www.jkfas.org http://dx.doi.org/10.14193/jkfas.2015.19.1.11
서 론
종골 골절은 족부 골절 중 약 60%를 차지하는 빈도 높은 골절이 다.
1)
종골 골절은 관절 내 골절과 관절 외 골절로 분류할 수 있으 며 관절 내 골절이 75%를 차지하고 이에 따른 관절면 불일치에 의Received October 24, 2014 Revised January 8, 2015 Accepted February 9, 2015 Corresponding Author: Chan Kang
Department of Orthopedic Surgery, Chungnam National University Hospital, 282 Munhwa-ro, Jung-gu, Daejeon 301-721, Korea
Tel: 82-42-338-2438, Fax: 82-42-338-2482, E-mail: [email protected] Financial support: None.
Conflict of interest: None.
Original Article
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
CCby-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright 2015 Korean Foot and Ankle Society. All rights reserved. ⓒ
Purpose: To report the radiographic and clinical results of 6.5 mm cancellous full threaded buttress screw or Steinmann pin fixation to
maintain a reduction of calcaneal posterior facet depression fracture.Materials and Methods: From June 2009 to June 2012, 50 consecutive cases with calcaneal joint depression fracture that underwent
open reduction and screw or pin fixation were enrolled in this study. A 6.5 mm cancellous full threaded screw was inserted from the posteroinferior aspect of the calcaneal tuberosity to the posterior facet (group A) or Steinman pin was inserted from the posterosupe- rior aspect of the calcaneal tuberosity to the calcaneocuboidal joint (group B). Both preoperative and postoperative Bohler and Gissane angles were measured radiographically, and American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot scale on the final follow-up were assessed.Results: The mean age of patients was 44.1 years, and the mean follow-up period was 27.2 months. According to the Sanders classifica-
tion, 28 cases were type II and 22 cases were type III. In Sanders type II, Bohler and Gissane angles improved significantly from 10.1o
and 126.2o
preoperatively to 27.2o
and 117.1o
, respectively, in the immediate postoperative radiograph, and at the final follow-up, 26.6o
and 118.6o
, respectively. In Sanders type III, Bohler and Gissane angles improved significantly from 5.0o
and 129.8o
to 29.9o
and 119.3o
, respectively, in the immediate postoperative radiograph, and 26.9o
and 120.2o
at the final follow-up. All cases achieved bony union, and the average period until complete union was 13.3 weeks. AOFAS ankle-hindfoot scale was 82.6 in Sanders type II and 77.3 in Sanders type III at the final follow-up.Conclusion: A 6.5 mm cancellous full threaded buttress screw or Steinman pin fixation is a noninvasive treatment method with a merit
of being able to maintain the bearing capacity of the posterior facet comparable to plate fixation.Key Words: Calcaneus, Intra-articular fractures, 6.5 mm cancellous screw, Steinmann pin
종골의 관절 함몰 골절에서 6.5 mm 해면골 나사와 Steinmann 핀을 이용한 치료의 유용성
이기수*, 강 찬, 황득수, 노창균, 이기영
충남대학교 의과대학 정형외과학교실, *건양대학교 의과대학 정형외과학교실
Usefulness of Treatment with 6.5 mm Cancellous Screw and Steinmann Pin Fixation for Calcaneal Joint Depression Fracture
Gi-Soo Lee*, Chan Kang, Deuk-Soo Hwang, Chang-Kyun Noh, Gi-Young Lee
Department of Orthopedic Surgery, Chungnam National University School of Medicine,
*Department of Orthopedic Surgery, Konyang University College of Medicine, Daejeon, Korea
총 47명 중 남자가 32명(68.1%), 여자가 15명(31.9%)이었으며, 연령 분포는 20대 8명, 30대 10명, 40대 9명, 50대 15명, 60대 5명으 로 평균 연령은 44.1세였다. 이들 중 23명(48.9%)에서는 우측, 21 명(44.7%)에서는 좌측, 그리고 양쪽 모두의 골절은 3명(6.4%)에서 일어났다(Table 1). 종골 관절 함몰 골절의 관혈적 정복 후 이를 유 지하기 위하여 종골 융기 후하방에서 종골 후과 방향으로 6.5 mm 해면골 전산나사못을 이용한 버팀(buttress) 고정한 방법(A군) 또 는 종골 융기 후상방에서 종입방 관절 방향으로 Steinmann 핀을 이용한 버팀 고정한 방법(B군)을 시행하였으며, 종골 후방 관절면 의 직하방 위치에서 횡 방향으로 금속핀(K-wire) 또는 4.0 mm 유 관 나사못(cannulated screw) 고정을 하기도 하였다. 비관혈적 수 술 방법을 이용한 경우는 대상에서 제외하였다. 종골 관절 내 골 절 분류상 Sanders type II형은 28예, Sanders type III형은 22예였 다. A군은 Sanders type II형이 17예, Sanders type III형이 15예였으 며 B군은 Sanders type II형이 11예, Sanders type III형이 7예였다.
