서 론
난청은 세계적으로 흔한 건강 문제 중 하나이다. 미국에서 2001년 부터 2008년까지 시행된 연구에 따르면, 0.5, 1, 2, 4 kHz의 순음 청력 평균치 25 dB 이상 기준으로 12세 이상에서 약 20.3%가 단측 또는 양 측성 난청이 있으며, 40대부터 급격한 증가를 보여 70대 이상에서는 68.1%인 것으로 나타났다.1)
국내의 경우 2012년 국민건강통계 보고에 따르면, 0.5, 1, 2, 3 kHz의 순음 청력 평균치 40 dB 이상을 기준으로 12세 이상에서 양측성 난 청은 5.7%이고, 나이에 따라 유병률이 증가하며 70대 이상에서는 2 명 중 1명은 난청이 있는 것으로 나타났다.2)
난청은 언어 기능 장애를 유발하여 의사소통에 제한을 가져올 수 있으며 이러한 제한은 직업, 건강 관련 행위뿐만 아니라 정서적 상태 에 부정적인 영향을 줄 수 있는 만큼 심각한 문제가 될 수 있다.3) Received March 9, 2017 Revised June 10, 2017 Accepted July 5, 2017
Corresponding author Ji-Ho Choi Tel: +82-32-890-3547, Fax: +82-32-890-2195 E-mail: [email protected]
Copyright © 2017 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2017.7.6.892 eISSN 2233-9116
Korean J Fam Pract. 2017;7(6):892-897
Korean Journal of Family Practice
KJFP
40세 이상 한국 성인에서 흡연과 난청의 연관성:
2013년 국민건강영양조사 자료 이용
이유림, 최지호*, 이연지, 오정민, 송현진, 윤남희
인하대학교 의과대학 가정의학교실
Effect of Cigarette Smoking on Hearing Impairment in Korean Adults Over 40 Years-Old:
Based on the Data from Korean National Health and Nutrition Examination Survey, 2013
Yu Rim Lee, Ji-Ho Choi*, Yeon-Ji Lee, Jeong Min Oh, Hyeun Jin Song, Nam Hee Youn Department of Family Medicine, Inha University College of Medicine, Incheon, Korea
Background: Previous studies reported that smoking was associated with hearing impairment. However, the results were not consistent. Therefore, we aimed to analyze the effect of smoking on hearing impairment in Korean adults over 40 years of age.
Methods: This study included 4,212 participants over 40 years of age in the 2013 Korean National Health and Nutrition Examination Survey. Pure-tone audiometric testing was conducted and the frequencies tested were 0.5, 1, 2 and 3 kHz. Smoking status was categorized into two groups, smoking and non-smoking. The smoking group was divided according to number of cigarettes smoked smoked into 4 groups: 1–10, 11–20, and >20 cigarettes/day.
Results: In the smoking group, the prevalence of hearing impairment was increased (odds ratio [OR], 1.46; 95% confidence interval [CI], 1.260–1.685). In the age-stratified analysis, smoking was associated with hearing impairment in those aged 50–69 years. Adjusting for age, alcohol consumption, diabetes, hypertension, regular exercise, education, and noise exposure, we found that the smoking group had significantly increased hearing impairment compared to the non-smoking group (OR, 1.86; 95% CI, 1.514–2.283). In those aged 50–69 years, the OR was 2.07 (95% CI, 1.601–2.682).
The increase in prevalence according to smoking level was more prevalent (OR, 2.40; 95% CI, 1.582–3.645).
Conclusion: Smoking significantly influenced hearing impairment, and the risk increased greatly in those aged 50-69 years. There was a dose-response relationship between smoking level and prevalence.
