CASE REPORT
특발성 맹장 궤양의 미세천공에 의한 다발성 화농성 간농양
염동한, 손기창, 주민수, 조동호, 조은영, 김학철
원광대학교 의과대학 내과학교실
Multiple Pyogenic Liver Abscesses Caused by Microperforation of an Idiopathic Cecal Ulcer
Dong Han Yeom, Ki Chang Sohn, Min Su Chu, Dong Ho Jo, Eun Young Cho, and Haak Cheoul Kim Department of Internal Medicine, Wonkwang University College of Medicine, Iksan, Korea
Idiopathic cecal ulcer is a rare disease entity of unknown cause diagnosed by ruling out other known causes of cecal ulceration.
The most common complication of an idiopathic cecal ulcer is bleeding; perforation, peritonitis, abscess, and stricture formation have been noted. The authors treated a 53-year-old woman who presented with fever and intermittent right upper quadrant abdominal pain. Multiple pyogenic liver abscess and a solitary cecal ulcer were diagnosed by radiologic, endoscopic, and pathologic examination, followed by laparoscopic cecectomy. After extensive study, we concluded that this patient’s liver abscesses were a complication of the idiopathic cecal ulcer. Herein, we report a case of multiple pyogenic liver abscess caused by microperforation of idiopathic cecal ulcer. (Korean J Gastroenterol 2016;67:44-48)
Key Words: Idiopathic cecal ulcer; Liver abscess
Received June 13, 2015. Revised August 31, 2015. Accepted September 5, 2015.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2016. Korean Society of Gastroenterology.
교신저자: 김학철, 54538, 익산시 무왕로 895, 원광대학교병원 내과
Correspondence to: Haak Cheoul Kim, Department of Internal Medicine, Wonkwang University Hospital, 895 Muwang-ro, Iksan 54538, Korea. Tel: +82-63-859-2672, Fax: +82-63-855-2025, E-mail: [email protected]
Financial support: This study was supported by a grant from Wonkwang University in 2014. Conflict of interest: None.
INTRODUCTION
Idiopathic cecal ulcers are rare, and diagnosed by ruling out other known causes of cecal ulceration. Therefore, it is of- ten difficult to correctly diagnose the disease preoperatively.
The disease may mimic ulcerative colonic diseases, such as ulcerating colonic malignancy or ulcerative colitis, and colo- noscopic biopsies may yield negative results. Endoscopists should be aware of the endoscopic, radiologic, and patho- logic manifestations of the disease. The most common com- plication of an idiopathic cecal ulcer is bleeding, but perfo- ration, peritonitis, abscess, and stricture formation have also been observed.1 To the best of our knowledge, this report de- scribes the first case of multiple pyogenic liver abscesses
caused by microperforation of an idiopathic cecal ulcer.
CASE REPORT
A 53-year-old woman was referred to our hospital for sus- pected multiple liver metastases, based on abdomen-pelvis CT findings suggestive of multiple hepatic low attenuated lesions. She had a three day history of fever, and a history of intermittent right upper and lower quadrant abdominal pain for more than three months, but complained of no other symptoms, including diarrhea, constipation, hematochezia, or bowel-habit changes. There was no history of abdominal pain and no chronic underlying gastrointestinal or general medical illness. Diet, travel, and medication history were
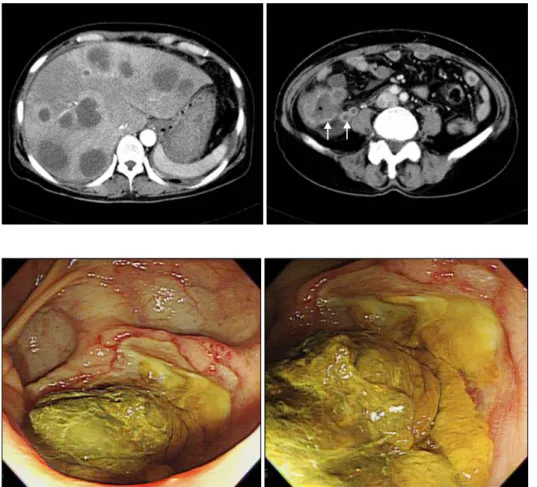
Fig. 2. Two views of a large cecal ulcer occupying approximately two-thirds of the cecum with overlying necrotic tissue found on colonoscopy.
