Total hip arthroplasty (THA) has become a popular surgi- cal treatment for hip disease; however, it is commonly fol- lowed by pain, which is difficult to diagnose as the cause of it is unknown.1) There are many possible causes of such pain, including infection, loosening of the prosthesis, and
iliopsoas tendinitis. Adverse local tissue reaction (ALTR) and pseudotumors after metal-on-metal (MoM) THA can also cause postoperative pain. It has been reported that ALTR can occur not only on MoM bearing surfaces but also when using polyethylene liners.2)
ALTR has few other characteristic clinical and phys- ical findings, apart from pain, and cannot be revealed by radiography. Plain computed tomography (CT) and mag- netic resonance imaging (MRI) are valuable tools in this respect. ALTR is characterized by the production and pro- liferation of fluid components or necrotic tissue and often appears between the soft tissues around the artificial joint prosthesis. Numerous reports have shown the usefulness
Fluorodeoxyglucose Positron-Emission Tomography/Computed Tomography and Magnetic Resonance Imaging for Adverse Local Tissue Reactions near Metal Implants after Total
Hip Arthroplasty: A Preliminary Report
Makoto Kimura, MD, Nobuhiro Kaku, MD, Yuta Kubota, MD, Hiroaki Tagomori, MD, Hiroshi Tsumura, MD
Department of Orthopedic Surgery, Faculty of Medicine, Oita University, Yufu, Japan
Background: Plain computed tomography (CT) and magnetic resonance imaging (MRI) are useful for diagnosing adverse local tis- sue reactions after metal-on-metal total hip arthroplasty (THA), but metal artifacts can hamper radiological assessments near the implants. We sought to clarify the usefulness of 18F-fluorodeoxyglucose positron-emission tomography (18F-FDG-PET) CT and MRI in the periprosthetic region, which is difficult to assess after THA due to metal artifacts.
Methods: We performed preoperative 18F-FDG-PET/CT and 18F-FDG-PET/MRI, as well as plain CT and MRI, in 11 metal-on-metal THA patients who underwent revision surgery.
Results: Most patients showed high FDG uptake in the metal artifact areas and pseudotumors in the 18-F-FDG-PET/CT and 18-F- FDG-PET/MRI scans. Intraoperative intra-articular macroscopic and histopathological intra-articular granulation tissue findings were suggestive of adverse local tissue reaction.
Conclusions: The enhanced uptake in the metal artifact areas seemed to reflect adverse local tissue reaction. Therefore, 18F-FDG- PET/CT and 18-F-FDG-PET/MRI can be useful for the auxiliary diagnosis of adverse local tissue reactions after metal-on-metal THA.
Keywords: Arthroplasty, Computed tomography, Fluorodeoxyglucose F18, Metal-on-metal joint prostheses, Positron-emission to- mography
Copyright © 2021 by The Korean Orthopaedic Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Clinics in Orthopedic Surgery • pISSN 2005-291X eISSN 2005-4408 Received September 19, 2020; Revised December 24, 2020;
Accepted December 28, 2020 Correspondence to: Nobuhiro Kaku, MD
Department of Orthopedic Surgery, Faculty of Medicine, Oita University, 1-1 Idaigaoka Hasama-machi, Yufu, Oita 879-5593, Japan
Tel: +81-97-586-5872, Fax: +81-97-586-6647 E-mail: [email protected]
of MRI, which has a clearer soft-tissue delineation than CT.3) MRI is also recommended in the ALTR diagnostic algorithm for MoM THA.4)
However, even with MRI, which allows diagnosis of pseudotumors away from the metal prosthesis, lesions in the prosthesis’ vicinity are difficult to assess due to the influence of metal artifacts. Many studies have reported that metal ions from bearing surfaces and head-neck junc- tions within the joint can cause ALTR.5) Therefore, the existence of an abnormality, particularly in the early stages of ALTR, often cannot be determined by imaging, as the initial pathogenesis of ALTR is likely to be in the vicinity of the prosthesis. Improving the diagnostic performance in this metal artifact area is an essential requirement for the early detection of ALTR, even in the absence of a remote pseudotumor or fluid collection. The usefulness of metal- artifact-reduction sequence (MARS)-MRI modalities has been reported in recent years, but they are not yet com- monly used.6)
18F-fluorodeoxyglucose positron-emission tomog- raphy (18F-FDG-PET) has been recognized as a useful imaging modality for cancer detection.7) In addition, its usefulness for detecting post-THA surgical infections and laxity has recently been reported.8) In recent years, it has become possible to perform 18-F-FDG-PET/CT and 18-F- FDG-PET/MRI in combination with each other, which allows for simultaneous anatomical and qualitative evalu- ation by PET. CT is usually more versatile because it has a wider imaging area and requires a shorter imaging time.