Keywords: Hearing Loss; Smoking; Age; Sex
이유림 외. 40세 이상 한국 성인에서 흡연과 난청의 연관성 Korean Journal of Family Practice
KJFP
난청에 영향을 미치는 인자로는 나이가 가장 중요한 것으로 알려 져 있으며, 이외에도 인종, 성별, 직업, 교육수준, 당뇨, 고혈압, 소음 노출, 흡연, 만성중이염, 약물 등이 있다.4-9)
이 중 흡연은 혈액 순환을 악화시켜 청력 저하에 영향을 준다는 여러 연구가 있다. 반면, 다른 여러 연구에서는 흡연이 청력 저하와 관련이 없는 것으로 나타났다.10-14) 국내의 흡연과 난청의 연관성에 관한 연구는 아직 많지 않으며 각 연구마다 연구 방법에서 많은 차 이가 있어 다양한 결과가 있다. 흡연자에서 회화 영역과 고주파 영역 에서 난청이 유의하게 증가한다는 결과가 있는 반면,15) 흡연이 중등 도 이상의 난청에는 유의한 상관관계가 없다는 결과도 있다.16) 또한, 저주파 영역은 흡연량에 따라 영향을 받지만, 고주파 영역에서는 유 의한 상관관계가 없다는 연구 결과가 있다.17)
이에 본 연구는 난청의 유병률이 증가하는 40대 이상의 한국인에 서, 흡연이 난청에 영향을 주는지 알아보았으며 흡연량에 따라 난청 위험이 증가하는지 알아보고자 시행하였다.
방 법
1. 연구 대상
본 연구는 제6기 1차년도(2013년)에 시행한 국민건강영양조사 자 료를 기반으로 시행하였다. 조사에 참여하였던 40세 이상 남녀 4,212 명에서 청력검사 및 설문조사에 참여자 중 보청기 및 인공 와우 사 용자를 제외하였으며, 항목별로 결측치 및 무응답을 제외하여 최종 적으로 3,249명(남성 1,408명, 여성 1,841명)을 본 연구 대상에 포함하 였다.
2. 변수의 정의 1) 흡연
흡연은 설문지를 통해 조사하였으며 평생 흡연 여부를 기준으로 흡연하지 않았거나 100개비 미만인 경우 비흡연군, 100개비 이상인 경우를 흡연군으로 나누었다.
2) 난청
난청은 국민건강영양조사에서 시행한 순음 청력검사 결과에서 0.5, 1, 2, 3 kHz 각 주파수의 순음이 들리는 최소 역치의 평균값이 25 dB 이상인 것을 난청으로 정의하여 일측성 또는 양측성 난청을 가 지고 있는 사람을 난청군으로 분류하였다.
3) 기타 변수
음주 형태는 평생 음주 경험이 없는 경우와 있는 경우로 나누었
다. 규칙적 운동은 격렬한 신체 활동(평소보다 몸이 매우 힘들거나 숨이 많이 가쁜 정도)을 1회 10분 이상, 1일 총 20분 이상 주 3일 이상 또는 중등도 신체 활동(몸이 조금 힘들거나 숨이 약간 가쁜 정도의 강도)을 1회 30분 이상, 주 5일 이상 실천하는 경우로 정의하였다. 고 혈압은 수축기 혈압 140 mmHg 이상 또는 이완기 90 mmHg 이상, 고 혈압 약을 복용 중이거나, 의사에서 진단받은 경우로 정의하였다. 당 뇨는 공복혈당 126 mg/dL 이상, 의사 진단을 받았거나 혈당강하제를 복용하거나, 인슐린 주사를 투여 받고 있는 경우로 정의하였다. 교육 수준은 중학교 졸업 이하, 고등학교 졸업, 대학교 졸업 이상으로 나 누었다. 소음 노출 여부는 설문을 통해 기계음 등 소음이 큰 곳에서 3개월 이상 근무 경험이 있거나, 직업 이외에 주당 5시간 이상 큰 소 음에 노출된 적이 있거나 총소리나 폭발음 등 큰 소음에 순간적 노 출이 있었는지 여부에 따라 나누었다.
3. 통계 분석
대상자의 기본 특성은 성별에 따라 t 검정과 카이제곱검정을 이용 하여 분석하였고 평균과 표준편차, 비율로 표시하였다.
