댄디 워커 증후군이 동반된 증후성 신경피부멜라닌증
조선대학교 의학전문대학원 소아과학교실
고영권・주정연・이성찬・노영일
An earlier version of this article was presented at the 64th annual fall meeting of the Korean Pediatric Society, 2014.
This study was supported by research fund from Chosun University, 2013.
Submitted: 24 August, 2016 Revised: 13 September, 2016 Accepted: 13 September, 2016 Correspondence to Young Il Rho, MD
Department of Pediatrics, Chosun University Hospital, 365, Pilmun-daero, Dong-gu, Gwangju 61453, Korea Tel: + 82-62-220-3036, Fax: +82-62-227-2904 E-mail: [email protected]
Symptomatic Neurocutaneous Melanosis Associated with Dandy Walker Complex
Neurocutaneous melanosis (NCM) is a rare nonheritable congenital phakomatosis.
NCM is characterized by large or multiple (>3) congenital nevi that are associated with benign and/or malignant melanocytic tumors of the leptomeninges. Approxi- mately 10% of symptomatic patients with NCM have associated Dandy Walker complex (DWC), which seems to have an extremely poor prognosis. We report the case of a 7 year-old patient with multiple congenital NCM associated with DWC, who experienced a transient improvement in neurological symptoms including mental status and hemiparesis after intravenous immunoglobulin (IVIG) therapy. We suggest that the administration of IVIG may play a role in the treatment of symp- tomatic NCM.
Key Words: Neurocutaneous melanosis, Dandy Walker complex, Intravenous immu-
noglobulins
Young Kwon Koh, MD, Jung Yeon Joo, MD, Sung Chan Lee, MD, Young Il Rho, MD
Department of Pediatrics, School of Medicine, Chosun University, Gwangju, Korea
Copyright © 2016 by The Korean Child Neurology Society
http://www.cns.or.kr
Introduction
Neurocutaneous melanosis (NCM) is a rare nonheritable congenital phakoma
tosis characterized by giant or multiple (>3) nonmalignant melanocytic nevi that are associated with benign and/or malignant melanocytic tumors in the central nervous system (CNS)1). To date, approximately 100 cases of NCM have been reported in the literature; 10% of symptomatic NCM cases were associated with Dandy Walker complex (DWC)29). Symptoms of NCM include papilledema, cranial palsies, headaches, vomiting, and seizures. The patients that manifest neurological symptoms experienced rapid neurological deterioration and death by 4 years of age in the majority of reported cases. We report the case of a 7 yearold patient with multiple congenital NCM associated with DWC. She experienced a transient improvement in neurological symptoms including mental status, facial nerve palsy, and hemiparesis after repeated intravenous immuno
globulin (IVIG) therapy. In addition, we discuss the management and prognosis of NCM with DWC in the light of new data from the recent literature. We suggest that the early administration of intravenous immunoglobulin (IVIG) may have a role to play in the treatment of symptomatic NCM.
Case report
A 7year old girl presented to the Chosun University Hospital emergency department with an episode of seizure. She had no previous history of seizures and her developmental history had previously been normal. There was no family history of epilepsy or neurocutaneous disease. Her head circumference was within normal limits. Her developmental state was normal. She had multiple, small to mediumsized black pigmented nevi on her scalp, chest, abdomen, and extremities since birth (Fig. 1).