However, when the pathology has a limited location, MRI is more valuable than CT, particularly for anatomical iden- tification of soft tissues and evaluation of fluid lesions, and it does not involve radiation exposure.
The use of 18F-FDG-PET to investigate ALTR after THA has rarely been reported9-11) and has been limited to 18F-FDG-PET alone or 18F-FDG-PET/CT combination.
However, there have been no reports of 18F-FDG-PET combined with MRI. In addition, there are no reports of the usefulness of 18F-FDG-PET/CT and 18F-FDG-PET/
MRI in the area where metal artifacts appear near the ar- tificial joint. The purpose of this study was to clarify the usefulness of 18F-FDG-PET/CT and 18F-FDG-PET/MRI for evaluations of the region near the prosthesis with metal artifacts in patients with ALTR after THA.
METHODS
Ethics
This prospective study was performed in accordance with the ethical standards as laid down in the 1964 Declara-
tion of Helsinki and its later amendments or comparable ethical standards. The present study was approved by the Institutional Review Board of Oita University (IRB No.
1396; April 16, 2018), and all study participants provided informed consent before the initiation of FDG-PET.
Patients
The present study included patients with recurrent hip pain after primary MoM THA, who underwent revision surgery between May 2018 and February 2020. ALTR was suspected, and revision surgery was performed because of poor clinical improvement, resistance to conservative treatment, and prolonged or increased pain in all patients.
The study population consisted of 9 patients with 11 joints (6 right hips and 5 left hips). Eight patients were female, and 1 was male. The causative diseases were osteoarthritis of the hip in 8 cases and rheumatoid arthritis in 3 cases.
The acetabular components used in the primary THA were the M2aMagnum (Biomet, Warsaw, IN, USA) in 6 cases, the M2aRadial (Biomet) in 2 cases, the Pinnacle in 2 cases (DePuy Synthes, Warsaw, IN, USA), and the Metasul in 1 case (Zimmer, Warsaw, IN, USA). For the femoral stem, 2 patients received an AML prosthesis (DePuy Syn- thes), 1 patient received a Natural Hip stem (Zimmer), and 8 patients received a Bi-Metric stem (Zimmer). A re- vision was performed using a posterolateral approach, and cementless implants were used in all cases. Eight of the revisions consisted of the liner and ball-head-only replace- ments, while 3 were acetabular-side revisions. There were no cases of simultaneous bilateral surgery.
After a preoperative MRI, 18F-FDG- PET/MRI was performed to evaluate the area in which metal artifacts occur in the vicinity of the prosthesis. We focused on the presence or absence of FDG uptake around the hip joint, the maximum standardized uptake value (SUV) in the early phase, and the maximum SUV in the delay phase.
Imaging diagnoses, including determining whether pseu- dotumors were present outside the metal artifacts, were performed by two orthopedic surgeons (MK and NK).
Preoperative Plain CT
CT was performed using a Biograph 40 TruePoint (Sie- mens, Munich, Germany) with a slice thickness of 3 mm and an interval of 2 mm.
Preoperative Plain MRI
Patients underwent MRI with a MAGNETOM Skyra (Siemens), and a 3.0-T MRI scanner was used with T1- weighted spin-echo (SE), T2-weighted SE, and short tau inversion recovery (STIR) sequences.
Acquisition of PET/CT and MRI
According to the FDG-PET protocol, all patients fasted for at least 6 hours before the examination, and the 18F- FDG dose was 3.7 MBq/kg. 18F-FDG-PET images were acquired within the range of the orbit to the thigh using a BIOGRAPH 40 PET scanner (Siemens). The blood sugar levels were checked before the injection, and the scan was performed if blood sugar levels were < 150 mg/dL. The early and delayed phase images were obtained after 60 minutes and between 90 and 120 minutes, respectively.
The FDG-PET data were reconstructed in a 168 × 168 ma- trix.
CT was performed using the same scanner (BIO- GRAPH 40; Siemens) at 120 kV and 220 mAs (CARE Dose4D). The slice thickness was 3 mm, and the interval was 2 mm. MRI was performed on a 3-T system (Achieva;
Philips, Best, The Netherlands) using a 32-channel cardiac coil. MR images were obtained with T1-weighted, T2- weighted, and STIR sequences in the coronal and axial planes, and diffusion images were also obtained, all of which represent MARS-MRI.
