Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University, Korea
Abstract
Purpose: The purpose of this study was to compare the stability of GSII implants used to treat complete edentulous patients. A multicenter prospective evaluation was carried out.
Materials and Methods: From January 2007 to December 2008, the study was conducted on 34 completely edentulous patients - maxillary, mandibular, or both - who received Osstem® GSII implants at dental hospitals and clinics nationwide (Chosun University Dental Hospital, Bundang Seoul University Hospital, Apsun Dental Hospital, FM Dental Hospital, Chonnam National University, and Jeju Yena dental clinics). Before and after Osstem® GSII placement, various data were collected and recorded by referring to medical records, radiographs, and clinical tests.
Results: In total, 150 implants were analyzed. The mean follow-up observation period after the implant functioning of the final prosthesis was 8.3 months. In our study, more cases were restored with fixed dentures than with overdentures. Cases restored with overdentures showed a 100% survival rate, and cases restored with fixative dentures showed a 99% survival rate. The GSII implants showed good first and second stability (after the second surgery). At the final follow-up, the survival rate of implants was 98.7%. Four implants showed excessive resorption of the alveolar bone of more than 1.5 mm within one year after implant functioning, and when they were included in the failure group, the survival rate was 97.2%. At the final follow-up observation, no cases exhibited failure of the denture.
Conclusion: Based on the above study, the Osstem® GSII implant system showed good outcomes in short-term follow- ups, and it was confirmed that this system could be usefully applied in edentulous patients during implant restoration.
Key Words: dental implant, survival rate (Implantology 2011; 15(2):142~152)
Introduction
As the human life span increases, so does the size of the elderly population worldwide;
consequently, in the field of dentistry, demand for prosthetic restoration in partially or completely edentulous elderly people is on the rise.
The use of dental implants has increased dramatically, and in partially or completely edentulous patients, the use of dental implant plays an important role to restore lost masticatory function. In patients satisfied only with traditional dentures, implant treatment has been reported to bring about substantial positive effects on their quality of life. Additionally, even in patients with no direct experience to dentures, because of negative prejudice against dentures or indirect experience, the number of patients desiring implant treatment is increasing.
Regarding early implants used successfully in clinics, the goal was to improve the low quality of the edentulous mandible, which had undergone severe resorption, in both mandibles. For example, Branemark implants were placed and fixed resin dentures were reinforced with metals. When such restoration of the mandibular eden- tulous jaw showed good results, the indications for implants were expanded to the maxillary edentulous jaw1.
With the generalization of implants in the edentulous area, numerous implants were developed and used, and based on various studies, further technical develop- ment was achieved. Implants have now been used in clinics for several years. Recently, implants have been
commercialized by various manufacturers in Korea, and in combination with improvements in surgery, retrospective and prospective studies have demon- strated the stability and success rates of these implants.
Osstem® implants were commercialized about 10 years ago. They have been used in clinics and good results have been obtained. The GSII implant (Osstem, Seoul, Korea) used in this study was developed in early 2000. Since that time, although single-center retro- spective studies have been reported, multicenter pro- spective clinical studies are required to assess its effectiveness.
Thus, from 2007, evaluation categories for a pro- spective study were determined, and we asked several centers to record their experience with the implants and to provide scores for the evaluation categories during implant placement.
The purpose of this prospective multicenter study was to evaluate the prognosis of the implants in com- pletely edentulous patients treated using GSII implants.
Materials and Methods
1. Implant
The implants used in this study were GSII (Osstem, Seoul, Korea). GSII implants are submerged type implants have connection of internal hex. These have dual thread of micro and macro thread to minimize bone resorption and surface are treated by RBM.
