서 론
고혈압은 한국인의 대표적인 만성질환으로 2015년 국민건강영양 조사 통계에 따르면 고혈압 유병률은 32.7%로 전년도 29.8%에 비해 상승하였다. 하지만 이들 중 고혈압 조절률(만 30세 이상 고혈압 유 병자 중 수축기 혈압이 140 mmHg 미만이고 이완기 혈압이 90
mmHg 미만인 분율)은 46.2%로 여전히 낮은 수준이다.1) 목표 혈압에 도달하는 것은 고혈압의 합병증 예방에 있어서 매우 중요하다. 한 대 규모 무작위 연구에 의하면 적절한 고혈압 치료는 뇌졸중 상대위험 도를 30%–40% 및 급성심근경색 상대위험도를 20%–25% 감소시킨다 고 하였다.2)
일반적으로 고혈압 치료는 비약물적 치료로 시작하며 이 중에 규
Received July 20, 2017 Revised September 20, 2017 Accepted October 7, 2017
Corresponding author Byungsung Kim
Tel: +82-2-958-8696, Fax: +82-2-958-8699 E-mail: [email protected]
ORCID: http://orcid.org/0000-0002-4984-6918
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2018.8.5.676 eISSN 2233-9116
Korean J Fam Pract. 2018;8(5):676-683
Korean Journal of Family Practice
KJFP
고혈압 환자에서 신체활동이 심혈관 질환에 미치는 영향
김동후
1, 김병성
1,*, 원장원
1, 최현림
1, 김선영
2, 장민혜
1, 신우영
31
경희대학교병원 가정의학과,
2경희대학교 대학원 의학과,
3식품의약품안전처 바이오생약심사부 생물제제과
The Relationship Between Physical Activity and Risk of Cardiovascular Disease Among Hypertensive Persons: A Community-Based Prospective Study
Donghoo Kim
1, Byungsung Kim
1,*, Changwon Won
1, Hyunrim Choi
1, Sunyoung Kim
2, Minhye Jang
1, Wooyoung Shin
31
Department of Family Medicine, Kyung Hee University Hospital;
2Department of Medicine, Graduate School, Kyung Hee University, Seoul;
3Division of Biologics, Department of Biopharmaceuticals and Herbal Medicine Evaluation, National Institute of Food and Drug Safety Evaluation, Ministry of Food and Drug Safety, Cheongju, Korea
Background: Hypertension, a major risk factor for the development of cardiovascular disease, is a prevalent chronic disease in Korea. It has been shown previously that regular physical activity is effective in controlling blood pressure and preventing cardiovascular disease. We investigated the relationship between physical activity and cardiovascular disease in patients with hypertension.
Methods: This study used data collected in the Ansan and Anseong Cohort, performed by the Korean Center for Disease Control. The baseline survey was carried out between 2000–2001 and two prospective biennial surveys were conducted and analyzed.
Results: Of the 8,807 total subjects included in the analysis, 2,805 patients were hypertensive, and 705 patients were diagnosed with cardiovascular disease at 12-year follow up. The non-hypertensive subjects in the 7.5–15 metabolic equivalent hours per week (MET-hr/wk) group had the lowest cardiovascular disease risk (hazard ratio [HR], 0.65; 95% confidence interval [CI], 0.45–0.95). Of the hypertensive subjects, the risk of cardiovascular disease was lowest in the 15–30 MET-hr/wk group (HR, 0.6; 95% CI, 0.43–0.84). Multivariate analysis of hypertension showed a decrease in the risk of cardiovascular disease in the 15–30 MET-hr/wk group (HR, 0.69; 95% CI, 0.49–0.98). Additionally, the risk was significantly reduced in women compared to men at 15–30 MET-hr/wk (HR, 0.61; 95% CI, 0.39–0.97).
Conclusion: The risk of cardiovascular disease was significantly reduced in patients with hypertension and, specifically, females with hypertension who performed 15-30 MET-hr/wk of physical activity.