Image Analysis
The 18F-FDG-PET/MRI was reconstructed with image analysis software (AZE Virtual Place Fujin; AZE, Chiyoda, Japan) because the 18F-FDG-PET and MRI devices were independent. The SUVmax was calculated in the area of the highest uptake around the artifact near the artificial joint. In the evaluation of pseudotumors, uptake in the
18F-FDG-PET/MRI was expressed as high uptake (SUV value of 3.5 and above and colored red), highly photopenic (SUV of 1.76 to 3.4 and colored orange or yellow), weak (SUV of 0.1 to 1.75 and colored green), and none (SUV of 0 and colored purple or black).
Histological Review
Resected samples were preserved in 10% buffered forma- lin, and sections were stained with hematoxylin and eosin by a pathological technologist (MK). Specimens obtained by revision operation were evaluated by a pathologist (MK) and an orthopedic surgeon (NK). Pathology results were calculated using the aseptic lymphocytic-dominated vasculitis-associated lesion (ALVAL) score, based on the report of Campbell et al.12) The ALVAL score was evalu- ated based on three factors: synovial lining, inflammatory infiltration, and tissue organization were scored on a scale of 0‒3, 0‒3, and 0‒4 points, respectively, with a total score rated on a 10-point scale. A total score of 0‒4 was classified as low, 5‒8 as moderate, and 9‒10 as high. In cases where the assessments between the two evaluators differed, scores were discussed until a consensus was reached.
RESULTS
The mean age at revision was 68.4 ± 5.9 years. The mean time from primary THA to examination was 7.1 ± 3.9 years, and this period exceeded 3 years in all patients. All patients had dull pain (Table 1). Laboratory data, such as
Table 1. Patient Characteristics Case no. Sex Age*
(yr) Side Original
disease Acetabular
implant model Stem
implant model Interval period†
(mo) WBC
(× 103/μL) CRP (mg/dL)
1 F 70 R RA Pinnacle AML 58 5.2 0.07
2 F 70 L RA Pinnacle AML 55 5.2 0.07
3 M 82 R OA Metasul Natural hip 66 4.6 0.7
4 F 58 L OA M2aMagnum Bi-Metric 42 8.55 1.4
5 F 75 L OA M2aMagnum Bi-Metric 62 6.55 0.11
6 F 66 L OA M2aRadial Bi-Metric 73 5.17 0.08
7 F 66 R OA M2aRadial Bi-Metric 84 9.47 0.12
8 F 68 R RA M2aMagnum Bi-Metric 81 7.84 0.04
9 F 69 R OA M2aMagnum Bi-Metric 95 4.97 0.04
10 F 64 R OA M2aMagnum Bi-Metric 89 4.99 0.06
11 F 65 L OA M2aMagnum Bi-Metric 84 4.86 0.08
WBC: white blood cell count, CRP: C-reactive protein, R: right, L: left, RA: rheumatoid arthritis, OA: osteoarthritis of the hip.
*Age at revision surgery. †The period from primary total hip arthroplasty to the examination.
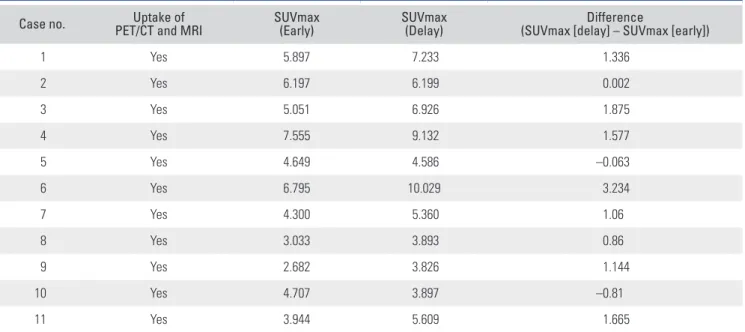
the white blood cell count and C-reactive protein level, did not suggest infection in any of the patients. Preoperative radiographs and CT did not show periprosthetic radio- lucency or osteolysis in any of the patients. Preoperative plain CT and MRI showed metal artifacts in the prosthe- sis’ vicinity in all cases, while pseudotumor images outside the metal artifacts were found in 8 cases. All cases dem- onstrated 18F-FDG-PET uptake within the metal artifact areas, with mean SUVmax values of 4.98 ± 1.45 and 6.06 ± 2.01 in the early phase and delay phase, respectively (Table 2). The difference between the SUVmax values of the early and delay phases was 1.08 ± 1.05. In the 8 cases with non- artifactual pseudotumor images away from the metal artifact area, 4 cases showed strong uptake, and their plain MR images showed areas of mixed brightness in T1, T2, or both sequences (Table 3).