비흡연과 흡연군으로 분류한 후 난청의 유병률을 카이제곱검정 을 이용하여 분석하였으며 난청에 영향을 줄 수 있는 연령, 음주 여 부, 규칙적 운동 여부, 교육수준, 당뇨, 고혈압, 소음 노출 여부를 보정
Original Article
Korean Journal of Family Practice
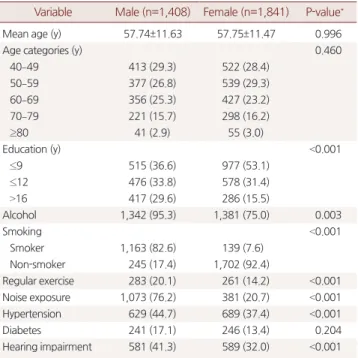
Table 1. Baseline characteristics of study population according to sex from KNHANES 2013
Variable Male (n=1,408) Female (n=1,841) P-value*
Mean age (y) 57.74±11.63 57.75±11.47 0.996
Age categories (y) 0.460
40–49 413 (29.3) 522 (28.4)
50–59 377 (26.8) 539 (29.3)
60–69 356 (25.3) 427 (23.2)
70–79 221 (15.7) 298 (16.2)
≥80 41 (2.9) 55 (3.0)
Education (y) <0.001
≤9 515 (36.6) 977 (53.1)
≤12 476 (33.8) 578 (31.4)
>16 417 (29.6) 286 (15.5)
Alcohol 1,342 (95.3) 1,381 (75.0) 0.003
Smoking <0.001
Smoker 1,163 (82.6) 139 (7.6)
Non-smoker 245 (17.4) 1,702 (92.4)
Regular exercise 283 (20.1) 261 (14.2) <0.001 Noise exposure 1,073 (76.2) 381 (20.7) <0.001
Hypertension 629 (44.7) 689 (37.4) <0.001
Diabetes 241 (17.1) 246 (13.4) 0.204
Hearing impairment 581 (41.3) 589 (32.0) <0.001 Data are presented as mean±standard error or number (%).
KNHANES, Korean National Health and Nutrition Examination Survey.
*P-values were obtained by Student’s t-test or Chi-square test.
Yu Rim Lee, et al. Effect of Cigarette Smoking on Hearing Impairment in Korean Adults Over 40 Years-Old
Korean Journal of Family Practice
KJFP
한 후 로지스틱 회귀분석을 시행하였다.
연령별, 성별에 따라 흡연에 따른 난청의 영향에 차이가 있는지 알 아보기 위하여 각각의 분석은 연령별, 성별 분석을 시행하였다. 또한 흡연량에 따라 위험이 증가하는지 알아보고자 하루 평균 흡연량에 따른 분석을 시행하였다. 모든 분석은 SPSS version 19.0 (IBM Co., Ar- monk, NY, USA)을 이용하였으며 P-value가 0.05 미만일 때 통계학적 으로 의미 있다고 판단하였다.
결 과
1. 연구 대상자의 일반적인 특성
Table 1의 결과를 보면 대상 인구 3,249명 중 남성 1,408명(43.3%) 여 성 1,841명(56.7%)이었고, 평균 나이는 각각 남성 57.7세, 여성 57.8세였 다. 흡연자는 남성 82.6%, 여성 7.6%로 나타나 남성 흡연군의 비율이 유의하게 높게 나타났다(P<0.001). 난청은 남성 41.3%, 여성 32.0%로 나타나 남성에서 난청이 유의하게 높게 나타났다(P<0.001). 규칙적인
운동 여부, 음주 여부, 소음 노출, 고혈압 여부, 교육수준은 남성에서 유의하게 높았으며(P<0.001) 당뇨 유병률은 남녀 간 차이가 없는 것 으로 나타났다.
2. 흡연과 난청
전체 대상자에서 흡연 여부에 따라 난청의 유병률을 살펴본 결과 비흡연군에서 32.5%, 흡연군에서 41.2%로 나타났으며 연령별 분석에 서는 50–69세 흡연군에서 유의하게 난청 유병률이 증가하는 것으로 나타났다(P<0.05) (Figure 1).
Table 2의 결과를 살펴보면 흡연군에서 교차비 1.46 (95% confi- dence interval [CI], 1.260-1.685)로 난청 발병 위험이 유의하게 높은 것 으로 나타났다(P<0.05). 남녀별 흡연에 따른 난청의 유병률을 살펴본 결과 남성 흡연군에서 교차비 1.34 (95% CI, 1.007–1.786)으로 높게 나 타났으나(P<0.05) 여성에서는 유의한 차이가 없었다. 연령별 분석에 서는 50대에서 교차비 2.27 (95% CI, 1.659–3.118), 60대에서 1.69 (1.268–2.255)로 난청의 위험이 유의하게 높게 나타났다(P<0.05). 남성 의 연령별 분석에서는 50대에서 교차비 2.04 (95% CI, 1.040–4.011) 60 대에서 1.90 (1.098–3.274)로 유의하게 나타났으나(P<0.05) 여성에서는 유의한 결과가 없었다. 70세 이상 여성 흡연자는 모두 난청으로 나타 났다.
