458
경동맥 내막 부위 에코 음영 증강의 관상 동맥 범행 병변 내의 죽상 경화 예측 정도
가톨릭대학교 의과대학 순환기내과학교실
최윤석·윤호중·홍은주·최용원·이동현·김지훈·박철수 오용석·정욱성·승기배·김재형·최규보·홍순조
The Prediction of High Echogenicity of Intimal Area in Carotid Artery for the Plaque Burden of Culprit Lesion in Coronary Artery Disease
Yun-Seok Choi, MD, Ho-Joong Youn, MD, Eun-Joo Hong, RN, Yong-Won Choi, MD, Dong-Hyun Lee, MD, Ji-Hoon Kim, MD, Chul-Soo Park, MD,
Yong-Seog Oh, MD, Wook-Sung Chung, MD, Ki-Bae Seung, MD, Jae-Hyung Kim, MD, Kyu-Bo Choi, MD and Soon-Jo Hong, MD
Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
ABSTRACT
Background and Objectives:The intima-media thickness (IMT) of the common carotid artery has been widely used as a good index of atherosclerosis. The aim of this study was to test the correlation between the thickness of the high echogenicity intimal area (HELIT) on carotid ultrasound and the plaque burden of the culprit lesion on coronary intravascular ultrasound (IVUS). Subjects and Methods:In 33 patients (M:F=20:13, mean age 63±8 yrs) that underwent coronary angiogram, the HELIT and IMT from carotid ultrasound were compared with the plaque burden of the culprit vessel on IVUS. The high echogenic layer of the intimal area (HELIA) on carotid ultrasound was defined as a thickened echogenic superficial layer at the far wall of the common carotid artery using 15 MHz linear array transducer. The plaque burden was defined as the maximal percent plaque area of the culprit lesion on IVUS. The HELIT and IMT ration was defined as the percent ratio of HELIT on IMT. Results:The mean HELIT, carotid IMT, ratio of HELIT/IMT and maximal percent plaque area of the culprit lesion were 0.27±
0.03 mm, 0.85±0.22 mm, 0.33±0.07 and 68.43±11%, respectively. The HELIT was closely related to the maximal percent plaque area on IVUS (r=0.34, p<0.05), but not to the other IVUS parameters or risk factors of CAD.
Conclusion:Our data suggest that the high echogenic layer of the intimal area on carotid ultrasound is predictive of the plaque burden in the culprit vessel. (Korean Circulation J 2006;36:458-464)
KEY WORDS:
Carotid artery;Atherosclerosis;Coronary artery disease;Plaque.
서 론
경동맥 초음파는 심혈관계의 동맥 경화성 변화를 조기에 발
견할 수 있는 비 관혈적 검사로 오랫동안 널리 이용되어 왔 으며1-3) 경동맥 초음파상에서 관찰되는 죽상 경화반은 관상 동맥의 심각한 협착을 시사하는 중요한 소견으로 알려져 있 다.4)5) 그러나 보고된 문헌에 따라 차이가 있지만 현재까지 경 동맥 초음파상의 내막-중막 두께(intima-media thickness, 이하 IMT)와 관상 동맥 협착 정도와의 상관 관계는 기대 이 상으로 높지는 않다(r=0.26~0.29).6) 이중에서 가장 중요한 이유는 관상 동맥 내의 죽상 경화반은 혈관의 구조상 내피 세 포, 결체 조직, 평활근 등으로 구성 되어 있는 내막(이하, in- 논문접수일:2006년 1월 31일
수정논문접수일:2006년 4월 19일 심사완료일:2006년 5월 06일
교신저자:윤호중, 150-713 서울 영등포구 여의도동 62 가톨릭대학교 의과대학 순환기내과학교실
전화:(02) 3779-1325·전송:(02) 3779-1374 E-mail:[email protected]
tima)층의 증식에 해당되지만 정상인에서 경동맥 초음파의 IMT중 intima가 차지하는 비율은 30% 정도이며 나머지 약 70%는 중막(이하, media)이 포함된 수치이기 때문에7) 관상 동맥의 협착 정도와 경동맥 IMT와의 상관도가 높지 않을 수
있다.8-10) 그러므로 intima의 두께 만을 측정하고자 하는 시
도가 있어 왔으나11) 정상 intima의 두께가 0.3 mm 이하이며 동맥 경화의 특성상 병변이 불규칙하게 분포되기 때문에 신 뢰성 있는 비 관혈적 측정 방법은 아직 보고된 바가 없다.