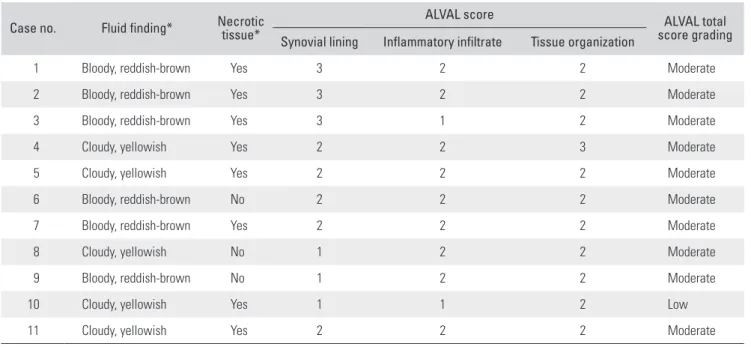
Intraoperatively, all patients had macroscopic ne- crotic tissue and fluid uptake in the joint (Table 4). The ALVAL score for histopathology of granulation tissue ob- tained intraoperatively was moderate in 10 cases and low in 1 case (Table 4). Clinical symptoms, such as preopera- tive pain, improved after revision in all cases.
Case Presentation
Case 2 is a representative case. Plain CT and MRI did not allow evaluation due to the presence of metal artifacts near the artificial joint, but pseudotumors outside the metal ar- tifacts could be visualized more clearly on plain MRI than
on plain CT (Fig. 1A and B). 18F-FDG-PET/CT and 18F- FDG-PET/MRI showed high uptake in the metal artifact area (Fig. 1C and D). As 18F-FDG-PET/MRI provides clearer findings for muscles and pseudotumors surround- ing the metal artifact than 18F-FDG-PET/CT, it facilitates
Table 3. Findings of Pseudotumor Outside of Metal Artifacts in Plain MRI and PET/MRI
Case no. MRI T1 MRI T2 Uptake of PET/MRI
1 NP NP NP
2 Low High None
3 Mixed Mixed High uptake overall
4 Low High High uptake overall
5 NP NP NP
6 Iso Mixed Highly photopenic
7 Low Mixed Highly photopenic
8 Low High Weak
9 Iso High Weak
10 NP NP NP
11 Low High None
MRI: magnetic resonance imaging, PET: positron-emission tomography, NP: there were no findings of pseudotumor on MRI, Mixed: mixed signal intensity.
Table 2. FDG-PET Images in the Area of Metal Artifacts
Case no. Uptake of
PET/CT and MRI SUVmax
(Early) SUVmax
(Delay) Difference
(SUVmax [delay] – SUVmax [early])
1 Yes 5.897 7.233 1.336
2 Yes 6.197 6.199 0.002
3 Yes 5.051 6.926 1.875
4 Yes 7.555 9.132 1.577
5 Yes 4.649 4.586 –0.063
6 Yes 6.795 10.029 3.234
7 Yes 4.300 5.360 1.06
8 Yes 3.033 3.893 0.86
9 Yes 2.682 3.826 1.144
10 Yes 4.707 3.897 –0.81
11 Yes 3.944 5.609 1.665
FDG-PET: fluorodeoxyglucose positron-emission tomography, CT: computed tomography, MRI: magnetic resonance imaging, SUV: standardized uptake value.
the understanding of the anatomical relationship between tissues. Bloody fluid and necrotic tissue were found in the intracapsular joint (Fig. 2A-C), and corrosion of the stem
neck or ball head was observed (Fig. 2D and E). The total ALVAL score of this case was 7 (Fig. 2F).
Table 4. Macroscopic and Histological Findings of Intra-articular Tissue Case no. Fluid finding* Necrotic
tissue*
ALVAL score ALVAL total
score grading Synovial lining Inflammatory infiltrate Tissue organization
1 Bloody, reddish-brown Yes 3 2 2 Moderate
2 Bloody, reddish-brown Yes 3 2 2 Moderate
3 Bloody, reddish-brown Yes 3 1 2 Moderate
4 Cloudy, yellowish Yes 2 2 3 Moderate
5 Cloudy, yellowish Yes 2 2 2 Moderate
6 Bloody, reddish-brown No 2 2 2 Moderate
7 Bloody, reddish-brown Yes 2 2 2 Moderate
8 Cloudy, yellowish No 1 2 2 Moderate
9 Bloody, reddish-brown No 1 2 2 Moderate
10 Cloudy, yellowish Yes 1 1 2 Low
11 Cloudy, yellowish Yes 2 2 2 Moderate
ALVAL: aseptic lymphocytic-dominated vasculitis-associated lesion.