Keywords: Exercise; Metabolic Equivalent; Hypertension; Cardiovascular Diseases
김동후 외. 고혈압 환자에서 신체활동이 심혈관 질환에 미치는 영향
Korean Journal of Family PracticeKJFP
칙적인 신체활동 및 유산소운동은 중요한 비중을 차지한다.3) 장기적 인 유산소운동은 평균적으로 수축기 혈압을 46 mmHg, 이완기 혈압 을 3 mmgHg 감소시킨다고 알려져 있다.4-6) 또한 규칙적인 신체활동 은 심혈관계 합병증 예방에도 효과가 있는데 신체활동을 가장 활동 적으로 하는 사람들은 가장 활동적이지 않은 사람들과 비교했을 때 심혈관 질환이 발병할 위험이 30%–40% 낮다.7) 이러한 활동량과 심 혈관 질환의 위험 관계는 연령, 성별, 민족성에 관계없이 일관성이 있 어 보인다.8) 이 외에도 규칙적인 신체활동은 제2형 당뇨, 비만, 유방 암과 대장암, 불안, 우울증, 인지기능 이상 등의 여러 질환을 예방하 고 개선하는 효과를 나타냈다.9,10)
하지만 한국인의 신체활동은 여전히 부족한 상황으로 국민건강 영양조사 결과 걷기 실천율은 2005년 19세 이상에서는 60.7%, 2015 년 40.7%, 65세 이상에서는 54.6%에서 35.8%로 큰 폭으로 감소하였 다.1) 고혈압은 그 자체로 관상동맥 질환, 뇌졸중, 말초혈관질환 등의 다양한 심혈관 질환의 위험을 증가시키기 때문에 신체활동의 감소 가 이러한 합병증 발생 위험을 더욱 높일 수 있다.11) 또한 고혈압은 우 리 나라에서 가장 흔한 만성질환으로 심혈관 질환의 합병증을 예방 하는 것은 더욱 중요하다. 따라서 본 연구는 우리나라의 농촌과 도 시를 대표하는 코호트인 안산·안성 코호트를 통하여 정상 혈압군 과 고혈압군 참가자들을 대상으로 일반적 특성을 비교하고 심혈관 질환 합병증의 발병 위험이 높은 고혈압 환자를 대상으로 신체활동 과 심혈관 질환과의 연관성을 알아보고자 시행되었다.
방 법
1. 연구 대상
본 연구는 질병관리본부의 한국인유전체 역학조사사업(Korean Genome and Epidemiology Study, KoGES)의 일부인 안산·안성 코호 트에 수집된 데이터에 근거하였다. 안산·안성 코호트는 우리나라의 만성 질환에 대한 전향적 지역 기반 역학 연구를 위해 수립되었
다.12,13) 연구에 참여하기 전 적어도 6개월간 연구 지역에 거주한 연령
40–69세 성인을 대상으로 하였고, 연령, 성별, 거주지로 층화하여 표 본 추출을 시행하였다. 안성에서는 7,192명의 연구 참여가능 성인 중 5,018명이 참여했고(응답률 70%) 안산은 15,580명의 연구 참여 가능 성인 중 5,020명(32.2%)이 참여했다. 연구 참여자는 등록 당시 10,030 명이었고 이 중 사망자는 총 633명이었으며 6차 추적조사까지 총 5,906명이 완료하였다. 기초 조사는 2000–2001년에 시행되었고 2년 마다 추적 조사를 시행하고 있는데, 본 연구는 총 12년 간의 조사 결 과를 대상으로 하여 분석하였다. 기반조사 당시 심혈관 질환이 동반 되어 있는 참가자는 분석에서 제외 되었으며 총 8,807명을 대상으로
시행되었다. 연구 기간 중 대상자의 정보 수집 및 검사는 동일한 기 계와 잘 훈련된 동일한 연구자에 의해 수행되었다. 혈압, 키, 몸무게 는 표준화된 방법으로 계측하였고 공복 상태의 혈중 포도당 농도 및 총 콜레스테롤, 중성지방, high density lipoprotein (HDL) 콜레스테 롤은 중앙 검사실에서 분석하였다.12,13)
본 연구는 경희대학교병원 임상시험심의위원회(Institutional Re- view Board, IRB)에 의해 승인되었다(IRB no. KHUH 2016-06-336).
2. 변수 정의
혈압은 5분 이상 휴식을 취한 후 훈련된 조사원에 의하여 수은혈 압계를 이용하여 측정하였다. 혈압은 앉은 자세에서 오른쪽과 왼쪽 에서 잰 혈압의 평균치를 사용하였으며, 고혈압 환자는 수축기 혈압 이 140 mmHg 이상이거나, 이완기 혈압이 90 mmHg 이상인 사람 또 는 현재 고혈압 약을 먹고 있는 사람으로 정의하였다. 본 연구에서는 총 2,805명이 고혈압군으로 분류되었다.
당뇨, 이상지질혈증, 심부전, 악성종양 등의 질병력에 대해서는 자 가 보고 방식으로 의사에게 진단을 받은 경우 또는 현재 치료 중인 경우를 포함시켰다.
그 밖의 변수들로 흡연은 20갑 이상의 담배 흡연 여부에 대한 질 문에 대한 응답으로 ‘아니오’라고 응답한 경우 비흡연, ‘예’라고 응답 한 경우 중에서 다시 과거 흡연자와 현재 흡연자로 분류하였다. 음주 의 경우 원래 술을 마시지 못하거나 종교적인 문제 등으로 처음부터 술을 마시지 못한다고 응답한 비음주군과 과거 음주군과 현재 음주 군으로 나누어 분석하였다. 고혈압 약 및 폐경 후 여성호르몬 약물 복용 여부에 관해서도 미복용군과 과거 복용, 현재 복용 3가지 군으 로 분류하였다.