I
II
2. Subject and methods
From January 2007 to December 2008, among patients who visited dental hospitals and clinics in Korea (Chosun University Dental Hospital, Bundang Seoul National University Hospital, Apsun Dental Hospital, FM Dental Hospital, Chonnam University Dental Hospital, and Jeju Yena Dental Clinic), the study was conducted on 34 patients with completely edentulous maxilla or completely edentulous mandibles who received Osstem® GSII implants. At each institu- tion, after explanation and obtaining informed con- sent, Osstem® GSII placement was performed, and prior to and after implant placement, the predeter- mined evaluation categories were assessed based on medical records, radiographs, and clinical examina- tions. One hundred and fifty implants in total were placed in the subjects. The average follow-up period after placement of the final prosthesis was 8.3 months.
To analyze the clinical success rate, the following factors were examined:
1. Distribution of gender and age
2. The presence or absence of systemic diseases and smoking status
3. Distribution of the edentulous jaw, according to location
4. Distribution of the diameter and width of the implants
5. Distribution of the area of implant placement 6. The number of implants according to the type of the prosthesis
7. The interval between the first and second surgery according to implant placement surgery
8. Evaluation of the residual alveolar crest in the
placement area
Using pre and postsurgical panoramic radiographs and clinical findings during surgery, this was deter- mined according to the Lekholm & Zarb classification method1.
9. Classification of surgical methods used in implant placement
10. Assessment of initial and subsequent stability The stability was measured using either a Periotest® (Siemens AG, Benssheim, Germany) or Osstell® Mentor (Integration Diagnostics AB, Goteborg, Sweden) at implant placement and second surgery. In most insti- tutions, it was measured using one of the two devices.
Patients for whom it was not measured were excluded from the analysis.
11. The resorption rate of marginal bone
At 6 and 12 months after functioning of the prosthe- sis and at the final follow-up observation, radiographs of the implant apex were taken, and the marginal bone resorption rate was measured by comparison with the radiograph of the implant apex taken after surgery.
The value of marginal bone loss was obtained by stan- dard apical X-ray using XCP to minimize error. The measurement method was as follows. The magnifica- tion was calculated based on the length of the placed implant, and subsequently, the average value of the bone resorption rate of the proximal and distal side of implants was obtained.
12. A summary of cases with failed implants 13. Survival rate2
A surviving implant was defined as an implant in place at the time of assessment.
Results
1. The distribution of gender and age (Table 1)
The average age of the patients was 59 years and the 34 patients consisted of 17 males and 17 females. Two patients were in their 30 s, five in their 40 s, eight in their 50 s, 11 in their 60 s, seven in their 70 s, and one patient was over 80.
2. The presence or absence of systemic disease and smoking status (Table 2)
Systemic diseases and smoking status were deter- mined by interviewing patients. The patients have
overlapped systemic diseases were excluded in this study. Of the 34 patients, 17 had systemic diseases, including nine with cardiovascular disease and four with diabetes. Four patients presently smoked or had a history of smoking.
3. Distribution of edentulous areas (Table 3)
The maxilla was completely edentulous in 16 patients, the mandible was completely edentulous in
Table 1. Distribution by age and gender (unit: no. of patients)
30~39 40~49 50~59 60~69 70~79 80~89 Men
Women Total
2 0 2 (6%)
4 1 5 (15%)
5 3 8 (23%)
4 7 11 (32%)
2 5 7 (21%)
0 1 1 (3%)
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
Table 2. General conditions and smoking habits
Type No. of patients
Diabetes mellitus Cardiovascular disease Smoking habit
4 (11.7%) 9 (26.4%)
14 (41.1%)
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
Table 3. Type of final restoration
Edentulous site No. of patients Maxilla only
Mandible only Maxilla+Mandible
14 (41.4%) 16 (47.0%) 4 (11.7%)
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
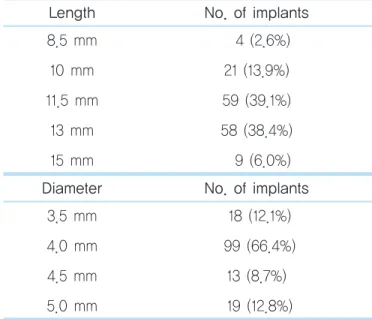
Table 4. Distribution according to length and diameter (unit: no. of implants)
Length No. of implants
8.5 mm 10 mm 11.5 mm
13 mm 15 mm
4 (2.6%) 21 (13.9%) 59 (39.1%) 58 (38.4%) 9 (6.0%)
Diameter No. of implants
3.5 mm 4.0 mm 4.5 mm 5.0 mm
18 (12.1%) 99 (66.4%)
13 (8.7%) 19 (12.8%)
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
III
14, and four patients had a bimaxillary completely edentulous jaw.