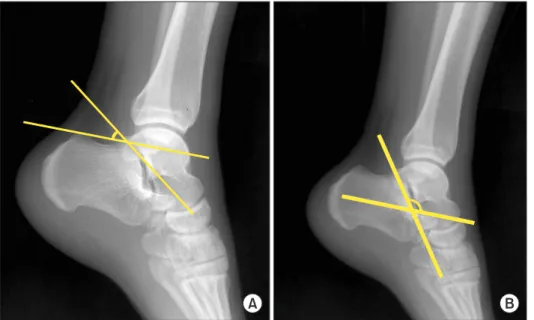
수술 전 정확한 골절 양상의 파악을 위해 환자의 족부 전후면, 측 면, 사면, 축상면, Broden 영상 촬영 및 족부 삼차원 컴퓨터단층촬 영(three-dimensional computed tomography, 3D CT)을 시행하였 다. 내고정 수술 후와 금속 제거술 후 최종 추시에서 시행한 단순 방사선 측면 사진으로 Bohler 각과 Gissane 각을 측정하였다(Fig.
1). 그리고 Broden 영상으로 후방 관절면의 해부학적 정복 정도를 평가하였다. 모든 계측치는 두 명의 정형외과 전문의(G.S.L., C.K.) 에 의해 2회 반복 측정한 뒤 평균치를 구하였다. 또한, 추시상에서 Broden 영상을 촬영하여 후방 관절면의 유지 상태를 확인하였다.
수술 방법으로는 환자를 측와위로 눕혀 변형된 Ollier 도달법을 사용하였다. 피부 절개는 외과 첨부 2.5 cm 상방 높이의 외과와 아 킬레스건 중간 지점에서 시작하여 비스듬하게 내려와 외과 첨부 1 cm 하방을 지나 족근동 부위를 거쳐 종입방 관절 부위까지 시 한 외상성 관절염 등이 발생하기 쉽다.
2-4)
관절 함몰형 골절에 대한 수술적 치료의 경우 광범위 외측 도달법을 통한 금속판 고정술 이 널리 이용되고 있으나, 광범위 박리로 인한 피판 괴사, 감염이 발생하기 쉽고 비복 신경의 외측 종골 분지 손상으로 인한 작열통 이나 감각이상, 금속판 자극, 불유합 등의 합병증을 일으킬 수 있 다.
5,6)
이에 저자들은 금속판 이외의 6.5 mm 해면골 전산나사못 또 는 Steinmann 핀 등을 이용하여 수술하였고, 이에 대한 방사선학 적 및 임상적 결과를 분석해 보고자 하였다.대상 및 방법
충남대학교병원에서 2009년 6월부터 2012년 6월까지 Sanders type II 또는 III형의 종골 관절 함몰 골절로 진단받고 관혈적 정복 후 6.5 mm 해면골 전산나사못 또는 Steinmann 핀으로 내고정술을 받은 뒤 최소 24개월 이상 추시 관찰이 가능하였던 47명, 50예를 대상으로 하였으며, 임상적 및 방사선학적으로 후향적 분석을 하 였다.