*Intra-articular macroscopic findings.
Fig. 1. Preoperative imaging in a 70-year-old female. She underwent bilateral total hip arthroplasty with the same metal-on-metal prosthesis in both hips. (A) Plain computed tomography (CT) image. There are extensive areas around the bilateral hip prostheses that are difficult to assess due to metal artifacts. (B) Plain magnetic resonance imaging (MRI) image (T1). There is a marked artifact on both sides. A cystic pseudotumor is seen posterior to the left hip prosthesis. This can be identified more clearly on MRI than on CT. (C) Fluorodeoxyglucose-positron-emission tomography (FDG-PET)/CT image.
Uptake near both prostheses is present in the region of metal artifacts. (D) FDG-PET/MRI image. The large pseudotumor on the left side is clearly visible and no uptake occurred in the area. There are uptakes near the metal implants. The uptakes on PET/MRI are more sharply delineated than on PET/CT.
PET/MRI enables the identification of the anatomical positional relationship of uptakes for easier differentiation from the surrounding soft tissue.
A B
C D
DISCUSSION
In this study, 18F-FDG-PET/CT and MRI were used to evaluate cases of groin pain after MoM THA. 18F- FDG- PET showed high uptake near the prosthesis with metal artifacts on plain CT or MRI in all cases. The enhanced uptake within the metal artifact area seemed to reflect ALTR, indicating that 18F-FDG-PET/CT and 18F-FDG- PET/MRI can be useful for the auxiliary diagnosis of ALTR after MoM THA. The uptakes on 18-F-FDG-PET/
MRI were more sharply delineated than on 18-F-FDG- PET/CT, and 18-F-FDG-PET/MRI enabled the identifica- tion of the anatomical positional relationship of uptakes for easier differentiation from the surrounding soft tissue.
Groin pain after THA can be caused by various reasons including loosening of the acetabular component, stress fracture, iliopsoas tendinitis, impingement, pelvic os- teolysis, and infection, but it can also be caused by ALTR, which is difficult to diagnose based on clinical symptoms alone.13) If a pseudotumor is present at a distance from the prosthesis, it can be evaluated by CT or MRI. Although a pseudotumor located in an area away from metal artifacts is one of the important findings for the diagnosis of ALTR,
there are cases in which a remote pseudotumor has not occurred in the early stages of ALTR. One of our patients had a high uptake in the metal artifact area and no remote pseudotumor in the right hip, and a moderate uptake in the metal artifact area and a large remote pseudotumor without uptake in the left hip (Fig. 1). In this patient, plain MRI could not distinguish ALTR in proximity to the ar- tificial joint because the technique is highly susceptible to interference from metal artifacts. Besides, pseudotumors by ALTR, which can be classified as cystic, solid, and mixed types,14,15) showed different uptake levels in the present study (Table 3). There was no association between the degree of the uptake in the remote pseudotumor and near the artificial joint in the present study (Tables 2 and 3, Fig. 1). These results also showed that it would be diffi- cult to estimate the degree of inflammation in the artificial joint’s vicinity due to ALTR based on findings such as the presence or absence, size, and uptake of a remote pseudo- tumor. Therefore, it is essential to improve the diagnostic performance of imaging modalities in the metal artifact area in order to allow early detection of ALTR caused by metal ions from the bearing surfaces in the joint and the head-neck junction.
Fig. 2. Intraoperative intra-articular macroscopic findings and histopathological findings of intra-articular granulation tissue. (A) The pseudotumor formation is cystic. (B) Venous joint fluid with a bloody reddish-brown color is present. (C) Necrotic tissue is observed in the intracapsular joint. (D) A portion of the stem neck is discolored and demonstrates macroscopic corrosion. (E) At the fitting portion, the ball head appears to be missing and demonstrates some corrosion. (F) In the joint capsule, giant cells, foam cells, collagen fibers, and metallic powders are present in the tissue.
Multinucleated imaginal cell phagocytosis of metallic powder can also be observed (H&E, × 400).