4. Distribution of the diameter and length of implants (Table 4)
The length of the placed implants was 11.5 mm in 59 implants, 13 mm in 58, 10 mm in 21, 15 mm in nine, and 8.5 mm in four implants. The diameter was 4.0 mm in 99 implants, 5.0 mm in 19, 3.5 mm in 18, and 4.5 mm in 13 implants.
5. Distribution according to the site of implant placement (Table 5)
Of the 150 implants, 92 were in the maxilla and 58 were in the mandible. In the maxilla, 38 were in the anterior tooth area, 29 were in the premolar area, and 25 were in the molar area. In the mandible, 30 were in the anterior tooth area, 12 were in the premolar area,
and 16 were in the molar area.
6. Number of implants according to the type of upper prosthesis (Table 6)
The number of jaws restored by overdenture pros- thesis was 25, and 13 jaws were restored with a fixed prosthesis. Sixty-four implants were used in connec- tion with the overdenture restorations and 86 were used in connection with fixed prostheses. In overden- ture cases, 2.2 implants on average were used per res- toration, and 6.9 implants on average were used in fixed prosthesis cases.
Table 5. Distribution of implants by site Anterior
tooth Premolars Molars Total Maxilla
Mandible
38 (25.3%) 30 (20.0%)
29 (19.3%) 12 (8.0%)
25 (16.7%) 16 (10.7%)
92 (61.3%) 58 (38.7%)
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
Table 6. Type of final restoration Arch No. of
implants
Average no. of implants Overdenture
Fixed prosthesis
25 (66%) 13 (34%)
64 (42.6%) 86 (57.3%)
2.2 6.9
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
Table 7. Mean interval between the first and second surgery (unit: weeks)
Site Mean weeks
Upper anterior tooth Upper premolars Upper molars Lower anterior tooth Lower premolars Lower molars
16.9 16.6 16.4 10.9 8.7 12.7
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
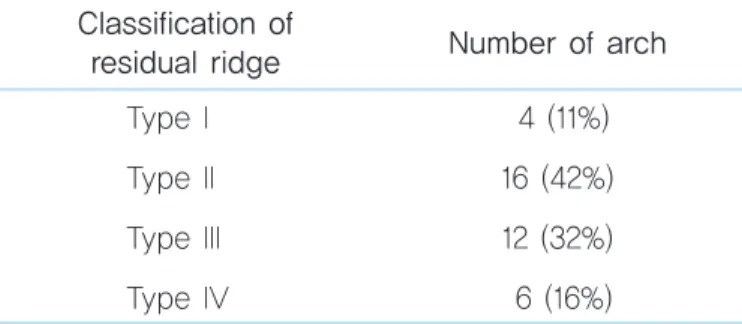
Table 8. Classification of the residual ridge Classification of
residual ridge Number of arch Type I
Type II Type III Type IV
4 (11%) 16 (42%) 12 (32%) 6 (16%)
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
7. Interval between the first and second surgery according to the method of implant placement (Table 7)
The average intervals from the first to the second surgery in the maxillary anterior tooth area, premolar area, and molar area were 16.9, 16.6, and 16.4 weeks, respectively. For the mandibular molar area, the man- dibular premolar area, and the mandibular anterior tooth area, the average intervals were 12.7, 8.7, and 10.9 weeks, respectively.