Table 1. Demographic Data of Patients
Variable Group A Group B p-value
Number of patients Mean age (yr) Gender (male) Affected foot (right) Smoker
32 44.5 (21∼63)
22 14 10
18 43.5 (24∼61)
10 9 4
0.593 0.869 0.612 0.245 Values are presented as number or mean (range).
Group A: a 6.5 mm cancellous full threaded screw inserted from the posteroinferior aspect of the calcaneal tuberosity to the posterior facet;
Group B: Steinman pin inserted from the posterosuperior aspect of the calcaneal tuberosity to the calcaneocuboidal joint.
A B
Figure 1. Measurement of Bohler and
Gissane angles. (A) Bohler angle is mea-
sured by the intersection of a line drawn
from most cephalic point on tuberosity to
highest point of posterior facet with a line
from highest point of posterior facet to
most cephalic part of posterior process of
calcaneus. (B) Gissane angle is measured
by the intersection of a line drawn from
the highest point of the posterior articular
facet to the highest point of the posterior
tuberosity and a line from the former to
the highest point on the anterior articular
facet.
www.jkfas.org
거나 또는 종골 융기 후상방에서 종입방 관절 방향으로 Steinmann 핀을 이용하여 버팀 고정하였다(Fig. 3). 후방 관절면의 정복 상태 를 판단하기 위해 수술 중 영상 증폭기(image intensifier)를 이용하 여 Broden 영상을 확인하였으며, 정복된 관절면의 높이 차이를 1 mm 이내로 허용하였다.수술 후 치료 방법은 초기 4주간은 단하지 석고 붕대 고정 및 비 체중부하 보행을 하였으며, 이후 석고 붕대를 제거하고 전족부 체 중부하 보행 및 발목 관절운동을 시작하였다. 8주경에는 후족부 접촉 체중부하 보행, 12주 이후부터는 전 체중부하 보행을 시작하 며 추적관찰하였다. 금속 제거술은 고정술 후 3개월이 지난 뒤에 좌골 신경 차단을 이용한 마취하에 시행하였다. 치료 결과에 대한 임상적 평가는 최종 추시에서 환자의 만족도, 관절운동 범위의 제 한 여부, 보행 능력, 족부 통증 여부 등을 종합한 American Ortho- paedic Foot and Ankle Society (AOFAS) ankle-hindfoot scale을 조사하였다. 통계적 분석은 IBM SPSS Statistics version 21.0 (IBM Co., Armonk, NY, USA)을 사용하였으며, 유의 수준은 p<0.05로 하였다. 또한 본 연구는 충남대학교병원 임상연구윤리위원회(in- stitutional review board)의 승인을 받았다.
결 과
골 유합 기준은 추시 방사선 사진에서 가골 형성이 보이고 골절 부위에 압통이 사라지는 시점을 기준으로 하여 평균 13.3주였으 며, 모든 환자에서 골 유합이 이루어졌다. 수상 후 수술까지 걸린 시간은 평균 5.7일이었다. 수술 전후 및 최종 추시에서 Bohler 각과 Gissane 각 및 AOFAS hindfoot scale은 다음과 같다. Sanders type II형에서 수술 전 평균 Bohler 각과 Gissane 각은 10.1
o
및 126.2o
였 고, Sanders type III형에서는 5.0o
및 129.8o
였다. Sanders type II형 에서 수술 후 평균 Bohler 각과 Gissane 각은 27.2o
, 117.1o
였고, 최 행하였다(Fig. 2). 피부 절개 후 비골 지지대 및 종비 인대를 가르고, 비복 신경 및 비골 인대를 보호하며 피판을 젖힌 후 비골과 종 골 후하방부에 금속핀을 횡 방향으로 삽입한 후 견인 장치를 이용 하여 비골과 종골 사이를 넓혀주어 종입방 및 후방 관절과 후방 결 절을 모두 노출시켰다. 이후 종골 후과 관절면의 함몰된 골 절편을 골막 분리기(periosteum elevator)를 이용해 들어올려 Bohler 각과 Gissane 각을 교정하고, 후방 관절면의 정복 상태를 육안과 프로브 (probe)를 이용하여 확인하였다. 필요한 경우 금속핀(K-wire) 또는 4.0 mm 유관 나사못을 이용하여 내측 골 절편과 외측 골 절편을 내고정한 후, 이를 유지하기 위하여 종골 융기 후하방에서 종골 후 과 방향으로 6.5 mm 해면골 전산나사못을 이용하여 버팀 고정하
Figure 2. Beginning from 2.5 cm superior to lateral malleolus tip, which is the midpoint between malleolus and Achilles tendon, the incision continues obliquely and distally toward 1 cm below the lateral malleo- lus tip, sinus tarsi, and dorsolateral aspect of the talonavicular joint.