혈관 내 초음파(intravascular ultrasound, IVUS)는 내강의 협착 정도만으로 관상 동맥 질환을 평가하는 고식적 관동맥 조영술에 비하여 동맥 경화반을 포함한 혈관벽의 구조를 정 확히 평가할 수 있다는 점에서 유용한 방법으로 알려져 있 으나12) 관혈적인 검사 방법이기 때문에 모든 환자에게 적용 하기는 어렵다. 이에 저자들은 경동맥 초음파에서 IMT의 표 층부에서 관찰되는 에코 음영 증강 층(High echogenic layer of intima area, 이하 HELIA)의 두께(thickness of HELIA, 이하 HELIT)를 고주파 선형 탐촉자로 측정하고 관상 동맥 IVUS와 비교함으로써 그 임상적 의의를 알아보고자 하였다.
대상 및 방법
대 상
2003년 2월부터 본 교실에서 관상동맥 조영술 상 70% 이 상의 협착 병변이 확인된 환자 중 관상동맥 조영술 및 혈관 내 초음파가 시행된 33명(남자:여자, 20:13명, 평균 연령, 63±8세)을 대상으로 하였다. 대상 환자들의 관상 동맥 위험 인자인 당뇨, 고혈압, 고지혈증, 흡연 등의 유무를 확인 하 였다. 당뇨병은 2001년 미국 당뇨병학회 진단 기준에 근거하 여 당뇨병의 전형적인 증상이 있으며 1) 현재 경구 혈당 강하 제나 인슐린 치료를 받고 있는 사람, 2) 평상시 혈당이 200 mg/dL 이상이거나 3) 공복 혈당이 전혈 기준으로 126 mg/
dL 이상이며 식후 2시간 혈당이 200 mg/dL 이상인 경우로 정의 하였고 고혈압은 2003년 제 7 차 국제 협력 모임(JNC
Ⅶ)의 기준에 의거 수축기 기준 140 mmHg 이상 이거나 이 완기 기준 90 mmHg를 초과하거나 현재 항 고혈압제를 복 용하여 치료중인 환자를 기준으로 하였으며 고 콜레스테롤 혈 증은 2001년 국제 콜레스테롤 교육 프로그램(NCEP)의 성인 치료지침 3판(ATP Ⅲ)에 따라 취침 전 8시간 이상 공복 후 총 콜레스테롤 기준 240 mg/dL 이상, 고 중성 지방 혈증은 200 mg/dL 이상으로 정의하여 이에 해당하거나 현재 항 고지혈 증 약물을 투약 중인 환자를 각각 포함하였다.
경동맥 초음파 및 HELIA의 두께 측정
경동맥 초음파는 관상 동맥 조영술을 시행 받은 동일한 환 자들을 대상으로 조영술의 결과를 모르는 상태에서 환자의 우측 경동맥 부위를 15 MHz 고주파 탐촉자를 이용한 초음파 (Hewlett Packard, HP Sonos 5500 system)를 통해 내경 동
맥 0.5~1.0 cm 부위가 포함되도록 관찰하였다. IMT의 측정 은 유양 돌기와 목 빗근의 흉골 부착부 사이를 총 경동맥의 직경이 최대로 관찰되는 단면을 Pignoli 등13)의 방법대로 경 동맥 벽의 intima 경계와 media와 외막 경계가 형성하는 두 개의 고음영선 사이의 거리를 측정하였다. HELIT의 측정은 경동맥 초음파의 원위부 벽의 영상을 inverted image로 처 리하여 경동맥의 내강과 접한 IMT 표층부의 HELIT중 최대 부위를 5회 측정하여 평균하였다. 또 HELIT와 IMT의 비를 구하였다(Fig. 1). 대상 환자에서 무작위로 추출한 8명에 대 해 검사자간 및 검사자 내 오차를 측정하였다. 측정은 우측 총 경동맥 분지 부위에서 시행하였으며 검사자간 오차는 두 명의 서로 다른 숙련된 경동맥 초음파 검사자에 의해 처음 검 사 후 2일 이내에 시행되었고 검사자 내 오차는 같은 검사자 에 의해 처음 시행 후 3일 이내에 이루어졌다. 결과는 Bland 와 Altman에 의한 coefficient variation 방법으로 나타내 었다.14)
관상동맥 조영술 및 혈관 내 초음파
관상동맥 조영술은 우측 대퇴 동맥을 통해 Judkins씨 방 법으로 시행하였다. 환자의 증상과 연관된 범행 병변은 심전 도 및 경흉부 심초음파, 심근 핵의학 영상, 운동 부하 검사 등을 통해 확인한 후 병변 내 혈관의 협착 정도가 가장 심 한 곳을 범행 병변으로 정하였다. 죽상 경화반의 정도는 조 영술 도중 IVUS catheter(Atlantis, 2.5F, 30 MHz, Boston Scientific, Natick, MA, USA)를 이용한 자동 pull back 방 법으로 풍선 확장술 전의 영상을 얻었으며 범행 병변의 혈관 최소 내경, 죽상 경화반의 최대 단면적을 측정하였고 plaque burden은 죽상 경화반의 최대 단면적과 기준 혈관의 외막 탄 력층 내의 단면적과의 비율로 정의하였다(Fig. 1).15) 경동맥 초음파상에서 측정된 HELIT와 IMT는 혈관 내 초음파에서 측정된 죽상 경화반의 정도 및 최대 단면적과 비교하여 각각 그 상관 정도를 평가 하였고 관상 동맥 위험 인자의 유무에 따라 HELIT, IMT, HELIT/IMT ratio의 평균을 비교하였다.