A B C
D E F
MARS-MRI may be superior to 18F-FDG-PET/
MRI in terms of low cost and less invasiveness, avoidance of intravenous administration of 18F-FDG, and radiation exposure. However, even if MARS-MRI leads to a clearer depiction of the metal artifact than plain MRI, it is still unknown whether MARS-MRI can visualize the inflam- matory pathology such as ALTR near the artificial joint.
Besides, even if dedicated software for MARS is attached to the existing MRI main unit, it will be difficult to reduce artifacts depending on the model of the MRI main unit, and the image of the tissue around metal artifacts will be- come unclear when the metal artifacts are further reduced by adjusting the sequence.
PET is often used to diagnose neoplasms,7) and its potential for the assessment of inflammation has been reported. It has been used as a tool for the objective inter- pretation of the severity of inflammatory diseases, such as rheumatoid arthritis and psoriatic arthritis.16) The uptake in PET for inflammation has also been characterized as showing less change or a decreasing trend in the applica- tion of dual time-point imaging, without showing a mark- edly increasing trend.17) Reinartz et al.8) reported a trend for infection and loosening based on the PET uptake area and SUV uptake values. There are no clear diagnostic cutoffs, although SUVs in cases of infection and loosen- ing have been assessed. Choe et al.18) found that the mean SUVmax of infection was relatively large at 11 (5‒17). Re- inartz et al.8) also stated that for values above 5‒6, the pos- sibility of infection may also have to be considered.
Regarding pseudotumors after THA, Kisielinski et al.9) reported the imaging potential of FDG-PET in a case of removal and revision of a pseudotumor, with an SU- Vmax of 5 at a distance from the prosthesis. Makis et al.
reported that FDG-PET/CT revealed the imaging charac- teristics of necrotic pseudotumors and differentiated these from malignant soft-tissue tumors.10) Aro et al. reported the usefulness of 18F-FDG-PET/CT for the imaging of pseudotumors, as compared to 68-Ga citrate.11) In the pres- ent study, the pseudotumor uptake seemed higher for solid or mixed findings on plain MRI (Table 3). On the other hand, Zhuang et al.19) reported nonspecific and physiologi- cal uptakes in contact with the bearing surfaces of the pros- thesis and head-neck junction after THA. Gelderman et al.20) reported a physiological mean SUV of 2.5 at the joint of the prosthesis. Imaging patterns have also been reported for uptake in asymptomatic patients’ prostheses.21) There- fore, caution should be exercised in diagnosing ALTR for all intra-articular uptakes in contact with the prosthesis after MoM THA. Even in moderate uptakes (SUV ≥ 2.5), careful diagnosis using clinical findings is required.
All near-joint uptakes, including those seen in the early and delay phases, had SUVs > 2.5 and showed a marked tendency to accumulate within metal artifact areas rather than in relatively remote pseudotumors. Although malignant lymphomas and gastrointestinal malignancies have been reported to show a tendency to increase the SUV value in the delay phase, as compared to the early phase,22,23) the mean value in this study was 1.08, without a tendency for a marked increase. The uptake in ALTRs was more pronounced in cases with malignant lymphomas and gastrointestinal malignancies than in pseudotumors in the early phase. On the other hand, there was a variability of SUV values among cases with near-joint uptake (Table 2), although our data showed high SUV values overall.
Based on previous reports,8,18) the SUV value also varies for patients with prosthetic joint infection as an inflamma- tory disease. It would be especially difficult to determine a definite SUV for the diagnosis of inflammatory diseases.
When there seems to be some variability in SUV values in ALTR, it is important not to neglect the comprehensive diagnostic process based on the consideration of other in- formation such as the clinical course of symptoms, blood or joint fluid examinations, and image findings.
18F-FDG-PET features of benign tumors were in contrast to those of malignant tumors. In addition, all cas- es in this study had macroscopic findings at revision and histopathological findings consistent with ALTR, such as findings of inflammation and necrosis in the joint. Thus, the uptakes seen in PET in the vicinity of the prosthesis after MoM THA may be an imaging finding indicative of ALTR.
Clinical studies showed that it is difficult to diag- nose ALTR on plain CT and MRI due to metal artifacts but combining these with 18F-FDG-PET may allow delin- eation of inflammation (which may cause clinical symp- toms, such as pain) in the metal artifact areas. 18-F-FDG- PET/MRI seemed to be superior to 18-F-FDG-PET/CT for understanding the anatomy of the condition because it could better delineate pseudotumors and surrounding soft tissues than 18F-FDG-PET/CT. On the other hand, pseu- dotumors located away from the joints did not show high uptake, particularly when containing fluid components, demonstrating the limitations of the sensitivity of 18F- FDG-PET examination.