Figure 3. Operative method. (A) A 6.5 mm cancellous buttress screw should be inserted from posteroinferior aspect of calcaneal tuberosity to the posterior facet (arrow). (B) Steinmann pins should be inserted from posterosuperior aspect of calcaneal tuberosity to the calcaneocuboid joint (arrow).
A B
종 추시에서는 26.6
o
, 118.6o
, 그리고 AOFAS ankle-hindfoot scale 은 82.6점이었다. Sanders type III형의 수술 후 평균 Bohler 각과 Gissane 각은 29.9o
, 119.3o
였고, 최종 추시에서는 26.9o
, 120.2o
, 그 리고 AOFAS ankle-hindfoot scale은 77.3점이었다. Sanders type II, III형 모두에서 Bohler 각과 Gissane 각이 수술 직후 유의한 호 전을 보였으며(p<0.05), 최종 추시 시 수술 직후와 비교하여 잘 유 지되었다(p>0.05; Table 2, 3). 또한, 종골 융기 후하방에서 종골 후과 방향으로 6.5 mm 해면골 전산나사못을 이용한 버팀 고정(A 군)과 종골 융기 후상방에서 종입방 관절 방향으로 Steinmann 핀 을 이용한 버팀 고정(B군)한 수술 방법에 대한 공변량 분석 결과 에서 통계적으로 유의할 만한 차이를 보여주지 못하였다(p>0.05;Table 6. Comparison of AOFAS Ankle-Hindfoot Scale between Group A and B in Sanders Classification Type II and III Calcaneus Fractures
Type Group A (n=32) Group B (n=18) p-value Type II (n=28)
Type III (n=22)
82.5±4.6 76.2±3.7
82.7±5.8 79.3±4.2
0.960 0.796 Values are presented as mean±standard deviation.
Group A: a 6.5 mm cancellous full threaded screw inserted from the posteroinferior aspect of the calcaneal tuberosity to the posterior facet;
Group B: Steinman pin inserted from the posterosuperior aspect of the calcaneal tuberosity to the calcaneocuboidal joint.
AOFAS: American Orthopaedic Foot and Ankle Society.
Table 2. Comparison between Preoperative and Postoperative Bohler and Gissane Angles in Sanders Type II Calcaneus Fractures (n=28)
Angle Preoperative Postoperative Final follow-up p-value* p-value
†Bohler angle Gissane angle
10.1
o±4.4
o126.2
o±5.5
o27.2
o±2.2
o117.1
o±3.2
o26.6
o±2.5
o118.6
o±4.4
o0.009 0.011
0.845 0.385 Values are presented as mean±standard deviation.
*Comparison between preoperative and postoperative Bohler and Gissane angles.
†
Comparison between postoperative and final follow-up Bohler and Gissane angles.
Table 3. Comparison between Preoperative and Postoperative Bohler and Gissane Angles in Sanders Type III Calcaneus Fractures (n=22)
Angle Preoperative Postoperative Final follow-up p-value* p-value
†Bohler angle Gissane angle
5.0
o±3.4
o129.8
o±9.5
o29.9
o±3.1
o119.3
o±8.7
o26.9
o±3.0
o120.2
o±12.0
o0.001 0.004
0.557 0.985 Values are presented as mean±standard deviation.