통 계
자료의 분석은 SPSS for windows 11.0(SPSS inc. Chicago, IL, USA)를 이용하였고 모든 수치는 평균 및 표준 편차로 표 시하였으며 평균을 t-test로 비교하여 p 값이 0.05미만일 경 우를 유의 한 것으로 판정하였다. 경동맥 초음파의 지표와 혈 관 내 초음파 지표들과의 상관은 Pearson 상관 계수를 이용 하여 구하였고 p값은 0.05이하를 유의한 것으로 판정하였다.
결 과
임상적 특징
대상군 33명의 평균 나이는 62.2±8.6세이고 관상 동맥 위 험 인자는 고혈압 21명(63.6%), 당뇨병 11명(33.3%), 흡연
12명(36.4%), 고 콜레스테롤 혈증 3명(9.1%), 고 중성지방 혈증 5명(15.2%)이었다. 이 중 고 지혈증 약물을 투약 중인 환자는 고 콜레스테롤 혈증 환자 3명중 1명에서 statin을 복
용하고 있었다. 대상 환자들의 진단은 안정형 협심증 24명 (72.7%), 불안정형 협심증 7명(21.3%), 비 ST 분절 상승 심 근경색 1명(3%), ST 분절 상승 심근 경색 1명(3%)이었으며 범행 혈관은 좌 주간지 4명(12.1%), 좌전하행지가 28명(84.9%), 우측 관상동맥 1명(3%)이었다. 관상 동맥 조영술상 70% 이 상의 협착을 갖는 혈관의 수는 1 vessel 22명(66%), 2 vessel 9명(27%), 3 vessel 2명(6%)이었다(Table 1).
관상 동맥 위험 인자에 따른 경동맥 HELIT, IMT, HELIT/IMT과의 비의 비교(Table 2)
대상 환자들 33명 모두 경동맥 초음파를 통해 HELIT, IMT 및 HELIT/IMT의 비를 측정 할 수 있었다. HELIT에 대한 검사자간 coefficient variation은 19.3%이었으며 검사자 내 의 variation은 16.1%로 나타났다. 또 관상 동맥 위험 별로 분리하여 보면 성별에 따른 남녀 평균 및 고혈압에 따른 HELIT, IMT, HELIT/IMT 비 간에 통계적 유의성은 없었다.
그러나 당뇨병의 유무에 따른 비교를 보면 HELIT 0.26±0.03 mm와 0.26±0.04 mm(p=0.60), IMT 0.98±0.17 mm과 0.76±0.11 mm(p=0.00), HELIT/IMT 비 0.27±0.06과 0.35±0.06(p=0.004)로 당뇨병이 있는 군에서 IMT가 유의 하게 증가 되었고 HELIT/IMT의 비에서는 비 당뇨병 군에서 유의한 증가를 보였다. 고 콜레스테롤 혈증의 유무는 HELIT/
Table 1. Clinical characteristics of the study subjects
Age (years) 62.2±8.6
Gender (male:female) 33 (20:13)
Risk factor
Hypertension 21 (63.6%)
Diabetes 11 (33.3%)
Smoking 12 (36.4%)
Hypercholesterolemia 03 (09.1%) Hypertriglyceridemia 05 (15.2%)
Diagnosis
Stable angina 24 (72.7%)
Unstable angina 07 (21.3%)
Non ST elevation MI 01 (03%)0.
ST elevation MI 01 (03%)0.
Vessel type(culprit vessel)
Lt. main coronary artery 04 (12.1%) Lt. anterior descending artery 28 (84.9%)
Rt. coronary artery 01 (03%)0.
Stenotic vessel number
1VD 22 (66%)0.
2VD 09 (27%)0.
3VD 02 (06%)0.