Figure 1. The prevalence of hearing impairment according to smoking status.
*P-value<0.05.
40 49 y 100
80
60
40
20
%
0
Non-smoker Smoker
50 59* y 60 69* y 70 79 y >80 y 11.8
8.4
31.4
16.7
59.0
46.0
77.7
71.7
90.6
87.7
Table 2. The unadjusted odds ratio between smoking and hearing im- pairment according to age
Age (y) Total Men Women
Overall 1.46 (1.260–1.685)* 1.34 (1.007–1.786)* 0.95 (0.653–1.378) 40–49 1.45 (0.943–2.232) 1.06 (0.491–2.274) 0.50 (0.114–2.096) 50–59 2.27 (1.659–3.118)* 2.04 (1.040–4.011)* 0.30 (0.071–1.282) 60–69 1.69 (1.268–2.255)* 1.90 (1.098–3.274)* 1.32 (0.632–2.784) 70–79 1.37 (0.906–2.072) 0.86 (0.385–1.962) N/A ≥80 2.60 (0.509–13.192) 5.17 (0.604–44.184) N/A Values are presented as odds ratio (95% confidence interval). Reference is nev- er smokers. Odds ratios and 95% confidence intervals were obtained by Chi– square test.
N/A, not available value.
*P-value<0.05
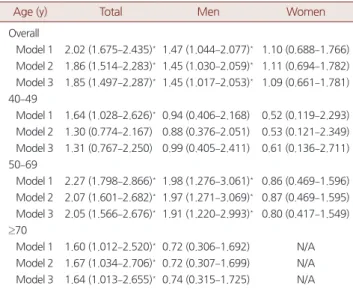
Table 3. The adjusted odds ratio between smoking and hearing im- pairment according to age
Age (y) Total Men Women
Overall
Model 1 2.02 (1.675–2.435)*1.47 (1.044–2.077)* 1.10 (0.688–1.766) Model 2 1.86 (1.514–2.283)*1.45 (1.030–2.059)* 1.11 (0.694–1.782) Model 3 1.85 (1.497–2.287)*1.45 (1.017–2.053)* 1.09 (0.661–1.781) 40–49
Model 1 1.64 (1.028–2.626)*0.94 (0.406–2.168) 0.52 (0.119–2.293) Model 2 1.30 (0.774–2.167) 0.88 (0.376–2.051) 0.53 (0.121–2.349) Model 3 1.31 (0.767–2.250) 0.99 (0.405–2.411) 0.61 (0.136–2.711) 50–69
Model 1 2.27 (1.798–2.866)*1.98 (1.276–3.061)* 0.86 (0.469–1.596) Model 2 2.07 (1.601–2.682)*1.97 (1.271–3.069)* 0.87 (0.469–1.595) Model 3 2.05 (1.566–2.676)*1.91 (1.220–2.993)* 0.80 (0.417–1.549) ≥70
Model 1 1.60 (1.012–2.520)*0.72 (0.306–1.692) N/A Model 2 1.67 (1.034–2.706)*0.72 (0.307–1.699) N/A Model 3 1.64 (1.013–2.655)*0.74 (0.315–1.725) N/A Values are presented as odds ratio (95% confidence interval). Reference is nev- er smokers. Odds ratios and 95% confidence intervals were obtained by multi- ple logistic regression analysis. Model 1 was adjusted for age, alcohol, diabetes, hypertension, regular exercise, education. Model 2 was adjusted for noise expo- sure, in addition to the factors of Model 1. Model 3 excluded cases who had his- tory of otitis media, in addition to the Model 2.
N/A, not available value.
*P-value<0.05.