심혈관 질환의 발생은 관상동맥 질환 및 뇌졸중의 발생을 2년마 다 추적 조사하여 획득한 설문지를 바탕으로 하였고 관상동맥 질환 및 뇌졸중을 진단받았거나 치료를 받고 있다고 응답한 경우를 심혈 관 질환이 있다고 정의하였다.
신체활동의 종류에 따른 강도는 대사당량(metabolic equivalent, METs)으로 나타내는데, 1 METs는 휴식 시 1분당 체중 1 kg에 대해 산소 3.5 mL를 소모하는 것을 의미한다. 본 연구에서는 예시로 제시 된 활동 항목별로 METs 값을 주어 활동별 평균 MET 값을 산출한 후, 주당 활동 시간을 곱하여 MET-hr/wk로 계산하였다.
미국 보건당국은 일주일간 중등활동을 150–300분 또는 격한 활 동을 75–150분 수행하도록 권장하고 있으며, 이는 500–1,000 MET- min/wk에 해당한다.14)
또한 신체활동 지침을 성인과 65세 이상의 노인으로 나누어 제시 하고 있는데 65세 이상의 노인은 가장 비활동적인 신체활동을 보이
Original Article
Korean Journal of Family Practice
Donghoo Kim, et al. The Relationship Between Physical Activity and Risk of Cardiovascular Disease
Korean Journal of Family Practice
KJFP
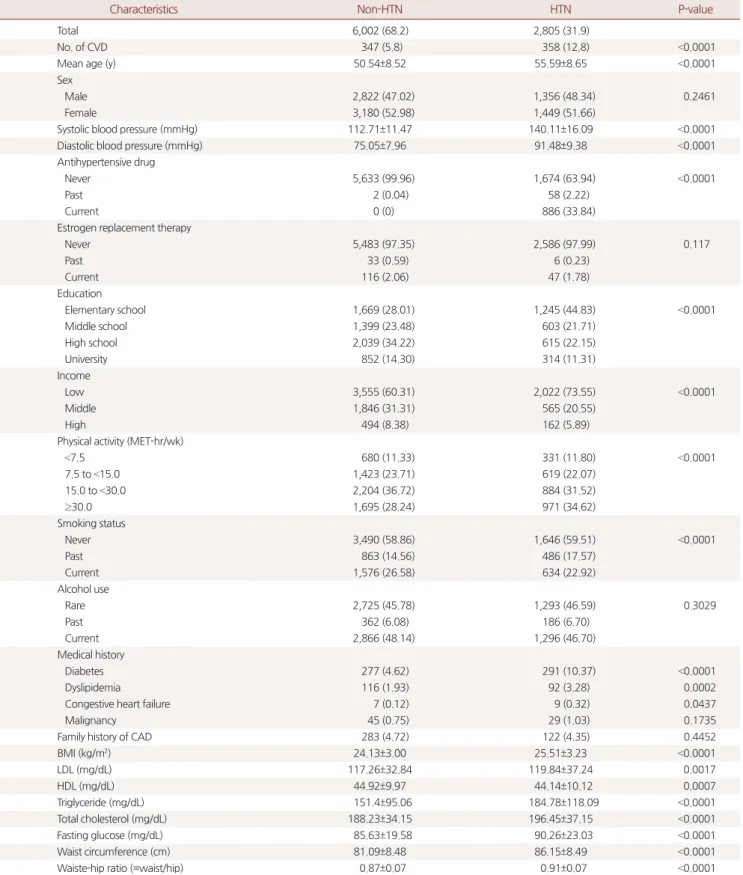
Table 1. Baseline characteristics of study population
Characteristics Non-HTN HTN P-value
Total 6,002 (68.2) 2,805 (31.9)
No. of CVD 347 (5.8) 358 (12.8) <0.0001
Mean age (y) 50.54±8.52 55.59±8.65 <0.0001
Sex
Male 2,822 (47.02) 1,356 (48.34) 0.2461
Female 3,180 (52.98) 1,449 (51.66)
Systolic blood pressure (mmHg) 112.71±11.47 140.11±16.09 <0.0001
Diastolic blood pressure (mmHg) 75.05±7.96 91.48±9.38 <0.0001
Antihypertensive drug
Never 5,633 (99.96) 1,674 (63.94) <0.0001
Past 2 (0.04) 58 (2.22)
Current 0 (0) 886 (33.84)
Estrogen replacement therapy
Never 5,483 (97.35) 2,586 (97.99) 0.117
Past 33 (0.59) 6 (0.23)
Current 116 (2.06) 47 (1.78)
Education
Elementary school 1,669 (28.01) 1,245 (44.83) <0.0001
Middle school 1,399 (23.48) 603 (21.71)
High school 2,039 (34.22) 615 (22.15)
University 852 (14.30) 314 (11.31)
Income
Low 3,555 (60.31) 2,022 (73.55) <0.0001
Middle 1,846 (31.31) 565 (20.55)
High 494 (8.38) 162 (5.89)
Physical activity (MET-hr/wk)
<7.5 680 (11.33) 331 (11.80) <0.0001
7.5 to <15.0 1,423 (23.71) 619 (22.07)
15.0 to <30.0 2,204 (36.72) 884 (31.52)
≥30.0 1,695 (28.24) 971 (34.62)
Smoking status
Never 3,490 (58.86) 1,646 (59.51) <0.0001
Past 863 (14.56) 486 (17.57)
Current 1,576 (26.58) 634 (22.92)
Alcohol use
Rare 2,725 (45.78) 1,293 (46.59) 0.3029
Past 362 (6.08) 186 (6.70)
Current 2,866 (48.14) 1,296 (46.70)
Medical history
Diabetes 277 (4.62) 291 (10.37) <0.0001
Dyslipidemia 116 (1.93) 92 (3.28) 0.0002
Congestive heart failure 7 (0.12) 9 (0.32) 0.0437
Malignancy 45 (0.75) 29 (1.03) 0.1735
Family history of CAD 283 (4.72) 122 (4.35) 0.4452
BMI (kg/m2) 24.13±3.00 25.51±3.23 <0.0001