MI: myocardial infaction, Lt: left, Rt: right, VD: vessel disease
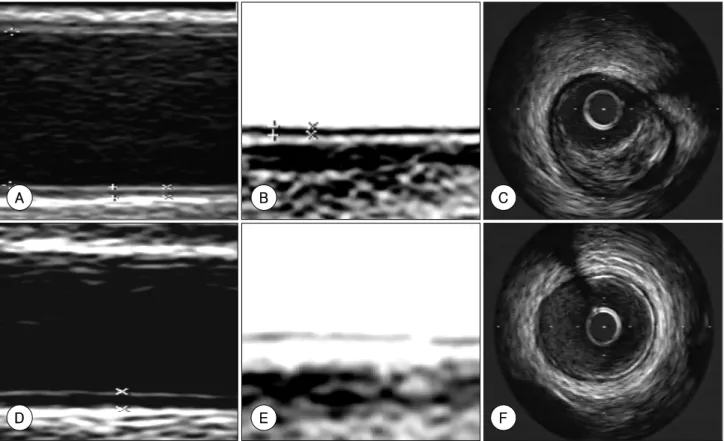
Fig. 1. Upper: example of measuring HELIT and IMT of far wall in common carotid artery using 15 MHz high frequency transducer in three vessel diseased patient. A: high echogenic thickening of intimal area was showed. B: more clearly delineated with inverted zoom image. C: IVUS finding of culprit vessel showed heavy plaque burden in this patient. Lower: example of same measuring in minimal coronary artery diseased patient. D:
minimal thickening of intimal area was showed. E: tiny echogenic layer was barely visible with inverted zoom image. F: and also minimal plaque burden on IVUS. HELIT: thickness of high echogenic layer of thickness, IMT: intima-media thickness, IVUS: intravascular ultrasound.
A B C
D E F
IMT의 비 0.41±0.11과 0.31±0.06(p=0.03)으로 고 콜레스 테롤 혈증의 환자에서 유의한 증가를 보였다. 흡연과 고 중 성지방 혈증 및 병변 혈관의 갯수와는 각각 HELIT, IMT, HELIT/IMT의 비는 통계적 유의성이 없었다(Table 3).
관상 동맥 위험 인자에 따른 IVUS 상의 죽상 경화반과 경동맥 초음파의 비교
IVUS는 대상 환자에서 풍선 확장술 없이 모두 시행할 수 있었다. IVUS를 통한 죽상 경화반의 면적을 비교해 보면 남 녀(p=0.13), 고혈압의 유무(p=0.50), 당뇨병의 유무(p=0.24), 흡연의 유무(p=0.48), 고 콜레스테롤 혈증(p=0.90), 고 중성 지방 혈증(p=0.18)등은 통계적 유의성이 모두 없었다. 그리 고 범행 병변의 plaque burden을 위험 인자와 비교하면 남
녀(p=0.50), 고혈압(p=0.26), 당뇨병(p=0.07), 흡연(p=0.59), 고 콜레스테롤 혈증(p=0.36), 고 중성지방 혈증(p=0.95)로 통계적 유의성은 전부 없었다. 혈청학적 인자 중 당화 색소 는 IMT및 HELIT/IMT의 비와 유의한 상관 관계를 보였고 (r=0.61, r=-0.35) 고밀도 콜레스테롤과 IMT는 음의 상관 관계를 보였다(r=-0.35). 그러나 그 이외 다른 경동맥 초음 파와 혈청학적 인자와는 상관 관계가 없었다(Table 4). IVUS 상의 죽상 경화반의 단면적은 당화 혈색소, 총 콜레스테롤, 총 중성지방, 고밀도 콜레스테롤, proBNP, CRP와 유의한 상 관 관계를 나타내지 않았다(Table 5).
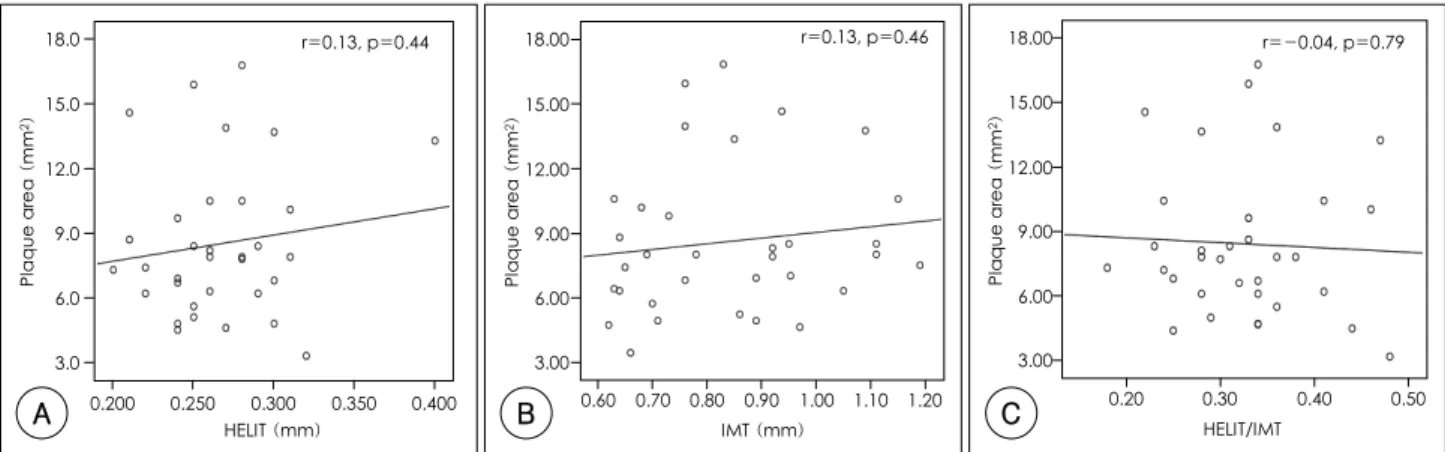
경동맥 초음파와 혈관 내 초음파 상에서 죽상 경화반과의 상관관계 혈관 내 초음파상의 죽상 경화반의 단면적은 HELIT, IMT, HELIT/IMT의 비 들과는 유의한 상관 관계를 보이지 않았고 (Fig. 2), 죽상 경화반의 중등도(plaque burden)와의 비교에
Table 2. Carotid HELIT and IMT and coronary plaque severity according to risk factors
Gender Hypertension Diabetes
Male (n=20) Female (n=13) + (n=21) - (n=12) + (n=11) - (n=22) HELIT (mm) 0.26±0.04 0.26±0.03 0.27±0.03 0.26±0.05 0.26±0.03* 0.26±0.04*
IMT (mm) 0.86±0.18 0.80±0.15 0.86±0.17 0.82±0.16 0.98±0.17* 0.76±0.11*
HELIT/IMT ratio 0.32±0.07 0.32±0.07 0.33±0.07 0.30±0.07 0.27±0.06* 0.35±0.06*
Plaque area (mm2) 9.23±3.74 7.38±2.78 7.60±2.71 10.0±4.18 9.51±3.32* 8.00±3.50*
Plaque burden (%) 70.3±11.2 67.8±10.0 67.8±8.63 72.2±13.4 74.0±7.91* 67.0±11.2*