이유림 외. 40세 이상 한국 성인에서 흡연과 난청의 연관성 Korean Journal of Family Practice
KJFP
Table 3은 난청 발생에 영향을 미칠 수 있는 연령, 음주 여부, 규칙 적 운동 여부, 당뇨 유병 여부, 고혈압 유병 여부, 교육수준, 소음 노 출 여부를 보정하여 분석한 교차비를 나타낸 것이다. 연령, 음주 여 부, 당뇨 유병 여부, 고혈압 유병 여부, 규칙적 운동 여부, 교육수준 보 정 모델(Model 1)과 소음 노출 여부를 추가 보정한 모델(Model 2), 추 가로 중이염 기왕력이 있는 군을 제외하고 분석(Model 3)을 시행하 였다. 연령별, 성별 분석을 함께 시행하였으며 연령그룹은 상관분석 에서의 유의한 결과를 토대로 40–49세, 50–69세, 70세 이상의 세 그 룹으로 분류하였다.
분석 결과 세 가지 모델에서 모두 난청과 흡연이 유의한 영향이 있 었다(P<0.05). 연령별 분석에서 40–49세는 Model 1에서 50–69세 그룹 과 70세 이상 그룹은 세 가지 모델 모두에서 유의한 결과를 보였다 (P<0.05). 특히 50–69세 그룹에서 교차비 2.27 (95% CI, 1.798–2.866)으 로 위험이 가장 높게 증가하는 것으로 나타났다(P<0.05). 남성에서도 세 가지 모델에서 유의한 연관성이 있다고 나타났으며, 50–69세에서 교차비 1.98 (95% CI, 1.276–3.061)로 가장 높이 나타냈다 (P<0.05). 여 성에서는 모두 유의하지 않은 것으로 나타났다.
Table 4는 흡연량과 난청 위험의 연관성을 알아보기 위해 하루 평 균 흡연량에 따라 0개비 이하(비흡연군), 1–10개비, 11–20개비, 20개비 초과 그룹으로 나누어 연령, 음주 여부, 당뇨 유병 여부, 고혈압 유병 여부, 규칙적 운동 여부, 교육수준, 소음 노출을 보정하여 로지스틱 회귀분석을 시행한 결과이다.
비흡연군과 비교하여 1–10개비 그룹은 교차비 1.69 (95% CI, 1.301–
2.200), 11–20개비 그룹은 1.90 (95% CI, 1.485–2.438), 20개비 초과 그룹 은 2.40 (95% CI, 1.582–3.645)로 유의한 증가를 보였다(P<0.05). 남성에
서는 20개비를 초과해서 피우는 그룹에서 교차비가 1.73 (95% CI, 1.053–2.838)로 유의한 증가를 보였다(P<0.05). 여성에서는 모두 유의 하지 않은 것으로 나타났다.
고 찰
이전에 여러 연구에서 난청에 중요한 인자로 나이를 생각해왔다.
연령 증가에 따른 난청의 기전은 신경섬유(neural fiber), 혈관조(stria vascularis), 내이와 외이 모세포와 관련되어 생기며 나이와 함께 난청 위험인자 알려진 요인들과 상승작용을 하며 달팽이관 혈액 공급을 감소시키는 것으로 알려져 있다. 난청은 주로 40대부터 고주파 영역 에서 나타나기 시작하여 50–60대에 회화 영역을 침범하기 시작한 다.18)
흡연이 청력에 영향을 주는 주요한 기전은 미세혈관 장애로 알려 져 있다. 니코틴으로 인한 혈관수축과 일산화탄소가 유발하는 저산 소증으로 혈액순환에 악영향을 미치며 또한 죽상동맥경화증 유발 로 내이의 혈액 순환을 감소시킨다.19) 말초 혈관 질환의 강력한 위험 인자로 흡연과 나이가 있으며 특히 50세 이상에서 흡연, 당뇨와 같은 심혈관 위험인자가 있을 시 혈관 질환이 증가한다.20)
본 연구에서도 나이에 따라 난청의 발생률이 큰 폭으로 증가하는 결과를 보였으며 회화 영역 난청이 본격적으로 시작하는 50–69세에 서 위험이 가장 크게 나타났다. 특히 50–69세 남성에서는 평균 흡연 량이 최대를 이루고 있으며 이외에 청력에 영향을 줄 수 있는 음주 량, 직업적 소음 노출, 만성질환 유병, 스트레스 등이 증가하면서 상 승효과를 내고 이에 따라 흡연에 따른 난청 위험이 가장 증가하는 것으로 생각된다.
흡연량 증가에 따른 난청 증가는 여러 연구들에서도 나타나고 있
다.21,22) 본 연구에서도 하루 평균 흡연량이 증가함에 따라 난청의 위
험도가 증가하는 것으로 나타나고 있다.
