98 Copyright 2015 The Korean Society of Neuro-Ophthalmology http://neuro-ophthalmology.co.kr
크립토코쿠스 수막염에 의한 뇌간경색에서 발생한 눈돌림신경마비와 핵간안근마비
도영록·박재한
대구가톨릭대학교병원 신경과
Oculomotor Nerve Palsy and Internuclear Ophthalmoplegia Associated with Brainstem Infarction in Cryptococcal Meningitis
Youngrok Do, MD, Jae Han Park, MD
Department of Neurology, Catholic University of Daegu, School of Medicine, Daegu, Korea
An 80-year-old man with chronic hepatitis C suffered a sudden decrement of mental status and fever. Oculomotor examination re- vealed internuclear ophthalmoplegia in the right eye and oculomotor nerve palsy in the left eye. Diffusion-weighted MRI showed high signals in the right dorsal pons and left upper midbrain. The gadolinium-enhanced MRI also showed prominent leptomenin- geal enhancement of ventral midbrain and cerebral hemisphere. In cerebrospinal fluid analysis, india ink test and fungus culture were negative, but cryptococcal antigen was positive. Internuclear ophthalmoplegia and oculomotor nerve palsy may develop due to ischemic complication of cryptococcal meningitis.
Keywords: Internuclear ophthalmoplegia; Oculomotor nerve palsy; Cryptococcal meningitis
서 론
크립토코쿠스증은 후천성면역결핍증(AIDS)같이 면역이 억제된 환자에서 주로 발생하지만 특별한 원인이 없는 환자에서도 나타날 수 있다. 수막뇌염(meningoencephalitis)이 가장 흔한 형태로 두통, 의식 변화, 발열 등의 전형적인 증상 외에도 다양한 이상소견을 보일 수 있 다.1 감염에 의한 뇌압의 증가로 인해 시각상실, 유두부종 그리고 안근 마비(ophthalmoplegia) 등이 나타날 수 있으며, 혈관의 침범에 의해 뇌 경색이 발생하기도 한다.2,3 하지만 크립토코쿠스 수막염에서 발생하 는 뇌경색은 뇌간을 침범하는 경우는 드물고, 핵간안근마비(internu- clear ophthalmoplegia, INO)와 눈돌림신경마비를 동시에 보이는 경우 는 없었다.3 저자들은 크립토코쿠스 수막염에 의한 뇌간경색에서 INO와 눈돌림신경마비를 보인 환자를 경험하였기에 보고한다.
증 례
80세 남자가 1일 전부터 발생한 두통과 의식저하를 주소로 응급실 로 왔다. 환자는 C형 간염 보균자로 본원 소화기 내과에서 추적관찰 중이었으며, 항바이러스제나 면역억제제를 복용하지는 않았다. 내원 10일 전부터는 식사를 잘하지 못하고 거동이 힘들어져 주로 누워 지 냈다고 하였다. 내원 당시 38.3°C의 발열이 있었고 의식은 혼미(stupor) 하였으며, 경부경직을 보였다. 신경학적 검사에서 좌측의 완전한 눈꺼 풀처침과 함께 좌안의 동공이 6 mm로 확장되어 있었고, 빛 반사가 보 이지 않았으며 전방주시에서 좌안이 외하방으로 편위되어 있어 좌측 눈돌림신경마비에 합당하였다(Fig. 1A and C). 동향운동(version), 단 안운동(duction), 눈모음(convergence) 그리고 회선 검사는 혼미한 의 식으로 인해 정확하게 시행할 수는 없었지만 정면 주시에서 우안도
Correspondence to: Jae Han Park, MD
Department of Neurology, Catholic University of Daegu, School of Medicine, Daegu Catholic University Hospital, 33 Duryugongwon-ro 17-gil, Nam-gu, Daegu 42472, Korea Tel: +82-53-650-3626; Fax: +82-53-654-9786; E-mail: [email protected]