Fig. 1. Multifocal rim-enhancing well- defined low-attenuation lesions of variable size are seen within both liver lobes. The arrows indicate the wall thickening of cecum with mild appen- diceal dilatation.
unremarkable. On physical examination, she was febrile with tachycardia and orthostatic blood pressure changes. No or- ogenital ulcer or skin manifestation was noted. Her abdomi- nal examination revealed localized pain in the right upper quadrant of the abdomen upon palpation without guarding or rebound tenderness, and direct tenderness without re- bound tenderness in the right lower quadrant.
Laboratory findings showed a white cell count of 1.5×104/L, hemoglobin of 12.6 g/dL, platelet count of 9.9×104/L, prothrombin time of 14.7 sec, AST/ALT ratio of 131/82 IU/L, total/direct bilirubin of 2.82/1.63 mg/dL, total protein/albumin of 5.3/1.9 g/dL, and CRP of 420.68 mg/L.
Serum carcinoembryonic antigen was within normal limits.
Stool was negative for ova, parasites, and enteric pathogens.
CT of the abdomen and pelvis showed multifocal rims-en- hancing cystic lesions of variable size in both liver lobes and abnormal wall thickening of the cecum with mild appendiceal dilatation and fluid collection in the perihepatic and right par- acolic gutter (Fig. 1). Three sets of blood cultures were com- pleted, and broad spectrum antimicrobial therapy was initiated.
Ultrasonography-guided percutaneous liver biopsy and fine needle aspiration were performed to evaluate the multi- ple cystic mass liver lesions. Pathologic evaluation revealed reactive hepatocytes with acute inflammation and necrotic debris. Purulent discharge was aspirated and sent for bacte- rial culture. However, all cultures were negative. The patient underwent repeated ultrasonography-guided placement of a percutaneous drainage catheter. Despite abscess drainage and antibiotic treatment for 11 days, her general status de- teriorated with intermittent high fever and sustained right up- per and lower quadrant abdominal pain. The suspicion of a contagious focus in the cecum needed to be addressed.
Furthermore, the abnormal thickening of the cecal wall need- ed to be differentiated from cancer. For these reasons, colo- noscopy was performed. Colonoscopy revealed that the en- tire colon appeared normal up to the proximal ascending co- lon, where a large ulceration with central necrotic tissue in- vagination was identified in the cecum (Fig. 2). Biopsy re- vealed a lymphoplasmacytic infiltrate and a benign lympho- cyte aggregate.
A laparoscopic cecectomy on the same day was performed
Fig. 4. Microscopic examination revealed acute and chronic inflam- mation, cellular infiltration, and ulcer with periappendicitis (H&E,
×200).
Fig. 3. The surgical findings showed 2×2 cm necrosis with micro- perforation on cecum.
Table 1. Differential Diagnosis of a Cecal Ulcer
Inflammatory bowel disease (ulcerative colitis, Crohn’s disease) Vasculitis (Behcet’s disease, systemic lupus erythematosus, etc.) Intestinal tuberculosis
Medications (nonsteroidal anti-inflammatory drugs, steroids, etc.) Infections (bacterial, fungal, viral, parasitic, or other)
Malignancy
based on the assumption that the abscess was caused by a complication of the cecal ulcer with direct extension from the bowel lumen to the liver. Surgical findings showed 2×2 cm sized necrosis on the cecum with microperforation (Fig. 3).
Microscopic examination revealed acute suppurative in- flammation and an ulcer with periappendicitis (Fig. 4). There was no evidence of carcinoma, ameba, mycobacteria, or cyto- megalovirus infections. Therefore, we diagnosed an idio- pathic cecal ulcer after histologically viewing the nonspecific inflammation. We suggest that the liver abscess occurred as complications of the idiopathic cecal ulcer. After surgery, the patient’s condition rapidly improved, and she was dis- charged one month later. Six months after discharge, an ab- domen and pelvis CT was obtained, revealing no evidence of recurrent abscess, but multiple small, low attenuated foci re- mained in the liver.
DISCUSSION
Little is known about idiopathic cecal ulcers. The clinical terminology of this disease is confusing, as it has been de- scribed as a simple, nonspecific, solitary ulcer.2 Usually an idiopathic cecal ulcer can be identified based on its location in the cecum, as other ulcers are located in the ascending co- lon, sigmoid colon, or other site. However, diagnosis is made af- ter excluding other diseases that may cause cecal ulcers, such as malignancy, inflammatory bowel disease, vasculitis, in- testinal tuberculosis, medications, and infections (Table 1).2,3 Due to the increasing use of colonoscopy for diagnosis of low-
er gastro-intestinal diseases, idiopathic cecal ulcers may be more frequently found. Endoscopists should keep the possi- bility of an idiopathic cecal ulcer in mind if colonoscopic find- ings are not typical of other ulcerating lesions in the cecum and the biopsy indicates only inflammation. We report our ex- perience and will briefly review clinical aspects of idiopathic cecal ulcers.