8. Evaluation of residual alveolar bone in the placement area (Table 8)
In evaluating alveolar bone in the implant placement site, type I was observed in four jaws (11%), type II in 16 jaws (42%), type III in 12 jaws (32%), and type IV in 6 jaws (16%).
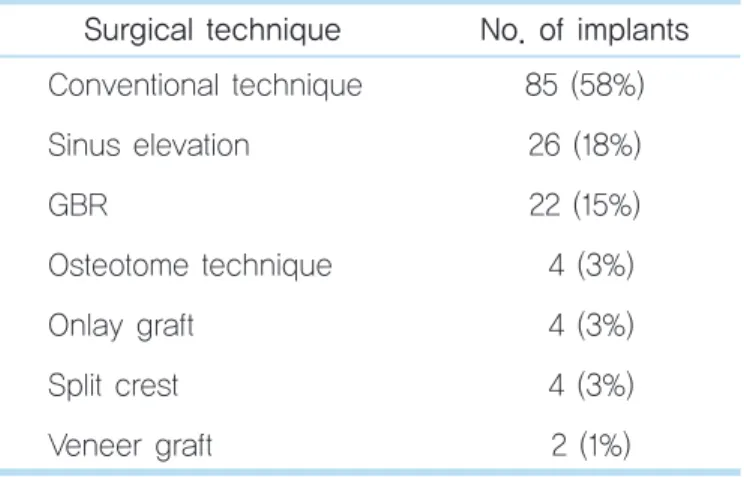
9. Surgical procedures used in implant placement (Table 9)
The previously described general surgical procedure was used in 58% of cases, maxillary sinus elevation in 18%, and guided bone regeneration (GBR) in 15%.
Additionally, an osteotome technique (3%), onlay graft (3%), split crest (3%), and veneer graft (1%) surgeries were applied.
10. Measurement of initial and subsequent stability (Table 10)
Of the implants, 87 were assessed using the Periotest® device; the stability measured immediately after surgery was on average −0.8. The average value Table 9. Surgical technique for implantation (unit:
no. of implants)
Surgical technique No. of implants Conventional technique
Sinus elevation GBR
Osteotome technique Onlay graft
Split crest Veneer graft
85 (58%) 26 (18%) 22 (15%) 4 (3%) 4 (3%) 4 (3%) 2 (1%) GBR, guided bone regeneration.
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
Table 10. Primary and subsequent stability
Stability Periotest® Osstell mentor Primary stability
Secondary stability
(after secondary surgery)
-0.8 -3.6
60.4 72.3
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
Table 11. Distribution of implants by bone re sorption (unit: no. of implants)
Amount of
bone resorption (mm) No. of implants None
0~0.4 0.5~0.9 1.0~1.4 1.5~1.9
≥2.0
136 5 4 1 2 0
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
measured after the second surgery was −3.6.
In 61 implants, stability was measured using the Osstell® mentor; the average stability was 60.4 ISQ immediately after surgery, 72.3 ISQ after the second surgery.
11. Resorption rate of marginal bone (Table 11)
The resorption rate was measured using the root apex radiographs taken immediately after implant placement and at the last follow-up. Among the 150 implants, the resorption rate could be measured in 148 implants. For the measurement method, the magnifi- cation was calculated based on the length of the placed implant, and subsequently, the average values of the bone resorption rate on the proximal and distal sides were obtained. One hundred and thirty-six cases were without bone loss. Bone loss was less than 0.5 mm in five implants, between 0.5 and 1.0 mm in four implants, between 1.0 and 1.5 mm in one implant, and between 1.5 and 2.0 mm in two implants. Bone loss of more than 2 mm did not occur.
12. Summary of cases with failed implants (Table 12)
Implant failure was observed in two patients. In a 68-year-old female patient, an implant 10 mm in
length and 4 mm in diameter was placed in the right maxillary first molar area in association with a maxil- lary sinus elevation procedure, and failure of the implant occurred due to failure of the initial fixation.
