하고 사용하는 중 발생하는 유해하고 의도하지 않은 반응으로 해당 의 약품 등과의 인과관계를 배제할 수 없는 경우를 의미한 다.
1)미국에서는 전체 사망 원인 중 약 4.6%가 약물유 해반응에 의한 사망이었다고 보고된 바 있으며,
2)약물 유해반응은 사망률 뿐만 아니라 환자의 재원 일수와 진 료비를 증가시키기 때문에 주요 의료 문제로 부각되고
있다.
3)-4)중환자는 다른 환자군에 비해 질환의 중증도, 다장기 부전(multi-organ failure), 다약제 사용, 흔하지 않 은 약물 사용(unusual prescription drugs), 빈번한 구두 처방 등으로 인해 약물유해반응 발생 빈도가 높고 이로 인한 피해도 보다 심각하다.
5)-6)일반 병동에 비해 중환자실에서 약 2배의 빈도로 약물유해반응이 발생했 다고 보고된 바 있으며,
5)외과계 중환자실의 재원 기간 이 약물유해반응 발생 시 약 2.31일 연장되었다는 연구 결과도 발표되었다.
4)약물유해반응은 경제적 부담 또한 가중시키는데 내과
계 중환자실에서 약물유해반응과 관련된 비용은 연간 약 85만달러로 추정된 바 있다.
7)반면 외과계 중환자실 담당 약사의 처방 중재를 통해 약물유해반응을 적극적 으로 예방한 결과 5개월 동안 약 2만4천달러가 절감되 었다는 연구 결과가 보고되었다.
8)따라서 중환자에서 빈번하게 발생하는 약물유해반응을 파악하고 이에 대 한 예방 대책을 마련함으로써 약물유해반응으로 인한 피해를 최소화하는 것이 중요하다. 하지만 내과계 중환 자에 비해 외과계 중환자에 대한 약물유해반응 현황에 대한 정보는 다소 부족한 것이 현실이다.
6)외과 환자는 외과적 수술 또는 시술에 의해 일시적인 생리학적 변화 가 발생 가능하고,
9)외과적 수술 또는 시술 후 주로 사 용되는 약제도 다르기 때문에 내과 환자와 약물유해반 응의 발생 양상이 다를 가능성을 배제할 수 없다.
한편, 약물유해반응 현황을 파악하기 위해 의료진의
자발적 보고, 전향적 모니터링, 후향적 의무기록 검토
모니터링, 실마리정보 모니터링 등의 다양한 방법이 적
용 가능하다.
10)자발적인 보고, 후향적 의무기록 검토
모니터링, 그리고 전산시스템을 활용한 실마리정보 모
니터링을 적용하여 약물유해반응을 탐색한 연구에서
각 모니터링 방법에 따라 검출되는 약물유해반응의 종
류가 다를 수 있음을 시사하였다.
11)하지만 이는 중환자 실과 일반 병동에 입원해 있는 모든 성인 환자를 대상 으로 진행된 연구로 중환자를 대상으로 적용하기에는 한계가 있다. 즉, 외과계 중환자의 약물유해반응 현황 을 파악하기 위해 어떠한 방법이 최적인지 아직 명확하 게 알려져 있지 않다.
따라서 본 연구에서는 외과계 중환자를 대상으로 전 향적 모니터링, 후향적 의무기록 검토 모니터링, 이상 검사소견 실마리정보 모니터링으로 약물유해반응 발생 을 조사함으로써 외과계 중환자실에서의 약물유해반응 현황과 최적의 약물유해반응 감시 방법에 대해 알아보 고자 하였다.
연구방법
1. 연구 대상
본 연구는 2015년 8월 3일부터 2015년 9월 11일까지 서울대학교병원 외과계 중환자실(32 beds)에 입실하 여 치료를 받은 19세 이상의 성인 환자를 대상으로 하 였다. 단, 24시간 이내 다른 병동으로 전동, 퇴원 또는 사망하거나 외과계 중환자실에 입실한 내과 환자는 연 구 대상에서 제외하였다. 동일 환자가 퇴실 후 다시 외 과계 중환자실에 입실한 경우 다른 환자로 간주하였다.