Regarding limitations of the present study, the study design is a case series with a small number of samples, and the time to surgery and the type of scanner used were dif- ferent in each case. Furthermore, a comparative study with asymptomatic cases was not performed. Although there is no doubt that MRI is safer in terms of radiation exposure
than CT, a previous report24) has suggested that MRI is problematic in cases with metal prostheses due to thermal fluctuation in the metal, and the choice of using CT is de- pendent on the patient’s preference or condition. MRI and CT should be performed after checking contraindications, such as the possibility of pregnancy, cardiac pacemaker models, and history of claustrophobia. Informed consent should be obtained after a thorough explanation to all pa- tients, including the additional cost.
In conclusion, this study suggests that 18F-FDG- PET/CT and 18F-FDG-PET/MRI could demonstrate the presence of a lesion and the severity of inflammation with- in metal artifact areas. In addition, 18F-FDG-PET/MRI seems to be excellent for enhancing the understanding of the overall pathology of ALTR after THA, as it also clearly delineates the surrounding soft tissue, including pseudo- tumors. With imaging study findings in the metal artifact areas using 18F-FDG-PET/CT and 18F-FDG-PET/MRI, we were able to bring ourselves closer to the diagnosis of ALTR based on comprehensive findings, including other information such as the patient’s medical history, physical findings, laboratory data, and other image findings. In the present study, we focused on post-THA ALTR, but 18F- FDG-PET/CT and 18F-FDG-PET/MRI should also be useful auxiliary diagnostic tools for the early diagnosis of pathological conditions that develop in the vicinity of the prosthesis after THA, such as iliopsoas tendinitis. Howev-
er, the diagnosis of post-THA diseases could not be accu- rately determined with findings of 18F-FDG-PET/CT or 18F-FDG-PET/MRI alone. We hope that our study results will help orthopedic surgeons provide another diagnostic option for patients with unknown pain after THA.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGEMENTS
We are thankful to Dr. Masashi Kataoka (MD, PhD) for technical support and histological evaluation in the pres- ent study. He is the histopathology specialist in the field of orthopedics at Physical Therapy Course of Study, Faculty of Welfare and Health Sciences, Oita University Hospital, Oita, Japan.
ORCID
Makoto Kimura https://orcid.org/0000-0002-7190-6075 Nobuhiro Kaku https://orcid.org/0000-0002-4041-1870 Yuta Kubota https://orcid.org/0000-0003-1426-1482 Hiroaki Tagomori https://orcid.org/0000-0002-6185-0098 Hiroshi Tsumura https://orcid.org/0000-0002-5384-822X
REFERENCES
1. Classen T, Zaps D, Landgraeber S, Li X, Jager M. Assess- ment and management of chronic pain in patients with stable total hip arthroplasty. Int Orthop. 2013;37(1):1-7.
2. Hjorth MH, Mechlenburg I, Soballe K, Roemer L, Jakobsen SS, Stilling M. Higher prevalence of mixed or solid pseudo- tumors in metal-on-polyethylene total hip arthroplasty com- pared with metal-on-metal total hip arthroplasty and resur- facing hip arthroplasty. J Arthroplasty. 2018;33(7):2279-86.
3. Nawabi DH, Gold S, Lyman S, Fields K, Padgett DE, Potter HG. MRI predicts ALVAL and tissue damage in metal-on-metal hip arthroplasty. Clin Orthop Relat Res.
2014;472(2):471-81.
4. Chalmers BP, Perry KI, Taunton MJ, Mabry TM, Abdel MP.
Diagnosis of adverse local tissue reactions following metal- on-metal hip arthroplasty. Curr Rev Musculoskelet Med.
2016;9(1):67-74.
5. Natu S, Sidaginamale RP, Gandhi J, Langton DJ, Nargol AV.
Adverse reactions to metal debris: histopathological features of periprosthetic soft tissue reactions seen in association
with failed metal on metal hip arthroplasties. J Clin Pathol.
2012;65(5):409-18.
6. Jungmann PM, Agten CA, Pfirrmann CW, Sutter R. Ad- vances in MRI around metal. J Magn Reson Imaging. 2017;
46(4):972-91.
7. Lee JW, Lee SM. Radiomics in oncological PET/CT: clinical applications. Nucl Med Mol Imaging. 2018;52(3):170-89.
8. Reinartz P, Mumme T, Hermanns B, et al. Radionuclide imaging of the painful hip arthroplasty: positron-emission tomography versus triple-phase bone scanning. J Bone Joint Surg Br. 2005;87(4):465-70.