LDL (mg/dL) 117.26±32.84 119.84±37.24 0.0017
HDL (mg/dL) 44.92±9.97 44.14±10.12 0.0007
Triglyceride (mg/dL) 151.4±95.06 184.78±118.09 <0.0001
Total cholesterol (mg/dL) 188.23±34.15 196.45±37.15 <0.0001
Fasting glucose (mg/dL) 85.63±19.58 90.26±23.03 <0.0001
Waist circumference (cm) 81.09±8.48 86.15±8.49 <0.0001
Waiste-hip ratio (=waist/hip) 0.87±0.07 0.91±0.07 <0.0001
Values are presented as number (%) or mean±standard deviation.
HTN, hypertension; CVD, cardiovascular disease; MET-hr/wk, metabolic equivalent-hours/week; CAD, coronary artery disease; BMI, body mass index; LDL, low density lipoprotein; HDL, high density lipoprotein.
김동후 외. 고혈압 환자에서 신체활동이 심혈관 질환에 미치는 영향
Korean Journal of Family PracticeKJFP
Table 2. Risk of cardiovascular disease between non-hypertensive and hypertensive persons using univariate cox regression analysis
Variable Non-HTN HTN
HR (95% CI) P-value HR (95% CI) P-value
Age 1.08 (1.07–1.09) <0.0001 1.06 (1.04–1.07) <0.0001
Sex
Male Reference Reference
Female 0.83 (0.67–1.02) 0.0727 1.17 (0.95–1.44) 0.1393
Antihypertensive drug
Never Reference
Past 1.25 (0.62–2.54) 0.5363
Current 1.8 (1.45–2.23) <0.0001
Estrogen replacement therapy
Never Reference Reference
Past 1.1 (0.27–4.42) 0.8922 1.07 (0.15–7.61) 0.9472
Current 0.56 (0.21–1.5) 0.246 0.76 (0.31–1.83) 0.5356
Education
Elementary school Reference Reference
Middle school 0.56 (0.43–0.73) <0.0001 0.71 (0.54–0.93) 0.0125
High school 0.35 (0.27–0.46) <0.0001 0.63 (0.47–0.83) 0.0009
University 0.35 (0.24–0.51) <0.0001 0.48 (0.32–0.72) 0.0005
Income
Low Reference Reference
Middle 0.49 (0.38–0.64) <0.0001 0.57 (0.43–0.77) 0.0002
High 0.46 (0.28–0.74) 0.0013 0.41 (0.23–0.76) 0.0041
Physical activity (MET-hr/wk)
<7.5 Reference Reference
7.5 to <15.0 0.65 (0.45–0.95) 0.0255 0.7 (0.5–0.99) 0.0449
15.0 to <30.0 0.73 (0.51–1.03) 0.0687 0.6 (0.43–0.84) 0.0027
≥30.0 1.04 (0.74–1.46) 0.8271 0.75 (0.55–1.03) 0.0743
Smoking status
Never Reference Reference
Past 1.28 (0.95–1.73) 0.103 0.98 (0.74–1.3) 0.8986
Current 1.42 (1.12–1.81) 0.0039 0.98 (0.75–1.27) 0.8745
Alcohol use
Rare Reference Reference
Past 0.95 (0.61–1.5) 0.8375 0.98 (0.65–1.47) 0.9099
Current 0.77 (0.62–0.96) 0.0189 0.77 (0.62–0.95) 0.0159
Medical history
Diabetes 2.65 (1.88–3.72) <0.0001 2.06 (1.55–2.72) <0.0001
Dyslipidemia 0.68 (0.28–1.65) 0.3946 0.95 (0.53–1.68) 0.8486
Malignancy 1.69 (0.63–4.53) 0.2959 0.92 (0.29–2.86) 0.8806