2. 자료 수집
연구 기간 내 외과계 중환자실에 대해 전향적 모니터 링, 후향적 의무기록 검토 모니터링, 이상검사소견 실 마리정보 모니터링의 세가지 방법으로 약물유해반응 모니터링을 실시하였다. 전향적 모니터링의 경우 외과 계 중환자실 담당 약사 1명이 연구 대상의 전자의무기 록(electronic medical record, EMR)을 분석하여 실 시간으로 약물유해반응을 탐색하였다. 후향적 의무기 록 검토 모니터링의 경우 전향적 모니터링 수행 약사와 다른 외과계 중환자실 담당 약사 1명이 전향적 모니터 링의 결과를 알지 못한 상태에서 연구 대상의 전자의무 기록을 검토하여 후향적으로 약물유해반응을 탐색하였 다. 이상검사소견 실마리정보 모니터링의 경우 여러 문 헌 조사를 통해 혈액장애(hematologic disorder), 응
고장애(coagulation disorder), 간독성(hepatotoxic- ity), 신독성(nephrotoxicity), 전해질불균형(elec- trolyte imbalance)과 관련된 이상 검사 수치 및 조건 을 설정하였고,
6),11)-14)이에 따라 약물유해반응을 탐색하 였다(Table 1). 관련 임상 검사를 나타낼 수 있는 질환 명이 있는 경우 이상검사소견 실마리정보 모니터링에 서 제외하였다(Table 1).
3. 분석 방법
각 약물유해반응 모니터링 방법에서 발견된 약물유 해반응 의심사례는 원인 약물과의 인과 관계를 파악하 기 위해 World Health Organization-Uppsala Monitoring Center (WHO-UMC) causality crite- ria에 따라 평가되었다. 확실함(certain), 가능성 높음 (probable/likely), 가능성 있음(possible), 가능성 희 박(unlikely), 자료보완/분류보류(conditional/
unclassified), 평가/분류불가(unassessable/
unclassifiable)로 약사가 평가하였으며, 이 중 확실 함, 가능성 높음, 가능성 있음에 해당하는 경우의 사례 들만 약물유해반응으로 간주하였다.
15)-16)약물유해반응 의 임상 증상은 World Health Organization- Adverse Reaction Terminology (WHO-ART) 092 버전에 따라 분류하였다.
약물유해반응의 중증도(severity)는 LDS scale에 따
라 경증(mild), 중등증(moderate), 중증(severe)으로
평가하였다.
12),17)그리고 약물유해반응의 예방 가능성
(preventability)과 중대성(seriouness)은 각각
Schumock and Thornton’ s criteria,
18)식품의약품
안전처 고시 제 2014-97호「의약품등 안전성 정보관
리 규정 일부개정」
19)에 따라 평가하였다. 중대한(seri-
ous) 약물유해반응은 사망을 초래하거나 생명을 위협
하는 경우, 입원 또는 입원기간의 연장이 필요한 경우,
지속적 또는 중대한 불구나 기능저하를 초래하는 경우,
선천적 기형 또는 이상을 초래하는 경우, 기타 의학적
으로 중요한 상황인 경우로 정의되는데,
19)이 중 불구나
기능저하 항목의 경우 객관적인 기준 값이 제시되어 있
지 않으므로 본 연구에서는 Common Terminology
Criteria for Adverse Events (CTCAE) version 4.03
을 기준으로 grade 3 이상에 해당 시 중대한 약물유해
반응으로 평가하였다.
또한 약물유해반응의 회복 여부에 대해 조사하였으 며, 병리 기전에 따라 Type A 약물유해반응과 Type B 약물유해반응으로 분류하였다. 과용량, 부작용, 이차효 과, 약물상호작용에 의해 발생하는 약물유해반응의 경 우 Type A로, 불내성, 약물 특이반응, 약물 알레르기, 가성 알레르기에 의해 발생하는 약물유해반응의 경우 Type B로 구분하였다.
20)-21)이후 약물유해반응 모니터링 방법에 따라 검출된 약 물유해반응의 특징을 비교하여 보았고, 각 모니터링 방 법의 약물유해반응 검출 능력을 평가하기 위해 민감도 (sensitivity)를 계산하였다. 민감도는 각 모니터링 방 법으로 확인된 약물유해반응의 수를 연구 기간 내 발생 한 총 약물유해반응의 수로 나눈 값으로 정의하였다.