An early report by Cameron4 in 1939 documented patients between the ages of 18 and 80 years (average age 37 years) with nonspecific cecal ulcers. Previous case report series suggest an equal distribution in men and women.1,2 Idiopath- ic cecal ulcers have varied clinical manifestations, depend- ing on the onset and associated complications. Acute or chronic right lower quadrant pain is the most common pre- senting symptom. Other symptoms are similar to lower gas- tro-intestinal tract diseases.1 The ulcer may be asympto- matic and discovered incidentally on colonoscopy.2 However, the clinical picture can change dramatically with complica- tions such as bleeding or perforation.5 This report describes the first case of multiple pyogenic liver abscesses caused by microperforation of an idiopathic cecal ulcer. Bacterial
pathogens can reach the liver by five different routes: portal vein, hepatic artery, biliary tract, penetrating trauma, and di- rect extension from a contiguous, usually intra-abdominal, rarely pleural focus. We suggest this as a mechanism that leads to liver abscesses. When the bowel is the suspected source, caused by bacteremia from a severe bowel infection, spread is possible through the weakened bowel mucosa (via the portal vein), and hematogenous spread is also possible (via the hepatic artery).6,7 Portal bacteremia and pyle- phlebitis occur in ulcerative colitis,8-10 as ulceration and loss of integrity of the normal mucosal barrier may predispose ul- cer patients to microbial invasion of the portal venous system.11,12 Patients with inflammatory bowel disease have an increased risk of multiple liver abscesses.13 Our patient did not exhibit pylephlebitis in the imaging study or bacter- emia in the blood culture, but the long-lasting gastro- intestinal symptoms suggested that the gradually pro- gressive cecal ulceration caused the transmigration of in- testinal microbes, and the liver abscess was the result of por- tal bacteremia. Moreover, because this patient’s cecum mu- cosa was not functioning properly, there was fluid collection in the right paracolic gutter. In addition, there was right lower quadrant pain for over three months, and microperforation was found during the surgery. Thus, it is likely that the conta- gious focus had been there for a long time and spread directly to the liver.
It is important to exclude other diseases by thorough ex- amination to diagnose idiopathic cecal ulcers. Radiographic and colonoscopic technical advances are resulting in in- creased discovery and diagnosis of this rare disease.14,15 A barium enema examination is frequently abnormal, but sel- dom specific. Changes include luminal narrowing, mucosal irregularity, and/or ulcer crater formation are usually in- terpreted as cecal carcinoma. Idiopathic cecal ulcer CT find- ings demonstrate diffuse or abnormal cecal wall thickening and adjacent fat stranding. These findings are non-specific, reflecting inflammation of the cecal wall and pericecal fat.
Radiographic techniques for detecting ulcers in the cecum seldom provide a definitive diagnosis due to nonspecific ra- diologic features.16 Colonoscopy is used to diagnose cecal ul- cers presenting with abdominal pain and abnormal radio- graphic imaging. Shallman et al.17 described the gross patho- logic appearance of benign cecal ulcers as resembling a pep- tic ulcer ranging from 5 mm to 5 cm in size, usually located
on the antimesenteric border within 2 cm from the ileocecal valve, and well demarcated from normal tissue, as in our patient. Ulcers are generally solitary, although they may be multiple. In this case, it is essential to differentiate from in- testinal Behcet’s disease, which has very similar endoscopic findings. Intestinal Behcet’s disease may be diagnosed if symptoms corresponding to Behcet’s disease are present, such as ulceration in the oral mucosa, genital ulcers, or skin or eye lesions,18 or if vasculitis and lymphocyte infiltration in the perivascular space are observed histologically. Behcet’s disease was excluded in our patient since she did not show any clinical symptoms of Behcet’s disease, and biopsy showed lymphoplasmacytic infiltrate and lymphocyte ag- gregate, but not vasculitis. In chronic cecal ulcers, a false tu- mor-like appearance may be visualized.1,19 The only method available for a more precise preoperative diagnosis is colonoscopy.20
Management is dictated by both the clinical presentation and the gravity of the major differential diagnostic consi- derations.2,19 In our report, the therapeutic option was surgi- cal resection. However, non-surgical, watchful management may be reasonable in stable patients with later stages of idio- pathic cecal ulcers.2 No specific guidelines exist for treating idiopathic cecal ulcers, only for treating associated complications. Each case should be individualized, with sur- gical management kept as an option if complications arise.1 In fact, no tenet argues against a diagnostic and therapeutic operation in patients with a suspected colon perforation, in- tra-abdominal abscess, or presumptive diagnosis of malig- nancy or appendicitis. An ulcer discovered at the time of sur- gery, with no evidence of malignancy, may be treated without further intervention by stapler-wedge cecectomy, or more ex- tensive right hemicolectomy.15 In our case, high fever and gastrointestinal symptoms continued despite percutaneous drainage for the liver abscess, but symptoms eased after cecectomy. Therefore, we believe that the liver abscesses were a complication of the cecal ulcer, although cecal ulcer perforation was not confirmed before surgery.