*: p<0.05. HELIT: thickness of high echogenicity of intimal area, IMT: intima-media thickness, CSA: cross sectional area. plaque area (mm2)=
vessel CSA-lumen CSA, plaque burden (%)=(plaque area/vessel CSA)×100
Table 3. Carotid HELIT and IMT and coronary plaque severity according to risk factors
Smoking Hypercholesterolemia Hypertriglyceridemia + (n=12) - (n=21) + (n=3) - (n=30) + (n=5) - (n=28) HELIT (mm) 0.26±0.01 0.26±0.04 0.32±0.07* 0.26±0.03* 0.25±0.01 0.26±0.04
IMT (mm) 0.83±0.18 0.83±0.16 0.84±0.13* 0.81±0.17* 0.87±0.18 0.83±0.17
HELIT/IMT ratio 0.32±0.06 0.33±0.08 0.41±0.11* 0.31±0.06* 0.29±0.05 0.33±0.07 Plaque area (mm2) 9.23±3.70 8.24±3.56 8.26±5.00* 8.53±3.40* 6.58±2.33 8.85±3.56 Plaque burden (%) 71.1±11.7 69.0±9.23 63.9±14.7* 69.8±10.3* 69.0±8.28 69.4±11.1
*: p<0.05. HELIT: thickness of high echogenicity of intimal area, IMT: intima-media thickness, CSA: cross sectional area. plaque area (mm2)=
vessel CSA-lumen CSA, plaque burden (%)=(plaque area/vessel CSA)×100 Table 4. Correlation between carotid parameters and coronary plaque on IVUS, serum markers
HELIT IMT HELIT/IMT
R p R p R p
Plaque area (mm2) -0.13* 0.44* -0.13* 0.46* -0.04* 0.79*
Plaque burden (%) -0.34* 0.04* -0.26* 0.13* -0.01* 0.93*
HbA1C -0.16* 0.36* -0.61* 0.00* -0.35* 0.04*
Total cholesterol -0.22* 0.21* -0.06* 0.70* -0.20* 0.25*
Triglyceride -0.00* 0.99* -0.13* 0.45* -0.20* 0.25*
HDL cholesterol -0.06* 0.73* -0.35* 0.04* -0.27* 0.12*
Pro BNP -0.22* 0.29* -0.87* 0.68* -0.22* 0.30*
CRP -0.05* 0.78* -0.04* 0.79* -0.10* 0.58*
*: p<0.05. HELIT: thickness of high echogenicity of intimal area, IMT: intima-media thickness, CSA: cross sectional area, BNP: brain natriuretic peptide, IVUS: intravascular ultrasound, CRP: C-reactive protein. HELIT/IMT: ratio of HELIT/IMT, plaque area (mm2)=
vessel CSA-lumen CSA, plaque burden (%)=(plaque area/vessel CSA)×100
Table 5. Correlation between coronary plaque on IVUS and serum markers
Plaque area (mm2) Plaque burden (%)
R p R p
HbA1C -0.24 0.17 -0.18 0.33
Total cholesterol -0.02 0.90 -0.14 0.43
Triglyceride -0.09 0.58 -0.04 0.78
HDL cholesterol -0.13 0.49 -0.16 0.37
Pro BNP -0.15 0.47 -0.11 0.58
CRP -0.04 0.83 -0.24 0.19
HELIT: thickness of high echogenicity of intimal area, IMT: intima- media thickness, CSA: cross sectional area, BNP: brain natriuretic peptide, IVUS: intravascular ultrasound, CRP: C-reactive protein.