Received: Sep. 8, 2015 / Accepted: Sep. 21, 2015
CASE REPORT
ISSN: 2234-0971 대한안신경의학회지: 제5권 제2호
Clin Neuroophthalmol 5(2):98-100, December 2015
크립토코쿠스 수막염에 의한 뇌간경색에서 발생한 눈돌림신경마비와 핵간안근마비 • 도영록 외
Clin Neuroophthalmol 5(2):98-100, December 2015 http://neuro-ophthalmology.co.kr 99
약간 외측으로 편위되어 있었고, 좌측을 보려고 할 때 우안의 내전장 애를 보이며 좌안에서 미약한 외전안진을 보여 우측의 INO를 의심할 수 있었다(Fig. 1B and D). 안구머리반사(oculocephalic reflex)를 통해 서도 우안의 내전장애는 극복되지 않았고, 혼미한 의식으로 자발적 인 수직 안구운동은 정확한 평가가 어려웠다. 혈액 검사에서는 백혈 구가 14,900/mm3 (중성구 91.3%)으로 증가되고, 저나트륨혈증(122 mEq/L, 기준치: 135-148 mEq/L)을 보인 것 외에는 모두 정상이었다. 뇌 MRI상 확산강조영상(diffusion weighted image)에서 우측 등쪽 교뇌 와 좌측 중뇌에 고신호 강도를 보이는 병변이 보이면서 겉보기확산계 수지도(apparent diffusion coefficient map, ADC map)에서는 저신호를 보여 뇌경색에 합당하였으며, T1조영증강영상(enhanced image)에서 중뇌의 배쪽면과 대뇌반구의 수막에 현저한 조영증강이 관찰되었다 (Fig. 2). 뇌 MRA는 동맥경화성 변화로 추정되는 혈관의 비균일성(ir- regularity)은 보였지만 협착이나 동맥류의 소견은 없었다. 뇌척수액 검사상 개방 압력은 150 mm H2O로 정상이었지만, 백혈구 90/mm3 (림프구 70%), 당 31 mg/dL (혈청 당: 102 mg/dL), 단백질 160 mg/dL (기 준치 15-50 mg/dL)로 수막염에 합당한 소견을 보였다. 그람염색(Gram stain)과 세균배양은 음성이었고, 결핵균 검사에서도 항산균염색 (AFB stain), 항산균배양, 결핵균 중합효소연쇄반응(polymerase chain reaction, PCR)이 모두 음성이었다. 크립토코쿠스 항원은 양성이었지 만 배양검사에서 균이 동정되지는 않았다. 크립토코쿠스 수막염으로 진단하고 암포테리신 B 1 mg/kg/day와 flucytosine 100 mg/kg/day를 투 여하였다. 2주일간 암포테리신과 flucytosine을 투여하였으나 발열이 간헐적으로 있었으며, 의식도 혼미한 상태로 지속되어 추가적인 검사 를 시행하지 못하였다. 환자는 핵간안근마비와 눈돌림신경마비가 호 전되지 않은 상태에서 타 병원으로 전원하였다.
고 찰
크립토코쿠스증은 진균감염의 하나로 수막염을 발생시켜 안구증 상(ocular symptom)을 일으킬 수 있다. 크립토코쿠스 수막염은 뇌척 수액 검사로 진단할 수 있는데, 진단받은 환자의 97%에서 세포 수의 증가, 90%에서 단백질의 상승, 55%에서 당 수치의 감소, 64%에서 뇌압 의 상승을 보일 수 있다. 또한 가장 의미 있는 소견은 크립토코쿠스 항 원을 확인하는 것으로 민감도가 93-100%, 특이도가 93-98%로 높아 전통적인 India ink 검사보다 우수하다고 알려져 있다.4 안구증상은 유두부종, 시신경위축, 시신경병이 잘 나타나며 3, 4, 6번 뇌신경과 관 련된 안근마비도 발생할 수 있다.3 또한, 안구증상은 아니지만 7, 8번 뇌신경 손상에 의한 안면마비, 청력이상에 대한 보고도 있다.3 국내에 서는 INO를 보인 크립토코쿠스 수막염이 2예가 보고되었고, 눈돌림
A B
C D
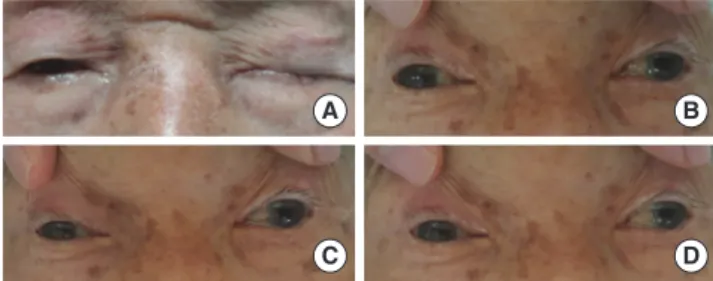
Fig. 1. Internuclear ophthalmoplegia in right eye and oculomotor nerve palsy in left eye. (A) The patient cannot elevate left eyelid voluntarily. (B) On attempted gaze to the right, the left eye dose not adduct. (C) During straight ahead gaze, the patient shows exotropia of both eyes and mydriasis of left pupil. (D) On at- tempted gaze to the left, the right eye dose not adduct completely.