In conclusion, our case of multiple pyogenic liver ab- scesses should be considered a complication due to an idio- pathic cecal ulcer. Colonoscopy is beneficial in cases of liver abscesses with cecal pathology for diagnosis and manage- ment decisions.
REFERENCES
1. Chi KD, Hanauer SB. Benign solitary cecal ulcer: a case report and review of the literature. Dig Dis Sci 2003;48:2207-2212.
2. Blundell CR, Earnest DL. Idiopathic cecal ulcer. Diagnosis by co- lonoscopy followed by nonoperative management. Dig Dis Sci 1980;25:494-503.
3. Mark HI, Ballinger WF 2nd. Nonspecific ulcer of the colon, report of a case and review of 51 cases from the literature. Am J Gastroenterol 1964;41:266-291.
4. Cameron JR. Simple non-specific ulcer of the caecum. Br J Surg 1939;26:526-531.
5. Corry RJ, Bartlett MK, Cohen RB. Erosions of the cecum: a cause of massive hemorrhage. Am J Surg 1970;119:106-110.
6. Albrecht H. Bacterial and miscellaneous infections of the liver.
In: Boyer TD, Manns MP, Sanyal AJ, eds. Zakim and Boyer's hep- atology: a textbook of liver disease. 6th ed. Philadelphia:
Elsevier, 2012:656-670.
7. Gross RG, Reiter B, Korsten MA. Pyogenic liver abscess compli- cating colonoscopic polypectomy. Gastrointest Endosc 2008;
67:767-768.
8. Brooke BN, Slaney G. Portal bacteraemia in ulcerative colitis.
Lancet 1958;1:1206-1207.
9. Eade MN, Brooke BN. Portal bacteraemia in cases of ulcerative colitis submitted to colectomy. Lancet 1969;1:1008-1009.
10. Felsen J, Wolarsky W. Suppurative pylephlebitis with bacteremia in chronic ulcerative colitis. Ann Intern Med 1950;33:211-216.
11. Greenstein AJ, Sachar DB, Lowenthal D, Goldofsky E, Aufses AH
Jr. Pyogenic liver abscess in Crohn's disease. Q J Med 1985;
56:505-518.
12. Mir-Madjlessi SH, McHenry MC, Farmer RG. Liver abscess in Crohn's disease. Report of four cases and review of the literature. Gastroenterology 1986;91:987-993.
13. Margalit M, Elinav H, Ilan Y, Shalit M. Liver abscess in in- flammatory bowel disease: report of two cases and review of the literature. J Gastroenterol Hepatol 2004;19:1338-1342.
14. Gardiner GA, Bird CR. Nonspecific ulcers of the colon resembling annular carcinoma: subject review. Radiology 1980;137:331- 334.
15. Rao PM, Novelline RA, Zukerberg L. Solitary caecal ulcer syn- drome, a benign condition which mimics the CT appearance of caecal carcinoma. Clin Radiol 1999;54:331-333.
16. Brodey PA, Hill RP, Baron S. Benign ulceration of the cecum.
Radiology 1977;122:323-327.
17. Shallman RW, Kuehner M, Williams GH, Sajjad S, Sautter R.
Benign cecal ulcers. Spectrum of disease and selective management. Dis Colon Rectum 1985;28:732-737.
18. International Study Group for Behçet's Disease. Criteria for diag- nosis of Behçet's disease. Lancet 1990;335:1078-1080.
19. Cha JM, Lee JI, Choe JW, Lee SH, Kim KY. A case report of idio- pathic cecal ulcer mimicking cecal cancer. Dig Dis Sci 2008;53:3259-3262.
20. Nagasako K, Ikezawa H, Gyo S, Takemoto T. Preoperative diag- nosis of a nonspecific ulcer of the cecum by colonofiberscopy:
report of a case. Dis Colon Rectum 1972;15:413-415.