Family history of CAD 1.16 (0.74–1.83) 0.5094 0.83 (0.49–1.42) 0.5026
BMI (kg/m2)
Normal (<25) Reference Reference
Overweight (25 to <30) 1.28 (1.03–1.59) 0.0261 0.91 (0.73–1.14) 0.4174
Obese (≥30) 0.92 (0.49–1.74) 0.7949 1.13 (0.78–1.62) 0.5183
LDL cholesterol
High (≥160) 1.22 (0.88–1.70) 0.2383 1.41 (1.06–1.87) 0.0175
Normal (<160) Reference Reference
HDL (mg/dL)
Low (M<40, F<50) 1.11 (1.90–1.37) 0.3439 1.35 (1.09–1.68) 0.006
Normal (M≥40, F≥50) Reference Reference
Triglyceride (mg/dL)
High (≥150) 1.32 (1.06–1.63) 0.0118 1.38 (1.11–1.70) 0.0033
Normal (<150) Reference Reference
Donghoo Kim, et al. The Relationship Between Physical Activity and Risk of Cardiovascular Disease
Korean Journal of Family Practice
KJFP
는 연령대로 낙상 위험, 만성 질환 유무 등을 고려하여 능력과 조건 이 허용하는 만큼 활동량을 결정해야 하기 때문이다. 따라서 본 연 구에서는 기존 연구 결과 및 미국 보건당국의 권고사항에 근거하여 신체활동량은 총 4개 군으로 나누어 분석하였으며 <7.5 MET-hr/wk 군은 비활동군, 7.5 to <15.0 MET-hr/wk군은 경도 활동군, 15.0 to <30.0 MET-hr/wk군은 중등도 활동군, ≥30.0 MET-hr/wk군은 고강도 활동 군으로 분류하였고 연령에 따라 층화하여 분석을 시행하였다.14,15)
3. 통계 처리 및 분석
연령은 연속 변수로 분석하였으며 신체활동, 음주, 흡연, 교육 및 소득 수준, 체질량지수(body mass index), 허리둘레, 혈중 LDL 콜레스 테롤 농도, HDL 콜레스테롤 농도, 중성지방 농도 등은 범주형 변수 로 분석하였다. Cox 비례 위험 회기분석을 통하여 심혈관 질환 위험 도에 대한 생존 분석을 시행하였고 결과는 위험도(hazard ratio, HR) 및 95% 신뢰구간(95% confidence interval [CI])으로 제시하였다. 생존 분석은 연령, 성별, 체질량지수, 흡연, 음주, 당뇨, 이상지질혈증을 공 변량으로 추가적 모델을 제시하였다. 또한 고혈압군에서 신체활동 이 심혈관 질환에 미치는 영향은 성별 및 연령 군에 따라 별도로 분 석하였다. 모든 통계 분석은 SAS ver. 9.4 (SAS Institute, Cary, NC, USA) 를 통하여 이루어졌으며 P값 0.05 미만을 통계적으로 유의하다고 판 단하였다.
결 과
1. 연구 대상자의 임상적 특징
안산·안성 코호트 10,030명 중 심혈관 질환이 없는 8,807명이 분
석에 포함되었으며 이 중 고혈압 환자군은 2,805명이었다. 연구 대상 자의 평균 나이는 비고혈압군은 50.5세, 고혈압군은 55.6세였다. 심혈 관 질환은 12년 추적관찰 기간 동안 비고혈압군에서 347건(5.8%), 고 혈압군에서 358건(12.8%)으로 총 705건(8.0%) 발생하였다. 고혈압군 은 비고혈압군에 비하여 체질량지수 및 허리둘레가 컸고, LDL 콜레 스테롤 및 중성지방, 공복 혈당은 더 높은 경향을 보였다(Table 1).
2. 임상적 특징에 따른 심혈관 질환 발생의 위험도
고혈압군 및 비고혈압군에서 각각의 임상적 특징에 따른 심혈관 질환의 발생을 분석한 결과 고혈압군에서 현재 혈압약을 복용하는 군에서 그렇지 않은 군에 비하여 심혈관 질환 발생의 위험이 높았다 (HR, 1.8; 95% CI, 1.45–2.23). 또한 두 집단 모두에서 학력 및 교육 수준 이 높을수록 심혈관 질환의 위험도는 감소하였다. 신체활동은 비고 혈압군에서는 7.5–15 MET-hr/wk군에서 심혈관 질환 위험도가 가장 낮았고(HR, 0.65; 95% CI, 0.45–0.95) 고혈압군에서는 15–30 MET-hr/
wk군에서 위험도를 가장 감소시켰다(HR, 0.6; 95% CI, 0.43–0.84). 고 혈압군에서 고 LDL 콜레스테롤혈증 및 저 HDL 콜레스테롤혈증, 고 중성지방혈증은 심혈관 질환의 위험도를 유의하게 상승시켰으며 높은 공복 혈당 및 허리둘레, 허리엉덩둘레비 역시 높은 심혈관 질 환의 위험도와 유의하게 연관이 있었다(Table 2).