*Comparison between preoperative and postoperative Bohler and Gissane angles.
†
Comparison between postoperative and final follow-up Bohler and Gissane angles.
Table 4. Comparison between Postoperative and Final Follow-up Bohler Angles for Group A and B in Sanders Classification Type II and III Calcaneus Fractures
Type Group A (n=32) Group B (n=18)
Postoperative Final follow-up Postoperative Final follow-up p-value
Type II (n=28) Type III (n=22)
28.7
o±2.5
o32.9
o±4.7
o27.8
o±2.2
o28.7
o±3.5
o24.5
o±2.1
o24.7
o±3.9
o24.4
o±1.8
o23.7
o±7.5
o0.727 0.825 Values are presented as mean±standard deviation.
Group A: a 6.5 mm cancellous full threaded screw inserted from the posteroinferior aspect of the calcaneal tuberosity to the posterior facet; Group B:
Steinman pin inserted from the posterosuperior aspect of the calcaneal tuberosity to the calcaneocuboidal joint.
Table 5. Comparison between Postoperative and Final Follow-up Gissane Angle of Group A and B in Sanders Classification Type II and III Calcaneus Fractures
Type Group A (n=32) Group B (n=18)
Postoperative Final follow-up Postoperative Final follow-up p-value
Type II (n=28) Type III (n=22)
117.2
o±1.9
o118.9
o±2.0
o118.9
o±2.1
o120.7
o±2.5
o116.8
o±2.0
o120.0
o±6.0
o118.1
o±1.8
o119.3
o±5.8
o0.862 0.740 Values are presented as mean±standard deviation.
Group A: a 6.5 mm cancellous full threaded screw inserted from the posteroinferior aspect of the calcaneal tuberosity to the posterior facet; Group B:
Steinman pin inserted from the posterosuperior aspect of the calcaneal tuberosity to the calcaneocuboidal joint.
www.jkfas.org
는 보이지 않으므로 내측 도달법이 유용하며 staple 또는 나사못으 로 내고정하여 82%에서 좋은 결과를 얻었다고 보고하였으나, Ross 와 Sowerby14)
는 내측 도달법은 신경혈관의 손상 위험이 있고 거골 하 관절면을 직접 볼 수 없으며 골피질이 얇아 조기 운동을 허용할 만큼 견고한 내고정을 시행할 수 없고 절개 부위 연장에 제한 등의 단점을 지적하였다. Levine과 Helfet21)
와 Schepers 등22)
은 최소 절 개를 이용하여도 관절면의 정복이 가능하고 양호한 결과를 보였다 고 하였으며 합병증도 최소화할 수 있다고 하였다. 이렇듯 관절 내 종골 골절은 치료에 있어 다양한 수술적 도달법 및 정복 방법이 소 개되고 있으나 치료 방법에 따른 결과 보고는 항상 일치하지는 않 았다. 다만, 해부학적 정복 및 견고한 고정과 관절의 조기 운동이 좋은 결과의 가능성을 높인다는 원칙과 비수술적 방법으로는 결코 관절 내의 전위된 골편이 정복될 수 없어, 정상적인 기능으로 회복 될 가능성이 희박하다는 점에서 적극적인 수술적 치료가 선호되고 있다.최근 가장 많이 사용되고 있는 외측 도달법에 의한 관혈적 정복 및 금속판 고정술은 단단한 고정력을 가져 방사선적 및 임상적으 로 좋은 결과가 보고되고 있으나, 비골신경 손상 등의 신경 손상, 상처 벌어짐, 피부 괴사, 연부조직에 긴장도 증가 등의 금속판 자 극, 금속 제거 시 광범위 절개가 필요함 등의 단점을 지니고 있다.
이에 저자들은 다른 수술 방법에 대한 가능성을 생각해 보았다.