A
B
C Fig. 2. (A) Diffusion-weighted MRI and apparent diffusion coefficient (ADC) map reveal acute infarction involving left midbrain (arrows). (B) Diffusion- weighted MRI and ADC map reveal acute infarction involving right dorsal pons (arrows). (C) T1-enhanced MRIs reveal prominent leptomeningeal enhancement of ventral midbrain and cerebral hemisphere (arrows).
Do Y, et al. • Oculomotor Nerve Palsy and INO in Cryptococcal Meningitis
Clin Neuroophthalmol 5(2):98-100, December 2015 100 http://neuro-ophthalmology.co.kr
신경마비에 대한 보고는 없었다.5,6 국외의 경우에도 INO 1예와 눈돌 림신경마비 4예만이 보고되었다.3 크립토코쿠스 수막염에서 발생하 는 안구증상은 뇌신경에 의한 직접적인 침범이나 감염에 의한 염증반 응에 의해 발생하거나, 증가된 뇌압에 의해 신경이 압박되어 나타난 다. 뇌압의 상승은 크립토코쿠스 자체가 거미막하공간에서 뇌척수액 이 지나는 길을 막거나 과도하게 침착된 크립토코쿠스의 부산물이 삼투압을 변화시켜 발생한다.3,7
크립토코쿠스 수막염에서 뇌경색이 생길 수도 있는데, 발생하는 빈 도에 대해서는 연구마다 차이가 있어 한 연구에서는 4%로 그리 높지 않은 빈도를 보이나 다른 연구에서는 39%로 높게 보고된다.8 수막염 과 관련된 뇌경색은 주로 기저핵(basal ganglia), 속섬유막(internal cap- sule), 그리고 시상(thalamus)에서 발생하며, 중뇌동맥 같은 큰 혈관이 나 뇌간을 침범하는 경우는 드물다.9 수막염에서 뇌경색이 발생하는 기전은 첫째, 뇌기저부 삼출물(exudate)이 뇌혈관을 둘러싸면서 혈관 을 직접 압박하여 혈관연축과 혈전이 생기는 것이다. 둘째, 수막에서 생긴 염증성 삼출물이 혈관벽을 침범하여 괴사성 혈관염을 일으키 고, 이로 인해 혈전이 생성되며, 또한 혈관의 경련이나 수축이 발생하 여 뇌경색을 일으키는 것이다. 마지막으로 혈관에 인접한 뇌실이 확장 되어 기능이 떨어진 혈관을 압박하고 순환에 장애를 일으켜 뇌경색 이 발생하는 것이다.8,9
저자들의 경우에는 뇌척수액 검사에서 개방 압력이 150 mm H2O 로 정상이어서 뇌압의 증가에 의한 안근마비의 가능성은 낮았고, MRI에서 뇌경색에 합당한 소견을 보였으므로, 수막염에 의한 이차적 인 뇌경색 때문에 INO와 눈돌림신경마비가 발생한 것으로 생각한다.