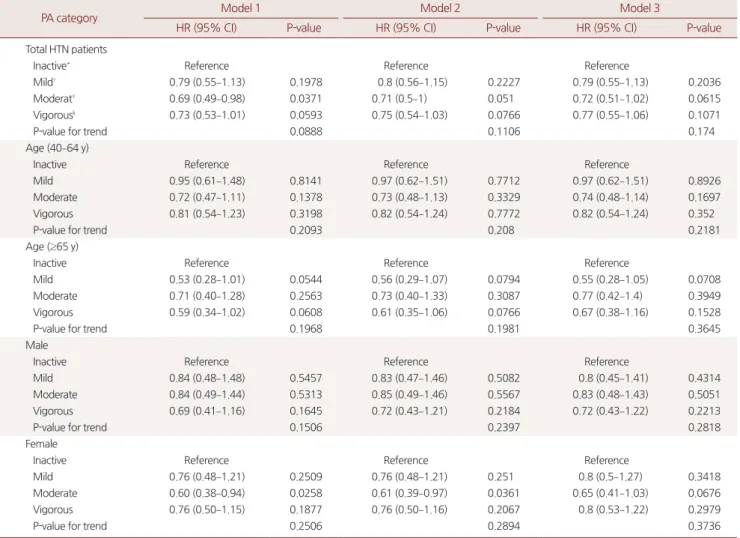
고혈압 환자군을 대상으로 신체활동과 심혈관 질환 발생의 위험 도를 확인한 결과 연령 및 성별을 보정하였을 때 중등도 활동군(15–
30 MET-hr/wk)에서 심혈관 질환의 위험을 유의하게 감소시켰다 (HR, 0.69; 95% CI, 0.49–0.98). 고혈압 환자군을 연령에 따라 층화하여 분석한 결과에서는 가장 신체활동이 적은 비활동군(0–7.5 MET-hr/
wk)에 비하여 더 높은 신체활동을 하는 군에서 심혈관 질환의 위험 Table 2. Continued
Variable Non-HTN HTN
HR (95% CI) P-value HR (95% CI) P-value
Total cholesterol (mg/dL)
High (≥240) 1.24 (0.85–1.80) 0.2647 1.26 (0.93–1.70) 0.1355
Normal (<240) Reference Reference
Fasting glucose (mg/dL)
High (≥126) 2.48 (1.61–3.83) <0.0001 1.97 (1.33–2.93) 0.0007
Normal (<126) Reference Reference
Waist circumference (cm)
Normal (M<90, F<80) Reference Reference
Obesity (M≥90, F≥80) 1.64 (1.33–2.03) <0.0001 1.73 (1.39–2.15) <0.0001
Waist:hip ratio
Normal (M<0.9, F<0.85) Reference Reference
Obesity (M≥0.9, F≥0.85) 2.08 (1.67–2.58) <0.0001 1.8 (1.39–2.32) <0.0001
HTN, hypertension; HR, hazard ratio; CI, confidence interval; MET-hr/wk, metabolic equivalent-hours/week; CAD, coronary artery disease; BMI, body mass index; LDL, low density lipoprotein; HDL, high density lipoprotein; M, male; F, female.
김동후 외. 고혈압 환자에서 신체활동이 심혈관 질환에 미치는 영향
Korean Journal of Family PracticeKJFP
도가 감소하는 추세를 보였지만 통계적으로 유의하지는 않았다. 성 별로 층화하였을 때 여성에서는 중등도 활동군(15–30 MET-hr/wk) 에서 심혈관 질환의 위험을 40% 낮추었으며(HR, 0.60; 95% CI, 0.38–
0.94), 이러한 추세는 생활 습관을 보정한 후에도 유지되었으나, 당뇨 및 고지혈증의 동반 질환을 보정한 후에는 남녀 모두에서 통계적 유 의하지 않았다(Table 3).
고 찰
본 연구는 한국의 성인 남녀에게서 신체활동 수준에 따라 심혈관 질환에 어떤 영향을 미치는지 알아보기 위하여 수행하였다. 고혈압 환자는 혈압 조절 및 심혈관계 합병증 예방을 위하여 적절한 신체활 동이 권고되기 때문에 고혈압 환자군을 대상으로 신체활동과 심혈
관 질환과의 연관성을 알아보고자 시행되었다. 정상혈압군과 고혈 압군을 나누어 분석하였을 때 고혈압군에서는 0–7.5 MET-hr/wk의 신체활동을 한 비활동군에 비하여 경도 활동군(7.5–15 MET-hr/wk) 과 중등도 활동군(15–30 MET-hr/wk)에서 심혈관 질환 위험도가 유 의하게 감소하였다. 다변량 분석 결과 전체 고혈압군 및 여성 고혈압 군에서 중등도 활동(15–30 MET-hr/wk)이 심혈관 질환의 발생을 낮 추는 것으로 드러났다.