plaque area (mm2)=vessel CSA-lumen CSA, plaque burden (%)=
(plaque area/vessel CSA)×100
서 HELIT는 유의한 양의 상관 관계를 보였다(r=0.34, p=
0.04)(Fig. 3). 그러나 IMT나(r=0.26, p=0.13). HELIT/IMT 과의 비(r=-0.01, p=0.93)는 IVUS에서의 plaque burden와 상관 관계를 보이지 않았다.
고 찰
많은 연구에서 동맥 경화증의 조기 발견에 대한 경동맥 초 음파의 유용성을 보고 한 바 있으나16-18) 아직까지 관상 동맥 질환의 협착의 정도와 경동맥 초음파의 IMT와는 그 관련성 이 높지 않다고 알려져 왔다.6)19) 김 등20)의 연구에 의하면 경 동맥 초음파의 IMT와 관상 동맥 조영술 상의 협착을 비교 한 연구에서 modified Gensini score와 최대 경동맥 IMT 사 이의 상관 정도는 0.29 정도였다(p<0.001). 이는 IMT와 70%
이상의 협착을 갖는 관상 동맥의 수를 비교한 Adams 등6)의 연구나(r=0.26) 본 연구에서의 IMT와 Plaque burden의 상 관 정도(r=0.26)와 유사 하였다. 관상 동맥의 죽상 경화성 변 화 정도를 IVUS로 평가 하는 연구21)에 이어 Ogata 등22) IVUS 를 통한 좌 주간지 혈관 내의 죽상 경화반의 정도를 경동맥 초음파와 비교하여 초기 관상 동맥의 죽상 경화를 비 침습적
방법으로 평가 하고자 하였다. 이들은 경동맥의 최대 IMT와 plaque number가 각각 좌 주간지 관상 동맥의 평균 plaque burden(r=0.39, r=0.32) 및 최대 plaque burden(r=0.41, r=
0.51)과 관련있다고 하여 관상 동맥 IVUS에서의 plaque bur- den이 경동맥 초음파의 IMT과 관련이 있음을 보고 하였다.23) 또 한편, Semba 등7)은 intima의 죽상 경화 변화가 media의 섬유화뿐 아니라 내측 탄력층의 중복, 분열 등에 영향을 받아 media과 intima은 서로 다른 양상으로 증가한다고 보고하여 intima과 media의 두께를 분리하여 측정하고자 하는 노력이 있어왔다. 본 연구에서는 이러한 시도들을 바탕으로 IVUS를 통한 죽상 경화반의 정량적인 측정과 경동맥 초음파상의 HE- LIT의 의미를 비교해 보고자 하였다. 결과에서 HELIT가 고 혈압이나 연령, 당뇨병 등과 큰 연관성이 없었으나 IMT가 당 뇨병에서 유의한 증가를 보였다는 사실은 당뇨병에서 나타나 는 경동맥 IMT는 Semba 등7)의 연구에서와 같이 media 층 의 비후와 관련이 있다는 연구와 일치하는 소견이라 할 수 있다. 또 본 연구를 통하여 얻을 수 있었던 중요한 결과는 HELIT는 관상동맥 내의 죽상 경화반의 단순한 단면적 보다 는 기준 혈관의 외막 탄력층의 넓이에서 죽상 경화반의 면적 이 차지하는 비율로 나타내는 plaque burden과 통계적으로
Fig. 2. A: correlation between carotid HELIT and plaque area on culprit vessel. B: correlation between carotid IMT and plaque area on culprit vessel. C: correlation between carotid HELIT/IMT ratio and plaque area on culprit vessel. HELIT: thickness of high echogenic layer of intima, IMT: intima-media thickness.
0.200 18.0
15.0
12.0
09.0 06.0
03.0
0.250 0.300 0.350 0.400 r=0.13, p=0.44
HELIT (mm) Plaque area (mm2)
A
r=0.13, p=0.46
IMT (mm) Plaque area (mm2)
18.00
15.00
12.00
09.00 06.00
03.00
0.60 0.70 0.80 0.90 1.00 1.10 1.20
B
r=-0.04, p=0.79
HELIT/IMT Plaque area (mm2)
18.00
15.00
12.00
09.00 06.00
03.00
0.20 0.30 0.40 0.50
C
Fig. 3. A: correlation between carotid HELIT and plaque burden on culprit vessel. B: correlation between carotid IMT and plaque burden on culprit vessel. C: correlation between carotid HELIT/IMT ratio and plaque burden on culprit vessel. HELIT: thickness of high echogenic layer of intima, IMT: intima-media thickness.