Widen
23)
이 거골하 관절의 정확한 정복이 운동성의 유지에 가장 확 실하다고 하였듯이, 저자들도 수술 전 3D CT 등을 이용한 관절 내 골절 양상의 정확한 이해를 통해 수술 시 가능한 한 최대한의 해부 학적 정복 및 견고한 내고정을 얻고자 하였다. 종골 후과 함몰 관 절 내 골절에서 정복에 필요한 최소한의 관혈적 외측 도달법(변형 된 Ollier 도달법) 후 후방 관절면의 골절 상태를 육안으로 확인하 여 관절면을 불일치 정도가 가능한 한 1 mm 이내가 되도록 정복한 후, 금속핀(K-wire) 또는 4.0 mm 유관 나사못를 이용하여 종골의 횡 방향으로 고정하였으며, 정복 유지를 위하여 종골 융기 후하방 에서 종골 후과 방향으로 6.5 mm 해면골 전산나사못을 이용한 버 팀 고정한 방법(A군)과 종골 융기 후상방에서 종입방 관절 방향으 로 Steinmann 핀을 이용한 버팀 고정한 방법(B군)에 대하여 방사 선학적 및 임상적 결과를 추시하여 결과를 비교 분석하여 보았다.저자들은 A군과 B군의 수술 방법을 후방 관절면의 골절 형태 및 골절편 크기에 따라 선택하였으며, 관절면의 골절편이 6.5 mm 해 면 전산나사못을 유지할 정도로 크기가 충분하면 전자를 선택하였 고 골절편의 크기가 해면 전산 나사못을 버틸 정도로 충분하지 못 하거나 해면 전산나사못이 삽입될 부위에 골절선이 있는 경우에는 후자를 선택하였다.
수술 직후와 최종 추시에서 Bohler 각과 Gissane 각을 비교한 결 과 Sanders type II형에서 Bohler 각은 2.2% 감소 및 Gissane 각은 1.3% 증가하였으며, Sanders type III형에서 Bohler 각은 10.1% 감 소 및 Gissane 각은 0.8% 증가하였다. AOFAS ankle-hindfoot scale Table 4, 5). AOFAS ankle-hindfoot scale 역시 양호한 결과를 보였
다(p>0.05; Table 6). 두 군 모두에서 Broden 영상 촬영을 이용하 여 수술 후 종골 후방 관절면의 해부학적 정복이 1 mm 이내로 된 것을 확인하였으며, 추시상에서 정복의 유의한 손실이 발생한 예 는 없었다.
모든 예에서 불유합이나 나사못의 해리 또는 파열, 창상의 감염 은 보이지 않았으며 비복신경의 손상 등의 합병증은 발생하지 않 았다. 또한, 최종 추시까지 종골의 높이 감소, 폭의 증가, 그리고 후 족부 내반 등의 부정 유합 발생으로 인하여 비골 충돌 증후군, 경 골-거골간 충돌, 그리고 외상 후 관절염 증상 발생으로 불편감을 크게 호소하는 환자는 없었다.
고 찰
종골은 해부학적 특성상 내부의 해면골을 얇은 피질골이 싸고 있는 구조로 되어 있어 축성 압박력이 가해졌을 때 함몰 형태로 손 상받기 쉬우며,
7,8)
거골과 관절을 이루어 후족부의 운동을 담당하 고 있어 관절면 손상 시 많은 문제점이 발생할 수 있다. 이러한 이 유로 종골 골절의 치료의 목적은 첫째, 종골의 높이와 길이 그리고 넓이를 회복하고 둘째, 모든 관절면 특히 후방 관절면을 해부학적 으로 정복하여 외상 후 관절염의 발생을 최소화하며, 셋째, 조기에 관절운동을 회복하며 안정된 골 유합을 이루는 것이다.9-12)
종골 골절의 치료와 관련하여 Sanders 등
13)
과 Ross와 Sowerby14)
가 관혈적 정복술 및 금속 내고정술에 대한 연구를 발표한 이래, 현재는 관절 내 종골 골절의 치료로써 관혈적 정복술 및 금속 내고 정술이 널리 사용되고 있다. Thordarson과 Krieger15)
의 전위된 관 절 내 종골 골절을 대상으로 한 전향적 무작위 대조 연구에서는 수 술적 치료를 한 경우에서 보존적 치료를 한 경우보다 수술 후 1년 이상 경과에서 보다 좋은 기능적 평가 결과를 보고하였다. 이후 최 근의 연구들에서도 Sanders type II, III형의 종골 골절에서는 수술 적 치료가 보존적 치료를 했을 경우보다 더욱 만족스러운 결과들 을 보고하고 있다.16,17)
종골 골절에서는 수술적 도달법으로는 외측 도달법, 내측 도달 법, 양측 도달법, 그리고 거골하 관절 고정술에 이용되는 후방 도 달법 등이 있다. 1948년 Palmer
18)
가 외측 도달법을 이용한 관혈적 정복 후 내고정술을 시행하여 90%에서 좋은 결과를 얻었다고 보 고하였으며, 이후 Maxfield와 McDermott19)
및 Ross와 Sowerby14)
는 70%∼80% 이상에서 좋은 결과를 얻었다고 보고하였다. 이는 광범 위한 절개로 거골하 관절과 종입방 관절을 노출 및 도달하여 정복 할 수 있고, 돌출된 외측 골편의 감압으로 비복신경과 비골건을 감 압할 수 있으며, 내고정하기에 좋고 신경혈관 손상의 위험이 없는 등의 장점들이 있어 외측 도달법은 많은 수술의에게 일차적 선택 방 법으로 사용되고 있다. 반면, McReynold20)