이전의 대규모 연구들에서 높은 수준의 신체활동은 심혈관 질환 위험의 감소16)와 연관이 있고 1,000 kcal/wk의 에너지 소비를 할 경우 심혈관 질환 사망률을 20%–30% 낮춘다고 밝힌바 있다.17) 최근의 연 구들은 여성들에 초점을 두고 한 경우가 많았는데 미국에서 시행된 74,000명의 여성을 대상으로 한 대규모 연구에서 걷기와 활발한 운 동 모두 관상동맥 질환의 위험도 감소와 관련이 있었다.18) 또한 고혈
Table 3. Risk of cardiovascular disease according to physical activity in subjects with hypertension using multivariable cox regression analysis
PA category Model 1 Model 2 Model 3
HR (95% CI) P-value HR (95% CI) P-value HR (95% CI) P-value
Total HTN patients
Inactive* Reference Reference Reference
Mild† 0.79 (0.55–1.13) 0.1978 0.8 (0.56–1.15) 0.2227 0.79 (0.55–1.13) 0.2036
Moderat‡ 0.69 (0.49–0.98) 0.0371 0.71 (0.5–1) 0.051 0.72 (0.51–1.02) 0.0615
Vigorous§ 0.73 (0.53–1.01) 0.0593 0.75 (0.54–1.03) 0.0766 0.77 (0.55–1.06) 0.1071
P-value for trend 0.0888 0.1106 0.174
Age (40–64 y)
Inactive Reference Reference Reference
Mild 0.95 (0.61–1.48) 0.8141 0.97 (0.62–1.51) 0.7712 0.97 (0.62–1.51) 0.8926
Moderate 0.72 (0.47–1.11) 0.1378 0.73 (0.48–1.13) 0.3329 0.74 (0.48–1.14) 0.1697
Vigorous 0.81 (0.54–1.23) 0.3198 0.82 (0.54–1.24) 0.7772 0.82 (0.54–1.24) 0.352
P-value for trend 0.2093 0.208 0.2181
Age (≥65 y)
Inactive Reference Reference Reference
Mild 0.53 (0.28–1.01) 0.0544 0.56 (0.29–1.07) 0.0794 0.55 (0.28–1.05) 0.0708
Moderate 0.71 (0.40–1.28) 0.2563 0.73 (0.40–1.33) 0.3087 0.77 (0.42–1.4) 0.3949
Vigorous 0.59 (0.34–1.02) 0.0608 0.61 (0.35–1.06) 0.0766 0.67 (0.38–1.16) 0.1528
P-value for trend 0.1968 0.1981 0.3645
Male
Inactive Reference Reference Reference
Mild 0.84 (0.48–1.48) 0.5457 0.83 (0.47–1.46) 0.5082 0.8 (0.45–1.41) 0.4314
Moderate 0.84 (0.49–1.44) 0.5313 0.85 (0.49–1.46) 0.5567 0.83 (0.48–1.43) 0.5051
Vigorous 0.69 (0.41–1.16) 0.1645 0.72 (0.43–1.21) 0.2184 0.72 (0.43–1.22) 0.2213
P-value for trend 0.1506 0.2397 0.2818
Female
Inactive Reference Reference Reference
Mild 0.76 (0.48–1.21) 0.2509 0.76 (0.48–1.21) 0.251 0.8 (0.5–1.27) 0.3418
Moderate 0.60 (0.38–0.94) 0.0258 0.61 (0.39–0.97) 0.0361 0.65 (0.41–1.03) 0.0676
Vigorous 0.76 (0.50–1.15) 0.1877 0.76 (0.50–1.16) 0.2067 0.8 (0.53–1.22) 0.2979
P-value for trend 0.2506 0.2894 0.3736
Model 1: Adjusted for age and sex. Model 2: Model 1+ body mass index, smoking and drinking. Model 3: Model 2+diabetes mellitus and dyslipidemia.
PA, physical activity; HR, hazard ratio; CI, confidence interval; HTN, hypertension.
*Inactive (<7.5 MET-hr/wk), †Mild (7.5 to <15.0 MET-hr/wk), ‡Moderate (15.0 to <30.0 MET-hr/wk), §Vigorous (≥30.0 MET-hr/wk).
Donghoo Kim, et al. The Relationship Between Physical Activity and Risk of Cardiovascular Disease
Korean Journal of Family Practice
KJFP
압과 마찬가지로 심혈관 질환의 주 위험인자인 당뇨병을 동반하고 있는 5,125명의 여성을 대상으로 신체활동에 대한 설문을 사용한 연 구에서는 중등도에서 활동적인 강도의 신체활동을 한 가장 높은 5 분위수의 그룹에서 심혈관 질환의 위험을 45% 감소시키는 것으로 나타났다.19) 이처럼 심혈관 질환 발생의 주요 위험인자를 동반한 참 가자를 대상으로 한 연구에서도 신체활동의 효과가 유의하게 밝혀 진 것은 본 연구와 어느 정도 일치하는 경향을 보인다.