남녀별 분석에서는 여성의 흡연이 난청에 유의한 연관성이 없는 것으로 나타났으나, 흡연이 남성보다 여성에서 혈관에 큰 영향을 준 다는 연구들이 있다. 흡연 여성에서 남성보다 관상동맥 위험이 증가 한다는 연구 결과가 있었으며,23) 특히 경구 피임약을 복용하는 여성 이 흡연 시 상승 효과로 인해 심혈관 위험이 크게 증가시키는 것으로 나타났다.24) 또한 2013년 국내 성인 흡연율은 남성 41.4%, 여성 5.7%로 경제협력개발기구(Organization for Economic Cooperation and Devel- opment, OECD) 국가 중 남성은 가장 높고 여성은 가장 낮은 것으로 나타났다. 남성의 하루 평균 흡연량은 여성의 약 2배이며, 여성에서 는 상대적으로 저니코틴과 저타르 함량 담배를 선호하고 있어 남녀 의 흡연자 비율, 흡연량, 선호도에 많은 차이가 있다.25,26) 아울러 본 연 Table 4. The adjusted odds ratio between smoking and hearing im-
pairment according to daily smoking dose
Model Total Men Women
Model 1 (cig/d)
0 1 1 1
1–10 1.79 (1.390–2.311)* 1.44 (0.965–2.133) 1.06 (0.636–1.799) 11–20 2.07 (1.647–2.604)* 1.43 (0.993–2.069) 1.15 (0.363–3.619) >20 2.64 (1.764–3.954)* 1.76 (1.073–2.872)* N/A Model 2 (cig/d)
0 1 1 1
1–10 1.69 (1.301–2.200)* 1.43 (0.958–2.120) 1.06 (0.634–1.780) 11–20 1.90 (1.485–2.438)* 1.42 (0.980–2.051) 1.15 (0.353–3.648) >20 2.40 (1.582–3.645)* 1.73 (1.053–2.838)* N/A Values are presented as odds ratio (95% confidence interval). Odds ratios and 95% confidence intervals were obtained by multiple logistic regression analysis.
Model 1 was adjusted for age, alcohol, diabetes, hypertension, regular exercise, education. Model 2 was adjusted for noise exposure, in addition to the factors of Model 1.
Cig, cigarettes; N/A, not available value.
*P-value <0.05
Yu Rim Lee, et al. Effect of Cigarette Smoking on Hearing Impairment in Korean Adults Over 40 Years-Old
Korean Journal of Family Practice
KJFP
구에서 흡연 여부가 자기 보고형 설문방식으로 이루어졌기 때문에 여성에서 흡연을 과소 보고를 했을 가능성도 존재한다. 최근 19세 이 상 성인에서 자가보고 흡연율과 소변 내 코티닌 성분 측정을 통한 실 제 흡연을 비교한 연구에 따르면 여성이 스스로 보고한 흡연율은 7.1%였으나 소변 내 코티닌 검사에서는 18.2%로 높아진 것으로 나타 났다.27)
따라서 본 연구에서 여성에서 흡연과 난청이 유의한 관계를 보이 지 않고 있으나 여성에서 흡연이 난청에 영향을 줄 수 있을 것으로 생각된다.
본 연구의 제한점으로 첫째, 본 연구는 단면연구이기 때문에 흡연 과 난청의 통계적 연관성은 보일 수 있으나 시간적 선후관계는 분명 하지 않을 수 있다. 둘째, 흡연 및 운동, 소음 노출 등의 일부 변수를 설문을 바탕으로 하였으므로 개인의 주관적 판단과 기억 오류가 있 을 수 있다. 셋째, 난청에 영향을 줄 수 있는 약물 복용에 관한 자료 가 없어 이독성 약물 영향을 배제할 수가 없었다. 이독성을 가지는 대표적인 약물로 아미노글리코사이드 계열의 항생제, 푸로세마이 드 같은 고리 이뇨제, 시스플라틴 같은 항암제 등이 있다. 마지막으 로 난청 여부 판별하는 방법이 연구마다 상이하여 다른 연구와 결 과를 직접적으로 비교하기에 어려움이 있다. 본 연구에서는 0.5, 1, 2, 3 kHz의 역치값의 평균 낸 4분법으로 난청 여부를 판별하였다. 앞으 로 흡연과 난청의 인과관계를 확실히 규명하기 위해서는 전향적인 추적 관찰 연구가 필요하다.