는 종골 골절 시의 2개의 주골편 중 제거돌기 골편의 정복이 중요함을 들며, 이는 외측에서41 Tscherne H, Schatzker J. Major fractures of the pilon, the ta- lus and the calcaneus: current concepts of treatment1 Berlin:
Springer-Verlag; 19931 p1153-741
51 Abidi NA, Dhawan S, Gruen GS, Vogt MT, Conti SF. Wound- healing risk factors after open reduction and internal fixation of calcaneal fractures1 Foot Ankle Int1 1998;19:856-611
61 Benirschke SK, Sangeorzan BJ. Extensive intraarticular fractures of the foot1 Surgical management of calcaneal fractures1 Clin Orthop Relat Res1 1993;(292):128-341
71 Barei DP, Bellabarba C, Sangeorzan BJ, Benirschke SK. Fractures of the calcaneus1 Orthop Clin North Am1 2002;33:263-851 81 Stephenson JR. Surgical treatment of displaced intraarticular
fractures of the calcaneus1 A combined lateral and medial ap- proach1 Clin Orthop Relat Res1 1993;(290):68-751
91 Essex-Lopresti P. The mechanism, reduction technique, and results in fractures of the os calcis1 Br J Surg1 1952;39:395-4191 101 Letournel E. Open reduction and internal fixation of calcaneus
fractures1 In: Spiegel PG, editor1 Topics in orthopedic trauma1 1st ed1 Baltimore: University Parkpress; 19841 p1173-921 111 Letournel E. Open treatment of acute calcaneal fractures1 Clin
Orthop Relat Res1 1993;(290):60-71
121 Zwipp H, Tscherne H, Thermann H, Weber T. Osteosynthesis of displaced intraarticular fractures of the calcaneus1 Results in 123 cases1 Clin Orthop Relat Res1 1993;(290):76-861
131 Sanders R, Fortin P, DiPasquale T, Walling A. Operative treat- ment in 120 displaced intraarticular calcaneal fractures1 Results using a prognostic computed tomography scan classification1 Clin Orthop Relat Res1 1993;(290):87-951
141 Ross SD, Sowerby MR. The operative treatment of fractures of the os calcis1 Clin Orthop Relat Res1 1985;(199):132-431
151 Thordarson DB, Krieger LE. Operative vs1 nonoperative treat- ment of intra-articular fractures of the calcaneus: a prospective randomized trial1 Foot Ankle Int1 1996;17:2-91
161 Basile A. Operative versus nonoperative treatment of displaced intra-articular calcaneal fractures in elderly patients1 J Foot Ankle Surg1 2010;49:25-321