r=0.34, p=0.04 90.00
80.00
70.00
60.00
50.00
40.00
0.200 0.250 0.300 0.350 0.400 HELIT (mm)
Plaque burden (%)
A
r=0.26, p=0.13
0.60
IMT (mm)
0.70 0.80 0.90 1.00 1.10 1.20 90.00
80.00
70.00
60.00
50.00
40.00
Plaque burden (%)
B
r=-0.01, p=0.93
Plaque burden (%)
90.00
80.00
70.00
60.00
50.00
40.00 0.20
HELIT/IMT
0.30 0.40 0.50
C
유의하다는 점에서 HELIT는 단순한 죽상 경화의 두께 보다 는 죽상 경화와 이로 인한 혈관 재형성과 관련이 있을 수 있 다는 것이다.24) 현 등25)은 새로운 컴퓨터 기반의 프로그램을 이용하여 intima 부위를 분리하여 측정하였는데 대상 환자의 40%정도에서 가능함을 보고하여 아직까지 intima 측정의 기 술적 어려움을 나타내었다. 이 연구에서는 평균 intima의 두 께가 0.34±0.03 mm로 IMT의 41%에 해당 한다고 하여 본 연구의 HELIT의 평균 0.27±0.03 mm과 HELIT/IMT의 비 (0.33) 보다 다소 높았으며 IMT는 intima의 두께, media의 두께, intima/IMT 비, media/IMT 비와 각각 상관 관계가 있다고 하였다. 본 연구에서는 15 MHz 고주파 탐촉자와 in- verted image를 이용하여 전체 대상 환자들에서 HELIT를 측정 할 수 있었다. 연구에서의 제한점으로는 대상군이 모두 관상 동맥의 심한 협착 소견을 보이는 환자였기 때문에 정 상인에서의 HELIT를 IVUS와 비교 할 수는 없었다. 또 여러 혈관에 질환이 있다 하여도 상대적 중요성을 고려한 시술자 의 주관적 판단으로 IVUS가 좌전 하행지나 근위부 병변에 서 주로 시행되어 대상 혈관이 좌전 하행지에 편중되게 되 었다. 비교 집단 간의 복용 약제에 대한 분석을 시행하지 못 하여 약제에 의한 영향을 완전 배제하지 못한 것도 제한점 이라 할 수 있으며 HELIT 측정의 오차를 개선시킬 수 있는 다양한 방법이 검증 되어야 할 것으로 보인다. 본 연구는 진 행된 관상동맥 협착 병변을 갖는 환자의 경동맥 초음파에서 관찰되는 HELIT와 IVUS를 비교한 첫 번째 보고로서 상기 한 제한점 들에 대한 추가적인 연구가 향후 꼭 필요하다. 결 론적으로 경동맥 초음파상의 intima 부위에서 관찰되는 에 코 음영 증강은 관상 동맥 협착 병변 내의 죽상 경화반의 중 등도를 비 관혈적으로 예측 할 수 있는 중요한 자료가 될 수 있을 것으로 사료된다.
요 약
배경 및 목적:
경동맥 초음파에서 관찰되는 intima 부위의 에코 음영 증 강 층(high echogenic layer of intimal area, 이하 HELIA) 의 두께(thickness of high echogenic layer of intimal area, 이하 HELIT)를 측정하여 혈관 내 초음파(intravascular ultra- sound, 이하 IVUS)를 통한 죽상 경화의 정도와 비교하여 그 임상적 의미를 알아보고자 하였다.
방 법:
관상동맥 조영술에서 70% 이상의 협착을 보이는 33명(평 균 나이 63±8세, 남성 20명, 여성 13명)을 대상으로 IVUS 와 15 MHz 고주파 탐촉자를 이용한 경동맥 초음파를 실시 하여 HELIT와 plaque burden을 비교 분석하였다.
결 과:
전체 대상 33명에서 모두에서 HELIT를 측정할 수 있었다.
HELIT, IMT의 평균 두께는 각각 0.27±0.03 mm, 0.85±
0.22 mm이었고 HELIT/IMT의 비는 0.33±0.07이며 HELIT 는 남녀, 고혈압, 당뇨병, 흡연, 고 콜레스테롤 혈증, 고 중성 지방 혈증과는 통계적 연관성이 없었다. 그러나 HELIT는 IVUS상의 plaque burden과 통계적 연관성을 보였다(r=0.34, p<0.05).
결 론:
경동맥 초음파에서 관찰되는 에코 음영 증강 층은 관상동 맥 죽상 경화반의 중등도와 관련이 있다.
중심 단어:경동맥;죽상 경화;관상 동맥;Plaque.
REFERENCES
1) Ferrieres J, Elias A, Ruidavets JB, et al. Carotid intima-media thickness and coronary heart disease risk factors in a low risk population. J Hypertens 1999;17:743-8.