이번 연구는 국내에서 대표성을 가진 대규모 인구 집단을 대상으 로 하였고 성별, 연령대별 흡연과 관련된 난청의 위험도의 차이가 있 음을 보여주었으며 흡연량에 따른 난청 위험의 증가를 보여 흡연과 난청 간의 용량 반응 관계를 보여준 연구라는 것에 의의가 있다.
요 약
연구배경:
이전 여러 연구에서 흡연과 난청에 관한 다양한 연구들 이 제시되고 있다. 본 연구에서는 난청의 발생이 증가하는 40세 이상 성인 남녀에서 흡연에 따른 난청의 영향을 분석하였다.방법:
국내에서 시행된 제6기 국민건강영양조사에 참여한 40세 이 상 성인을 대상으로 하였다. 순음 청력검사를 통해 난청 여부를 정의 하였다. 흡연 여부는 설문지를 통해 비흡연군과 흡연군으로 분리하 였다. 흡연이 난청에 주는 영향을 파악하기 위하여 카이제곱검정 및 로지스틱 회귀분석을 이용하였다. 분석은 연령별, 성별 분석을 시행 하였으며 흡연량에 따라 난청의 위험이 증가하는지 알아보았다.결과:
국내 40세 이상 성인에서 흡연과 난청이 유의한 관계가 있는 것으로 나타났다. 남자에서 흡연과 난청에 유의한 상관관계를 보였으나 여자에서는 유의하지 않은 것으로 나타났다. 연령별 분석에서 는 50–69세에서 유의한 결과를 보였다. 나이, 음주, 고혈압, 당뇨, 운 동 여부, 교육수준, 소음 노출 여부를 보정하여 분석한 경우에도 흡 연에 따라 난청의 위험이 증가하는 것으로 나타났다. 흡연량에 따른 분석결과에서 흡연량이 증가함에 따라 난청 위험도가 증가하는 것 으로 나타났다.
결론:
한국 40세 이상 성인에서 흡연이 난청의 위험을 유의하게 높 이고 있으며, 특히 50–69세에서 난청의 위험이 가장 높으며 흡연량이 증가할수록 위험도가 증가한다.중심단어:
난청; 흡연; 나이; 성별REFERENCES
1. Lin FR, Niparko JK, Ferrucci L. Hearing loss prevalence in the United States.
Arch Intern Med 2011; 171: 1851-2.
2. Korea Health Statistics 2012: Korea National Health and Nutrition Exami- nation Survey (KNHANES V-3) [Internet]. Cheongju: Korea Centers for Disease Control and Prevention; 2012. [cited 2012 Dec]. Available from:
https://Knhanes.cdc.go.kr.
3. Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences by demographic characteristics among US adults: data from the National Health and Nutrition Examination Survey, 1999-2004. Arch Intern Med 2008; 168: 1522-30.
4. Cruickshanks KJ, Tweed TS, Wiley TL, Klein BE, Klein R, Chappell R, et al.
The 5-year incidence and progression of hearing loss: the epidemiology of hearing loss study. Arch Otolaryngol Head Neck Surg 2003; 129: 1041-6.
5. Sousa CS, Castro Júnior Nd, Larsson EJ, Ching TH. Risk factors for presby- cusis in a socio-economic middle-class sample. Braz J Otorhinolaryngol 2009; 75: 530-6.
6. Agrawal Y, Platz EA, Niparko JK. Risk factors for hearing loss in US adults:
data from the National Health and Nutrition Examination Survey, 1999 to 2002. Otol Neurotol 2009; 30: 139-45.
7. Noorhassim I, Rampal KG. Multiplicative effect of smoking and age on hearing impairment. Am J Otolaryngol 1998; 19: 240-3.
8. Gates GA, Cobb JL, D’Agostino RB, Wolf PA. The relation of hearing in the elderly to the presence of cardiovascular disease and cardiovascular risk fac- tors. Arch Otolaryngol Head Neck Surg 1993; 119: 156-61.
9. Jung SP, Kim SY, Lee TY, Cho YC, Lee DB. The correlation of cardiovascular risk factors and hearing loss. Korean J Occup Environ Med 1998; 10: 189- 202.