171 Robb CA, Deans V, Iqbal MJ, Cooper JP. Comparison of non-op- erative and surgical treatment of displaced calcaneal fractures1 The Foot1 2007;17:169-731
181 Palmer I. The mechanism and treatment of fractures of the cal- caneus; open reduction with the use of cancellous grafts1 J Bone Joint Surg Am1 1948;30:2-81
191 Maxfield JE, McDermott FJ. Experiences with the Palmer open reduction of fractures of the calcaneus1 J Bone Joint Surg Am1 1955;37:99-1061
201 McReynold IS. The case on operative treatment of the os calcis1 In: Leach RE, Hoaglund FT, Riseborough EJ, editors1 Controver- sies in orthopedic surgery1 Philadelphia: Sanders; 19821 p1232- 541
211 Levine DS, Helfet DL. An introduction to the minimally invasive osteosynthesis of intra-articular calcaneal fractures1 Injury1 2001;32 Suppl 1:SA51-41
221 Schepers T, Schipper IB, Vogels LM, Ginai AZ, Mulder PG, Heetveld MJ, et al. Percutaneous treatment of displaced intra- articular calcaneal fractures1 J Orthop Sci1 2007;12:22-71 231 Widen A. Fractures of the calcaneus: a clinical study with special
은 Sanders type II형에서는 82.6점, Sanders type III형에서는 77.3점이었다. Lee 등
24)
은 광범위 외측 도달법 후 금속판을 이용한 결 과 Sanders type II형에서는 수술 후 평균 Bohler 각과 Gissane 각은 27.7o
, 121.4o
, 최종 추시에는 27.2o
, 120.7o
였으며, Sanders type III 형의 수술 후 평균 Bohler 각과 Gissane 각은 26.5o
, 121.8o
, 최종 추 시에는 26.3o
, 121.1o
였다고 보고하였다. 위의 결과에서 보듯이 본 연구의 결과와 비교하여 유의 있는 차이는 없다고 생각되며, 이 밖 에 다른 연구 결과 보고들과 비교하여도 양호한 결과를 보였음을 알 수 있었다.24-26)
일반적으로 최소 절개 외측 도달법을 이용한 수 술법은 Sanders type II형이나 일부 Sanders type III형에서 사용 가 능하다 여겨져 왔으나, 저자들은 Sander type II, III형 모두에서 변 형된 Ollier 도달법을 이용하여 금속판 고정 이외의 방법으로 비교 적 양호한 결과를 얻을 수 있었다.본 연구의 제한점으로, 저자들은 대부분의 종골 관절 내 골절에 서 본 연구의 방법으로 수술하였기에 금속판을 이용한 수술 방법 과의 객관적 비교 결과가 어렵다는 점이 있다. 많은 수의 환자들을 대상으로 수술적 도달법 또는 고정 기구에 따른 임상 결과의 전향 적 비교 연구가 이루어진다면, 각각의 수술 기법을 객관적 판단 및 비교 분석하는 데 도움이 될 것으로 생각된다.
결 론
저자들은 관절 내 종골 골절의 수술적 치료로 6.5 mm 해면골 전 산나사못 또는 Steinmann 핀 버팀 고정법을 이용하여 방사선적 지 표 및 임상적 결과가 만족스러움을 알 수 있었다. 또한, 4주간의 석 고 부목 고정 후에 관절운동 및 부분 체중부하가 가능할 정도의 충 분한 고정력을 가지는 것도 알 수 있었다. 종골 관절 내 골절에서 변형된 Ollier 도달법을 이용하여 후방 관절면의 충분한 시야 확보 를 통하여 정확한 정복 및 고정을 한다면, 6.5 mm 해면골 전산나 사못 또는 Steinmann 핀을 이용한 버팀 고정술은 일반적으로 많이 이용되고 있는 외측 도달법을 이용한 금속판 고정에 비교하여 손 색 없는 훌륭한 수술법으로 생각된다. 또한, 추후 금속 제거술 시 에도 최소 침습적으로 시행할 수 있는 장점이 있다.
REFERENCES