9. Kisielinski K, Cremerius U, Reinartz P, Niethard FU. Fluor- deoxyglucose positron emission tomography detection of inflammatory reactions due to polyethylene wear in total hip arthroplasty. J Arthroplasty. 2003;18(4):528-32.
10. Makis W, Rush C, Abikhzer G. Necrotic pseudotumor caused by a metal-on-metal total hip prosthesis: imaging characteristics on (18)F-FDG PET/CT and correlative imag-
ing. Skeletal Radiol. 2011;40(6):773-7.
11. Aro E, Seppanen M, Makela KT, Luoto P, Roivainen A, Aro HT. PET/CT to detect adverse reactions to metal debris in patients with metal-on-metal hip arthroplasty: an ex- ploratory prospective study. Clin Physiol Funct Imaging.
2018;38(5):847-55.
12. Campbell P, Ebramzadeh E, Nelson S, Takamura K, De Smet K, Amstutz HC. Histological features of pseudotumor-like tissues from metal-on-metal hips. Clin Orthop Relat Res.
2010;468(9):2321-7.
13. Lombardi AV Jr, Barrack RL, Berend KR, Cuckler JM, Jacobs JJ, Mont MA, et al. The Hip Society: algorithmic ap- proach to diagnosis and management of metal-on-metal arthroplasty. J Bone Joint Surg Br. 2012;94(11 Suppl A):14-8.
14. Hart AJ, Satchithananda K, Liddle AD, et al. Pseudotumors in association with well-functioning metal-on-metal hip prostheses: a case-control study using three-dimensional computed tomography and magnetic resonance imaging. J Bone Joint Surg Am. 2012;94(4):317-25.
15. Hauptfleisch J, Pandit H, Grammatopoulos G, Gill HS, Murray DW, Ostlere S. A MRI classification of peripros- thetic soft tissue masses (pseudotumours) associated with metal-on-metal resurfacing hip arthroplasty. Skeletal Radiol.
2012;41(2):149-55.
16. Vijayant V, Sarma M, Aurangabadkar H, Bichile L, Basu S.
Potential of (18)F-FDG-PET as a valuable adjunct to clini- cal and response assessment in rheumatoid arthritis and seronegative spondyloarthropathies. World J Radiol. 2012 28;4(12):462-8.
17. Kumar R, Basu S, Torigian D, Anand V, Zhuang H, Alavi A.
Role of modern imaging techniques for diagnosis of infec- tion in the era of 18F-fluorodeoxyglucose positron emission tomography. Clin Microbiol Rev. 2008;21(1):209-24.
18. Choe H, Inaba Y, Kobayashi N, et al. Use of 18F-fluoride PET to determine the appropriate tissue sampling region for improved sensitivity of tissue examinations in cases of sus- pected periprosthetic infection after total hip arthroplasty.
Acta Orthop. 2011;82(4):427-32.
19. Zhuang H, Chacko TK, Hickeson M, et al. Persistent non- specific FDG uptake on PET imaging following hip arthro- plasty. Eur J Nucl Med Mol Imaging. 2002;29(10):1328-33.
20. Gelderman SJ, Jutte PC, Boellaard R, et al. 18F-FDG-PET uptake in non-infected total hip prostheses. Acta Orthop.
2018;89(6):634-9.
21. Aydin A, Yu JQ, Zhuang H, Alavi A. Patterns of 18F-FDG PET images in patients with uncomplicated total hip arthro- plasty. Hell J Nucl Med. 2015;18(2):93-6.
22. Nakayama M, Okizaki A, Ishitoya S, Sakaguchi M, Sato J, Aburano T. Dual-time-point F-18 FDG PET/CT imaging for differentiating the lymph nodes between malignant lym- phoma and benign lesions. Ann Nucl Med. 2013;27(2):163-9.
23. Miyake KK, Nakamoto Y, Togashi K. Dual-time-point 18F-FDG PET/CT in patients with colorectal cancer:
clinical value of early delayed scanning. Ann Nucl Med.
2012;26(6):492-500.
24. Yamazaki M, Ideta T, Kudo S, Nakazawa M. Evaluation of artificial hip joint with radiofrequency heating issues dur- ing mri examination: a comparison between 1.5 T and 3 T.
Nihon Hoshasen Gijutsu Gakkai Zasshi. 2016;72(6):480-8.