INO는 안쪽세로다발(medial longitudinal fasciculus, MLF)의 손상에 의해, 좌측 눈돌림신경 마비는 눈돌림신경다발(oculomotor fascicle) 의 손상에 의해 생긴 것으로 보이며, MRI에서 보이는 병변과 일부 일 치한다. 하지만 환자의 의식이 혼미하여 수직 및 회선안구운동, 눈모 음, 안구머리반사 등에 대한 세밀한 안신경학적 검사를 시행하지 못 하였기 때문에 진단에 제한점이 있다 정위에서 양안의 외사시(exo- tropia)가 관찰되었기 때문에 양안의 INO도 생각해 볼 수 있으나 좌안 에서 관찰되는 외전안진이 우측을 볼 때 우안에서는 전혀 보이지 않 았고, 좌안은 외하방으로 편위되어 거의 움직임이 없는 상태로 완전 한 눈꺼풀처짐과 동공의 확장을 동반하여 우측의 INO와 좌측의 눈 돌림신경마비가 더 합당한 소견으로 생각하였다. 또한 MRI에서 보이
는 우측 교뇌의 병변도 MLF의 위치보다는 앞쪽에 위치한 것으로 볼 수 있으며, 좌측 중뇌의 병변도 비교적 눈돌림신경핵의 상방쪽에 위 치하고 있어 안구증상과의 일치에 제한이 있을 수 있다. 우측 교뇌의 병변은 MRI에서 보이는 고신호강도가 뚜렷하지 않은 상태로 MLF가 있는 등쪽까지 병변이 있을 것으로 추정되며, 좌측 중뇌병변도 하방 까지 MRI에서 보이지 않은 병변이 있을 가능성이 있을 수 있다. 또한 중뇌에 인접한 수막에 조영증강이 된 것으로 보아 수막의 염증이 눈 돌림신경의 마비에 영향을 주었을 수도 있다
교뇌와 중뇌에 보인 뇌경색은 뇌기저동맥의 정중옆분지(paramedi- an)의 지배 영역에 발생하였고 중뇌 배부의 현저한 조영증강을 볼 때, 위에서 설명한 기전 중 첫 번째나 두 번째 기전에 의해 발생한 것으로 추정된다.
크립토코쿠스 수막염에서도 드물지만 뇌간경색이 발생할 수 있으 며 침범되는 뇌간의 구조물에 따라 다양한 안구증상이 나타날 수 있 을 것이다.
REFERENCES
1. Makadzange AT, McHugh G. New approaches to the diagnosis and treat- ment of cryptococcal meningitis. Semin Neurol 2014;34:47-60.
2. Espino Barros Palau A, Morgan ML, Foroozan R, Lee AG. Neuro-oph- thalmic presentations and treatment of cryptococcal meningitis-related increased intracranial pressure. Can J Ophthalmol 2014;49:473-477.
3. Mohan S, Ahmed SI, Alao OA, Schliep TC. A case of AIDS associated cryptococcal meningitis with multiple cranial nerve neuropathies. Clin Neurol Neurosurg 2006;108:610-613.
4. Makadzange AT, Mchugh G. New approaches to the diagnosis and treat- ment of cryptococcal meningitis. Semin Neurol 2014;34:47-60.
5. Yi JY, Kim JI, Kim KS, Kang MC, Lee CM, Yang DW, et al. A Case of CNS cryptococcosis with Internuclear Ophthalmoplegia. J Korean Neu- rol Assoc 1997;15:1195-1198.
6. Kim SH, Kwon OY, Son SN, Kim JE, Choi JH, Park KJ, et al. A Case of Cryptococcal Meningitis with Bilateral Internuclear Ophthalmoplegia and Ptosis. J Korean Neurol Assoc 2005;23:557-560.
7. Liyanage DS, Pathberiya LP, Gooneratne IK, Caldera MH, Perera PW, Gamage R. Cryptococcal meningitis presenting with bilateral complete ophthalmoplegia: a case report. BMC Res Notes 2014;7:328.
8. Lan SH, Chang WN, Lu CH, Lui CC, Chang HW. Cerebral infarction in chronic meningitis: a comparison of tuberculous meningitis and crypto- coccal meningitis. QJM 2001;94:247-253.
9. Rosario M, Song SX, McCullough LD. An unusual case of stroke. Neu- rologist 2012;18:229-232.