신체활동이 심혈관 질환 위험을 낮추는 기전에 대해서는 부분적 으로만 밝혀져 있다. 한 연구에서는, 신체활동이 혈관의 저항을 감 소시키고, 교감신경계 및 renin-angiotensin system을 억제시켜 혈압 을 낮추는 효과가 있으며20) 혈중 지질 농도 감소와도 연관이 있다고 하였다.21) 또 다른 연구에서는, 신체활동이 혈장 fibrinogen 농도 및 점성을 감소시키는 작용에 기여한다고 하였으며,20,22) 일부 연구자들 은 신체활동이 강력한 심혈관 질환의 위험인자인 2형 당뇨를 예방 하는 효과가 있다는 연구 결과를 통해23-27) 신체활동과 심혈관계질 환과의 연관성에 대한 기전을 밝히고자 하였다.
본 연구에서는 고혈압군에서 높은 수준의 신체활동이 심혈관 질 환의 위험도를 감소시키는 것을 부분적으로 확인할 수 있었다. 하지 만 몇 가지 제한점을 가지고 있는데 첫째로 신체활동의 경우 객관적 인 측정도구를 이용하여 신체활동량을 계측한 것이 아니라 설문조 사 정보를 활용하였으므로 주관적으로 평가하여 과다보고 가능성 이 있다는 점이다. 둘째, 관상동맥질환 및 뇌졸중의 발생 역시 설문 조사 방식으로 수집하였기 때문에 과대평가 되었을 수 있다. 본 연구 에서는 12년 추적관찰 기간 동안 심혈관 질환의 발생은 약 8.0%로 높 게 측정되었다. 셋째, 이 연구는 안산, 안성의 거주민을 대상으로 한 것으로 현재까지도 추적 조사가 진행 중이나 중도 탈락률이 약 50%
로 매우 높은 편으로 통계적인 검정력을 낮췄을 가능성이 있다. 넷 째, 안산·안성 코호트에서는 사망자료를 공개하지 않아 심혈관 질 환으로 인하여 사망한 참가자의 정보를 반영할 수 없었다.
그러나 본 연구는 비교적 큰 규모의 지역 기반 코호트를 바탕으로 신체활동이 심혈관 질환에 미치는 영향을 전향적으로 12년 동안 관 찰했다는 큰 강점이 있다. 또한 그 중에서도 고혈압 환자에게서 신체 활동이 심혈관 질환에 미치는 영향을 따로 분석하였는데 국내에서 전향적으로 이러한 영향을 본 연구는 거의 보고된 바가 없다. 또한 기존 연구들에서는 운동량 또는 여가 시간의 신체활동만 분석을 한 경우가 많은데 본 연구에서는 일상 생활에서의 신체활동을 모두 포 함하여 조사한 장점이 있다. 추후 신체활동량을 보다 객관적으로 평 가하여 이러한 연관성을 정확히 밝히기 위하여 더 많은 연구가 필요 할 것으로 생각된다.
요 약
연구배경:
고혈압은 한국의 대표적인 만성 질환으로 심혈관 질환 발병의 주요 위험 인자이다. 규칙적인 신체활동은 혈압 조절 및 심혈 관 질환 예방에 효과가 있다는 것은 이전의 연구들을 통하여 밝혀 진 바 있어 본 연구에서는 고혈압 환자에서 신체활동과 심혈관 질환 과의 연관성을 알아보고자 하였다.방법:
본 연구는 질병관리본부의 한국인유전체 역학조사사업(Ko- GES)의 일부인 안산 · 안성 코호트에 수집된 데이터에 근거하였다. 기 반 조사는 2000–2001년에 시행되었고 이후 12년 간의 추적조사 자료 를 분석하였다. 기반조사 당시 심혈관 질환이 동반되어 있던 사람은 분석에서 제외하였다.결과:
분석에 포함된 8,807명 중 고혈압군은 2,805명이었으며 12년 추적 조사 결과 새롭게 심혈관 질환이 발생한 경우는 705건이었다.비고혈압군에서는 경도 활동군(7.5–15 MET-hr/wk)에서 심혈관 질환 위험도가 가장 낮았고(HR, 0.65; 95% CI, 0.45–0.95) 고혈압군에서는 중등도 활동군(15–30 MET-hr/wk)에서 위험도가 가장 낮았다(HR, 0.6; 95% CI, 0.43–0.84). 고혈압군을 대상으로 다변량 분석 결과에서 도 중등도 활동군(15–30 MET-hr/wk)에서 심혈관 질환의 위험도가 감소하였다(HR, 0.69; 95% CI, 0.49–0.98). 특히 여성에서 중등도 활동 군(15–30 MET-hr/wk)이 심혈관 질환 위험도가 유의하게 낮았다 (HR, 0.60; 95% CI, 0.38–0.94).
결론:
전체 고혈압 환자군 및 여성 고혈압 환자군에서 중등도 신체 활동을 한 군에서 심혈관 질환의 위험도가 유의하게 감소하였다.중심단어:
신체활동; 대사당량; 고혈압; 심혈관 질환REFERENCES