At that time, her focal dyscognitive seizure had lasted for 40 minutes. We administrated lorazepam (0.1 mg/kg) twice, but the seizure continued. The seizure stopped after a loading dose of phenytoin. Results of routine laboratory tests and cerebrospinal fluid (CSF) examination were normal. Electroencephalography showed diffuse low amplitude slow delta activity background on the right hemisphere intermixed with frequent sharp wave dis
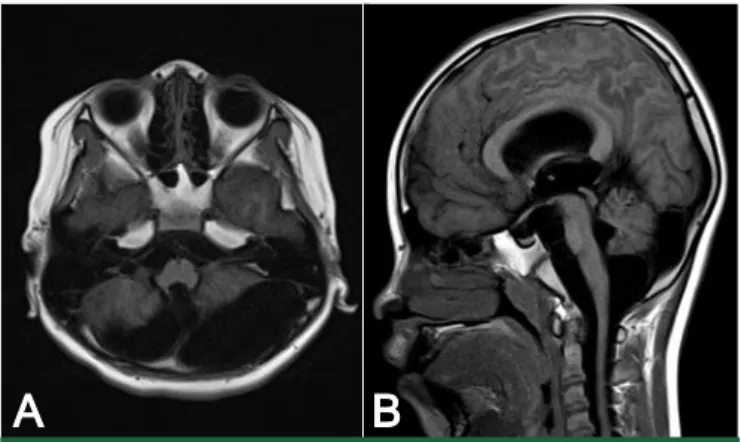
charges from the right central area. A magnetic resonance imaging (MRI) scan of the brain showed a large cyst in the posterior fossa with cerebellar vermis hypoplasia and slightly enlarged lateral ventricles bilaterally (Fig. 2). Histological
examination of a nevus showed melanocytic cells in dermis and no cytologic atypia. There was no indication of malignant mela
noma (Fig. 3). She was diagnosed with NCM with DWC and commenced on topiramate for her seizures. She developed headache and vomiting on hospital day 6. On hospital day 28, she underwent a cystoperitoneal shunt operation because of hydrocephalus worsening. Her headache and vomiting subse
quently subsided.
On hospital day 36, she abruptly developed leftsided hemi
paresis and aphasia. Her deep tendon reflexes of left knee and left biceps were hyperreflexive. The followup CSF examination at that time revealed an opening pressure of 15 cmH2O, white blood cell (WBC) count 6/mm3, protein 245.3 mg/dL, glucose 21.9 mg/dL and proliferation of melanocytes without evidence of malignancy. A repeat brain MRI showed no changes beyond an improvement in the hydrocephalus. She received methylpredni
solone pulse therapy (30 mg/kg/day, for 3 days), but there was no improvement in her symptoms. She was then treated with IVIG (1 g/kg/day, for 2 days), whereupon her hemiparesis and aphasia improved. The motor tone on her left side improved
Fig. 1. Diffuse black pigmented nevi of various sizes on the whole body.
A B
Fig. 2. Initial T1-weighted brain MRI image. T1-weighted brain MRI (A)
axial, (B) sagittal images show a large cyst in the posterior fossa and cerebellar vermis hypoplasia.
A B
Fig. 3. Pathological morphology features of the skin biopsy specimen. (A) In the low power field,
melanocytic nevus cells are arranged in the dermis (H&E stain, x100), (B) In the high power field,
melanocytic nevus cells without cytologic atypia are arranged in the dermis (H&E stain, x400).
from grade 2 to grade 4.
At 3 months after symptom onset, she presented to the emer
gency department with generalized tonic seizures that lasted for 1 minute. Her mental state was stupor. CSF examination at that time revealed an opening pressure of 14 cmH2O, WBC 7/mm3, protein 107.6 mg/dL, glucose 37.8 mg/dL and proliferation of melanocytes with no evidence of malignancy. The followup brain MRI showed extensive enhancement of the leptomeninges on both cerebral hemispheres (Fig. 4A) and a 0.8×1.0 cm sized subdural tumor in the right parietal lobe (Fig. 4B). She was treated with IVIG (1 g/kg/day, for 2 days); thereafter her mental status was improved.
At 5 months after the onset of her symptoms, she presented to the emergency department in a comatose state. The follow
up brain MRI showed a 1.5×2.0 cm sized hyperintense subdural mass with intracranial hemorrhage (ICH) on the right fronto
temporal lobe (Fig. 4C) and a 2.2×2.2 cm sized hyperintense
subdural mass with ICH on the right parietal lobe (Fig. 4D).
Tumor resection and craniotomy were performed. Histological examination of the brain tumor indicated malignant melanoma (Fig. 5). She died shortly after at 6.5 months after her initial presentation.