2) Wofford JL, Kahl FR, Howard GR, et al. Relation of extent of extracranial carotid artery atherosclerosis as measured by B-mode ultrasound to the extent of coronary atherosclerosis. Arterioscler Thromb 1991;11:1786-94.
3) Grobbee DE, Bots ML. Carotid artery intima-media thickness as an indicator of generalized atherosclerosis. J Intern Med 1994;
236:567-73.
4) Holme I, Enger SC, Elgeland A, et al. Risk factors and raised atherosclerotic lesions in coronary and cerebral arteries. Arte- riosclerosis 1981;1:250-6.
5) Sternby NH. Atherosclerosis in a defined population: an autopsy survey in Malmo, Sweden. Acta Pathol Microbiol Scand 1968;
(Suppl 194):5.
6) Adams MR, Nakagomi A, Keech A, et al. Carotid intima-media thickness is only weakly correlated with the extent and severity of coronary artery disease. Circulation 1995;92:2127-34.
7) Semba I, Funakoshi K, Kitano M. Histomorphometric analysis of age changes in the human inferior alveolar artery. Arch Oral Biol 2001;46:13-21.
8) Schachter M. The pathogenesis of atherosclerosis. Int J Cardiol 1997;62(Suppl):S3-7.
9) Libby P. Vascular biology of atherosclerosis: overview and state of the art. Am J Cardiol 2003;91(Suppl):3A-6A.
10) Salonen JT, Salonen R. Ultrasound B-mode imaging in observa- tion studies of atherosclerosis progression. Circulation 1993;87 (Suppl):1156-65.
11) Kume T, Akasaka T, Kawamoto T, et al. Assessment of coronary intima-media thickness by optical coherence tomography: com- parison with intravascular ultrasound. Circ J 2005;69:903-7.
12) Ge J, Liu F, George G, Haude M, Baumgart D, Erbel R. Angiog- raphically “silent” plaque in the left main coronary artery detec- ted by intravascular ultrasound. Coron Artery Dis 1995;6:805-10.
13) Pignoli P, Tremoli E, Poli A, Oreste P, Paoletti R. Intimal plus medial thickness of the arterial wall: a direct measurement with ultrasound imaging. Circulation 1986;74:1399-406.
14) Bland JM, Altman DG. Statistical methods for assessing agree- ment between two methods of clinical measurement. Lancet 1986;
1:307-10.
15) Mintz GS, Nissen SE, Anderson WD, et al. American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultra- sound Studies (IVUS). J Am Coll Cardiol 2001;37:1478-92.
16) O’Leary DH, Polak JF, Kronmal RA, et al. Distribution and cor- relates of sonographically detected carotid artery disease in the cardiovascular health study. Stroke 1992;23:1752-60.
17) Burke GL, Evans GW, Riley WA, et al. Arterial wall thickness is associated with prevalent cardiovascular disease in middle-aged adults. Stroke 1995;26:386-91.
18) Allan PL, Mowbray PI, Lee AJ, Forwkes FG. Relationship bet- ween carotid intima-media thickness and symptomatic and asymp- tomatic peripheral arterial disease. Stroke 1997;28:348-53.
19) Minamikawa J, Yamauchi M, Tanaka S, Koshiyama H. Carotid arterial intima-media thickening and plaque formation in NIDDM.
Diabetess Care 1998;21:323-4.
20) Kim JH, Youn HJ, Hong EJ, et al. Clinical significance of B-mode ultrasound of common carotid artery for prediction of severity of coronary artery disease: important parameters on hand measu- rement. Korean Circ J 2005;35:467-73.
21) Hagenaars T, Gussenhoven EJ, Poldermans D, van Urk H, van der Lugt A. Rationale and design for the SARIS trial: effect of statin on atherosclerosis and vascular remodeling assessed with intra-
vascular sonography: effect of statin on atherosclerosis and vas- cular remodeling assessed with intravascular sonography. Car- diovasc Drugs Ther 2001;15:339-43.
22) Ogata T, Yasaka M, Yamagishi M, et al. Atherosclerosis found on carotid ultrasonography is associated with atherosclerosis on coronary intravascular ultrasonography. J Ultrasound Med 2005;
24:469-74.
23) Hyun DW, Kim KS, Hur SH. Correlation between the carotid intima-media thickness and the plaque burden of the left main coronary artery using ultrason ography. Korean Circ J 2005;35:
795-800.
24) Hennerici M, Baezner H, Daffershofer H. Ultrasound and arterial wall disease. Cerebrovasc Dis 2004;17(Suppl 1):19-33.
25) Hyun DW, Bae JH, Kim KY, Hwang IK, Kim WS. Measurement of the carotid intima, media and intima-media thickness with ultrasound and new software. Korean Circ J 2005;35:625-32.