10. Nakanishi N, Okamoto M, Nakamura K, Suzuki K, Tatara K. Cigarette smoking and risk for hearing impairment: a longitudinal study in Japanese male office workers. J Occup Environ Med 2000; 42: 1045-9.
11. Karlsmose B, Lauritzen T, Engberg M, Parving A. A five-year longitudinal study of hearing in a Danish rural population aged 31-50 years. Br J Audiol 2000; 34: 47-55.
12. Gopinath B, Flood VM, McMahon CM, Burlutsky G, Smith W, Mitchell P.
The effects of smoking and alcohol consumption on age-related hearing
이유림 외. 40세 이상 한국 성인에서 흡연과 난청의 연관성 Korean Journal of Family Practice
KJFP
loss: the Blue Mountains Hearing Study. Ear Hear 2010; 31: 277-82.
13. Ward WD. Endogenous factors related to susceptibility to damage from noise. Occup Med 1995; 10: 561-75.
14. Brant LJ, Gordon-Salant S, Pearson JD, Klein LL, Morrell CH, Metter EJ, et al. Risk factors related to age-associated hearing loss in the speech frequen- cies. J Am Acad Audiol 1996; 7: 152-60.
15. Chang J, Ryou N, Jun HJ, Hwang SY, Song JJ, Chae SW. Effect of cigarette smoking and passive smoking on hearing impairment: data from a popula- tion-based study. PLoS One 2016; 11: e0146608.
16. Sung JH, Sim CS, Lee CR, Yoo CI, Lee H, Kim Y, et al. Relationship of ciga- rette smoking and hearing loss in workers exposed to occupational noise.
Ann Occup Environ Med 2013; 25: 8.
17. Hong JW, Jeon JH, Ku CR, Noh JH, Yoo HJ, Kim DJ. The prevalence and fac- tors associated with hearing impairment in the Korean adults: the 2010- 2012 Korea National Health and Nutrition Examination Survey (observa- tional study). Medicine (Baltimore) 2015; 94: e611.
18. Kim JS, Yeh MH, Chun BY, Woo KH, Kang YS, Kim KY, et al. Effect of ciga- reet smoking on air-conduction hearing threshold level in adult men. Kore- an J Prev Med 1998; 31: 285-92.
19. Matschke RG. Smoking habits in patients with sudden hearing loss. Prelimi- nary results. Acta Otolaryngol Suppl 1990; 476: 69-73.
20. Shammas NW. Epidemiology, classification, and modifiable risk factors of peripheral arterial disease. Vasc Health Risk Manag 2007; 3: 229-34.
21. Dawes P, Cruickshanks KJ, Moore DR, Edmondson-Jones M, McCormack A, Fortnum H, et al. Cigarette smoking, passive smoking, alcohol consump- tion, and hearing loss. J Assoc Res Otolaryngol 2014; 15: 663-74.
22. Cruickshanks KJ, Klein R, Klein BE, Wiley TL, Nondahl DM, Tweed TS.
Cigarette smoking and hearing loss: the epidemiology of hearing loss study.
JAMA 1998; 279: 1715-9.
23. Huxley RR, Woodward M. Cigarette smoking as a risk factor for coronary heart disease in women compared with men: a systematic review and meta- analysis of prospective cohort studies. Lancet 2011; 378: 1297-305.
24. Farley TM, Meirik O, Chang CL, Poulter NR. Combined oral contracep- tives, smoking, and cardiovascular risk. J Epidemiol Community Health 1998; 52: 775-85.
25. National Cancer Information Center [Internet]. Ilsan: National Cancer Center; 2016. [cited 2016 Mar 8]. Available from: http://www.cancer.go.kr/
mbs/cancer/jsp/album/gallery.jsp?boardType=02&boardId=31817&listTy pe=02&boardSeq=14037494&mcategoryId=&id=cancer_050207000000
&spage=1#.
26. Suh KH. Updates in the smoking and smoking cessation of Korean women.
Korean J Health Psychol 2007; 12: 695-713.
27. Park MB, Kim CB, Nam EW, Hong KS. Does South Korea have hidden fe- male smokers: discrepancies in smoking rates between self-reports and uri- nary cotinine level. BMC Womens Health 2014; 14: 156.