Discussion
NCM is an extremely rare disease that combines abnormalities of the skin and CNS. It was first described by Rokitansky10) in 1861. The criteria for the diagnosis of this condition was proposed by Fox in 196411) and later, by Kadonaga and Frieden in 19911). Congenital melanocytic nevi (CMN) are usually classified in three groups according to their size; small (<15 mm in diameter), medium (15199 mm in diameter), and large or giant CMN (>200 mm in diameter, GCMN). The prevalence of
A B
D C
*
Fig. 4. Three months after symptom onset, the contrast-enhanced T1 weighted (A) axial and (B)
sagittal images show extensive enhancement of the leptomeninges on both cerebral hemispheres and
0.8 x1.0 cm sized subdural tumor in the right parietal lobe(arrow). Five months after symtom onset, (C)
the T2 weighted axial image shows a 1.5x1.5 cm hyperintense subdural mass with hemorrhage on the
right frontotemporal area(arrowhead) and (D) a 2.2x2.2 cm hyperintense subdural mass with
hemorrhage on the right parietal lobe (star).
GCMN is estimated to be 1 in 500,000. The diagnostic criteria of NCM are as follows; (1) large or multiple congenital nevi in asso
ciation with meningeal melanosis or melanoma, (2) no evidence of cutaneous melanoma, except in patients in whom the exami
ned areas of the meningeal lesions were historically benign, (3) no evidence of cutaneous melanoma, except in patients in whom the examined areas of the cutaneous lesions were histo
rically benign1).
The pathogenesis of NCM is not sufficiently clear, but it is thought to be a phakomatosis caused by congenital dysplasia of the neural ectoderm in the developing embryo, particularly in the neural crest. This results in the excessive proliferation of melanocytes in the skin and the leptomeninges12).
Fewer than 100 cases of symptomatic NCM have been repor
ted in the literature. Approximately 10% of these were associated with DWC29) which is characterized by ventricular and cerebel
lar dysgenesis, and an enlarged posterior fossa with or without hydrocephalus. The cutaneous lesions of NCM are usually recognized at birth, although most patients remain otherwise asymptomatic. In cases of symptomatic NCM, neurological manifestations usually develop in the first 3 years of life1). The neurological symptoms could be related to benign extensive leptomeningeal melanocytic proliferation or to primary malig
nant melanoma of the CNS. The initial neurological symptoms
are broad and nonspecific. Twothirds of patients present with symptoms of increased intracranial pressure related to hydro
cephalus, which includes headache, nausea, vomiting, partial or generalized seizures, cranial nerve palsies and increased head circumference. The hydrocephalus may be related to DWC or may be caused by flow obstruction and decreased absorption of CSF due to arachnoid villi infiltration2, 13).
When NCM is clinically suspected, MRI is the radiological modality of choice for investigation. However, definitive diagno
sis still relies on histological data obtained by means of biopsy.
The meningeal disease of NCM is most frequently described as an increased signal intensity on unenhanced T1weighted images or decreased signal intensity on T2weighted sequen
ces6,12,14,15). Histological features of cutaneous lesions are similar to that of congenital nevi found in the absence of NCM. Neuro
pathological examination shows dark leptomeningeal infiltration on the basal surface of brain and the rostral the aspect of brain stem. This leptomeningeal proliferation of melanocytes is found more prominently on the inferior surface of the cerebellum, frontal, temporal, and parietal lobes along with the ventral aspect of the brain and upper cervical cord1,16). The associa tion of NCM with DWC represents a phenotypic marker for more profound melanotic infiltration of the leptomeninges, which increases the risk of malignant transformation8,12).
A B
D C
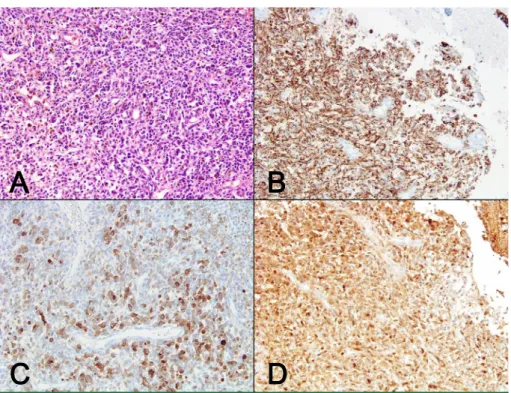
Fig. 5. Pathological morphology features and immunohistochemistry results of the brain biopsy speci-
men (x200). (A) The hematoxylin and eosin-stained section shows malignant cells arranged in a vague
organoid pattern with brown pigmentation. Immunohistochemical staining in the tumor cells for (B)
HMB45, (C) melan-A and (D) S-100 show cytoplasmic positivity.