16)또한 이상검사소견 실마리정보 모니터링에서 사용된 이상 검사 수치 및 조건의 적절성을 평가하기 위해 양
성예측도(positive predictive value, PPV)를 계산하 였으며, 이는 각 조건에 따라 추출된 약물유해반응 의 심사례 중 약물유해반응으로 평가된 사례의 수를 총 약 물유해반응 의심사례의 수로 나눈 값으로 정의하였
다.
11)-13)수집된 모든 자료는 Microsoft Office Excel
2013을 이용하여 분석하였다.
4. 연구대상자보호
본 연구는 서울대학교 의과대학/서울대학교병원 의 학연구윤리심의위원회의 승인을 받아 진행하였다(IRB No. 1607-074-776).
연구결과
총 96건(36.6%)의 약물유해반응이 확인되었으며, 경
WBC=white blood cell, PT=prothrombin time, INR=international normalized ratio, ALT=alanine transaminase, AST=aspartate transaminase, ALP=alkaline phosphatase, Cr=creatinine, CrCl=creatinine clearance
Signal criteria with description of associated laboratory abnormalities and rules Category
Table 1. Signals for monitoring adverse drug reactions
Hematologic disorder 1. WBC 3,500 /mm3
2. Platelet 50,000 ~ 120,000 /mm3 3. Eosinophil 800 /mm3
+ on causative medications for more than 5 days
- exclude related disease that may cause such laboratory abnormalities
Hepatotoxicity 1. Bilirubin, total 1.5 mg/dL
2. ALT 100 IU/L and ALT/AST ratio 0.5 3. ALP 350 IU/L
+ on causative medications for more than 4 days - exclude related hepatic diseases
Nephrotoxicity 1. Cr 1.3 mg/dL
2. CrCl 60 mL/min
+ on causative medications for more than 3 days - exclude related kidney diseases
Electrolyte imbalance 1. Serum K 5.7 mmol/L 2. Serum Na 130 mmol/L
+ on causative medications for more than 3 days
- exclude related kidney diseases that may cause hyperkalemia or hyponatremia Coagulation disorder PT INR 3.6
- exclude related coagulopathy or hepatic diseases
No. (%) of ADRs Prospective
(n=56)
Retrospective (n=74)
Signal (n=17)
Total (n=96) Characteristic
Table 2. Characteristics of detected adverse drug reactions
Severity
Severe 5 (8.9) 9 (12.2) 4 (23.5) 11 (11.5)
Moderate 15 (26.8) 17 (23.0) 8 (47.1) 29 (30.2)
Mild 36 (64.3) 48 (64.9) 5 (29.4) 56 (58.3)
Causality
Certain 1 (1.8) 1 (1.4) 0 (0.0) 1 (1.0)
Probable 32 (57.1) 42 (56.8) 1 (5.9) 47 (49.0)
Possible 23 (41.1) 31 (41.9) 16 (94.1) 48 (50.0)
Seriousness
Serious 8 (14.3) 14 (18.9) 10 (58.8) 23 (24.0)
Not serious 48 (85.7) 60 (81.1) 7 (41.2) 73 (76.0)
Preventability
Preventable 12 (21.4) 11 (14.9) 4 (23.5) 17 (17.7)
Not preventable 44 (78.6) 63 (85.1) 13 (76.5) 79 (82.3)
Clinical manifestation
Cardiovascular 8 (14.3) 10 (13.5) - 12 (12.5)
Metabolic & nutritional 1 (1.8) 8 (10.8) 6 (35.3) 13 (13.5)
Gastrointestinal system 17 (30.4) 20 (27.0) - 21 (21.9)
Hematologic 4 (7.1) 1 (1.4) 2 (11.8) 6 (6.3)
Liver & biliary system 1 (1.8) 1 (1.4) 5 (29.4) 6 (6.3)
Urinary system 2 (3.6) 4 (5.4) 4 (23.5) 5 (5.2)
Nervous system & psychiatric 22 (39.3) 26 (35.1) - 29 (30.2)
Others 1 (1.8) 4 (5.4) - 4 (4.2)