In the present case, the onset of neurological symptoms at 7 years old was unusually late. Brain MRI showed a large sized cystic mass in the posterior fossa with cerebellar vermis hypo
plasia, bilaterally enlarged lateral ventricles and extensive enhan
cement of the leptomeninges on both cerebral hemis pheres.
Histological examination of a nevus showed melano cytic cells in the dermis and no cytologic atypia which was no evidence of malignant melanoma. Brain biopsy specimen showed that ma
lignant cells were arranged in a vague organoid pattern and im
munoreactivity for glial acidic fibrillary protein (GFAP) were ne
gative, but homatropinemethobromide (HMB)45, MelanA, and S100 were positive, which indicated histologically malignant melanoma. However, it is difficult to diagnose malig nant transfor
mation using histocytological findings; the diagno sis is often made based on the clinical progression of the disease instead.
Their rapid progression, tumor formation and metastasis in the present patient suggested malignant transfor mation.
This is important considering the frequently fatal course of symptomatic NCM and the limited treatment options available for this disorder. There are no established treatments for symp
tomatic NCM such as radiotherapy and chemotherapy, although surgical resection may be performed to prevent the development of malignant melanoma. In cases of symptomatic NCM with DWC, surgical and medical measures remain palliative since death is often inevitable, especially when malignant CNS involvement is diagnosed. A ventriculoperitoneal shunt is very effective for palliating neurological symptoms secondary to hydrocephalus.
There are some reports of clinical improvement in paraneoplastic neurological syndrome after IVIG therapy17). IVIG has been shown to have a variety of anticancer activity, including interaction with tumor cell proteins, induction of interleukin12 secretion, ex
pression of matrix metalloprotei nase9, and suppression of tumor cell growth. The dose is typically 1 g/kg per cycle, given as a slow infusion, up to maximum of 25 g/day. The study pro
tocol determined that patients would be treated every 3 weeks for up to six cycles or until progressive disease occurred. At the time of each infusion, routine blood counts and serum bioche
mistry would be tested, along with physical examinations. This protocol might be useful when using IVIG earlier in the course of malignant melanoma or as adjunctive therapy in patients without evidence of disease following surgery.
According to the World Health Organization, the incidence of melanoma is increasing more rapidly than that of any other cancer worldwide despite ongoing attempts to prevent it. Recent reports have found that the 5year survival rate of melanoma is improving, which is probably due to early detection and treat
ment of the condition. The prognosis of symptomatic NCM is
extremely poor. Once symptoms develop 82% of NCM patients die within 3 years after a progressive and sometimes rapidly deteriorating course of the disease18,19). Association with DWC worsens this prognosis further. The median survival rate for these patients is 6.5 months after onset of symptom1,20). The acute deterioration and death were consistent with that of previous reports, which noted that most patients die within 4 months after the onset of neurological symptoms.
In conclusion, we present an extremely rare case of lateonset NCM associated with DWC. This condition needs attention, par
ticularly in patients with GCMN or multiple melanocytic nevi. In cases of symptomatic NCM with DWC, surgical and medical measures remain palliative since death frequently occurs in spite of treatment. We suggest that the administration of IVIG in NCM might have a role to play in the treatment of malignant melanoma.
요약
신경피부멜라닌증은 피부와 중추신경계를 침범하는 비가족성 선 천성 증후군으로 선천성 모반이 매우 크거나, 3개 이상 다수이면서 양성 또는 악성의 연수막 내 멜라닌세포 증식을 특징으로 하는 드문 증후군이다. 증상이 있는 신경피부멜라닌증의 10%에서 댄디 워커 증후군이 동반되며, 이 경우 예후는 매우 좋지 않다.
저자들은 발작으로 방문하여 신경피부멜라닌증과 댄디 워커증후 군이 동반된 7세 여아에서 반복적인 IVIG 투여로 일시적으로 신경학 적 증상(의식상태와 반마비)이 호전되는 증례를 경험하였기에 보고 하는 바이다.
References
1) Kadonaga JN, Frieden IJ. Neurocutaneous melanosis: definition and review of the literature. J Am AcadDermatol 1991;24:747-55.
2) Kalaycı M, Cağavi F, Bayar U, Gül Ş, Dursun A, Ermis B, et al. Neu- rocutaneous melanosis associated with Dandy-Walker malfor- mation. ActaNeurochir (Wien) 2006;148:1103-6.
3) Green LJ, Nanda VS, Roth GM, Barr RJ. Neurocutaneous mela- nosis and Dandy‐Walker syndrome in an infant. Int J Dermatol 1997;36:356-9.
4) Arai M, Nosaka K, Kashihara K, Kaizaki Y. Neurocutaneous me- lanosis associated with Dandy-Walker malformation and a men- ingohydroencephalocele: case report. J Neurosurg 2004;100:
501-5.
5) Berker M, Oruckaptan HH, Oge HK, Benli K. Neurocutaneous melanosis associated with Dandy-Walker malformation. Pediatr Neurosurg 2001;33:270-3.
6) Caceres A, Trejos H. Neurocutaneous melanosis with associated
Dandy-Walker complex. Childs Nerv Syst 2006;22:67-72.
7) Kang SG, Yoo DS, Cho KS, Kim DS, Chang ED, Huh PW, et al.
Coexisting intracranial meningeal melanocytoma, dermoid tumor, and Dandy-Walker cyst in a patient with neurocutaneous melanosis: Case report. . J Neurosurg 2006;104:444-7.
8) Marnet D, Vinchon M, Mostofi K, Catteau B, Kerdraon O, Dhel- lemmes P. Neurocutaneous melanosis and the Dandy–Walker complex: an uncommon but not so insignificant associa tion.
Childs Nerv Syst 2009;25:1533-9.
9) McClelland III S, Charnas LR, SantaCruz KS, Garner HP, Lam CH. Progressive brainstem compression in an infant with neuro- cutaneous melanosis and Dandy–Walker complex following ventriculoperitoneal shunt placement for hydrocephalus. J Neurosurg 2007;107:500-3.
10) von Rokitansky K. Ein ausgezeichneter Fall von Pigment-Mal mit. ausgebreiteter Pigmentierung der inneren Hirn-und Rüc- kenmarkshäute. Allg Wien Med. 1861;6:113-6.
11) Fox H, Emery JL, Goodbody RA, Yates PO. Neuro-cutaneous melanosis. Arch Dis Child 1964;39:508-16.
12) Chaloupka J, Wolf R, Varma P. Neurocutaneous melanosis with the Dandy-Walker malformation: a possible rare pathoetiologic association. Neuroradiol 1996;38:486-9.
13) Peters R, Jansen G, Engelbrecht V. Neurocutaneous melanosis with hydrocephalus, intraspinal arachnoid collections and syringomyelia: case report and literature review. Pediatr Radiol
2000;30:284-8.
14) Hayashi M, Maeda M, Maji T, Matsubara T, Tsukahara H, Takeda K. Diffuse leptomeningeal hyperintensity on fluid-attenuated inversion recovery MR images in neurocutaneous melanosis.
AJNR Am J Neuroradiol 2004;25:138-41.
15) Peretti-Viton P, Gorincour G, Feuillet L, Lambot K, Brunel H, Raybaud C, et al. Neurocutaneous melanosis: radiological- pathological correlation. Eur Radiol 2002;12:1349-53.
16) Faillace WJ, Okawara S-H, McDonald JV. Neurocutaneous mela- nosis with extensive intracerebral and spinal cord involvement:
report of two cases. J Neurosurg 1984;61:782-5.
17) Blaes F, Strittmatter M, Merkelbach S, Jost V, Klotz M, Schimrigk K, et al. Intravenous immunoglobulins in the therapy of para- neoplastic neurological disorders. J Neurol 1999;246:299-303.
18) Chu WC, Lee V, Chan YL, Shing MM, Chik KW, Li CK, et al.
Neurocutaneous melanomatosis with a rapidly deteriorating course. AJNR Am J Neuroradiol 2003;24:287-90.
19) Zhang W, Miao J, Li Q, Liu R, Li Z. Neurocutaneous melanosis in an adult patient with diffuse leptomeningeal melanosis and a rapidly deteriorating course: case report and review of the litera- ture. Clin Neurol Neurosurg 2008;110:609-13.
20) Di Rocco F, Sabatino G, Koutzoglou M, Battaglia D, Caldarelli M, Tamburrini G. Neurocutaneous melanosis. Childs Nerv Syst 2004;20:23-8.