Additionally, in a 51-year-old male patient, an implant 8.5 mm in length and 4 mm in diameter was placed in the right mandibular first molar area, together with GBR. Failure of the implant was believed to have been caused by an infection in the vicinity of implant.
13. Success and survival rates (Table 13)
In the 150 implants placed, failure of osseointegra- tion was seen in two implants (1.3%). Thus, the total survival rate was 98.7%. Four implants developed more than 1.5 mm bone loss; the success rate after 1 year Table 12. Summary of failed cases
Case Age Sex Area Length Diameter Prothesis Causes
1 2
68 51
F M
#16
#46
10 mm 8.5 mm
4 mm 4 mm
- Fixed prothesis
Poor primary stability Infection
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
Table 13. Survival, success, and failure rates
Type Rate
Osseointegration failure Total survival rate
Success rate : < 1.5 mm bone loss after a year
Survival of prosthodontics
2 (1.3%) 148 (98.7%) 146 (97.2%)
38 (100%)
Jong-Won Jung et al. : A Prospective Multicenter Study on the Clinical Success Rate of the Osstem® Implant (New GSII RBM) in Edentulous Patients. Implantology 2011
was 97.2%, and the prosthesis survival rate was 100%.
Discussion
In completely edentulous patients, resorption of the residual alveolar crest, indentation of the support of the orofacial area, and deterioration of oral function, in addition to various psychological and social prob- lems, result due to the tooth loss. During the first year after the loss of teeth, the height of the residual alve- olar crest decreases by about 2~3 mm in the maxilla and about 4~5 mm in the mandible3. Later, as the bone remodeling process progresses, the mandible and the maxilla slowly undergo resorption. In total denture patients, the annual resorption of the alveolar crest has been reported to be about 0.2 mm in the mandible and about 0.07 mm in the maxilla, although individual variations occur.
The prognosis of total denture treatment depends on the knowledge and skill level of the surgeon and fac- tors associated with the patient. In patients with no experience of total denture wearing, even if the objec- tive completion level is high, predicting the prognosis is difficult because of factors associated with the patient. Although esthetics can be recovered suffi- ciently by total dentures, and function can be recov- ered to a certain degree, the stability and maintenance are nevertheless poor in patients with a retracted alveolar crest, and particularly in the edentulous man- dible, obtaining maintenance power is difficult.
Compared to the mandible, the maxilla has wider sup- porting areas, and margin obstruction can be per-
formed readily. Thus, patient satisfaction levels for maxillary total dentures are higher. However, if the mandible is edentulous, stability of a total denture in the maxilla may decrease. Additionally, because of strong pressure from opposing teeth, resorption of the maxillary alveolar crest is accelerated and rapid resorption of the alveolar crest in the frontal maxillary area can occur, leading to protrusion of the teeth in the frontal mandibular area and resorption of the mandibular molar area. Thus, the denture can become unstable, and in unstable dentures, combinations of the problems described above can further develop and become exacerbated.
Recently, in patients with severe defects in the alve- olar crest, implant therapy has been used as a more predictable approach. Sennerby and Roos4 reported that by implant placement, resorption of the residual alveolar crest could be delayed. Awad et al.5 reported that in 65- to 75 year old patients treated by either traditional total dentures or overdentures, the average scores of overall satisfaction, comfort, and stability of the implant were significantly higher for overdentures.
In treatment of the completely edentulous jaw using implants, prosthetic restoration can be classified broadly into complete fixed bridges and overdentures;
the success rates of each have been reported. The suc- cessful restoration of the completely edentulous jaw by a complete fixed bridge has been observed in long- term studies, and the maxilla and the mandible have shown different results regarding the success rate.
Zarb and Schmitt6 reported a success rate of 86.3% for implants during 12~15 years of loading in the maxilla, and over a 4- to 9-year loading period, the mandible
IV
showed a 97% implant success rate and a 100% pros- thesis success rate. In implants used with fixed bridg- es, Adell et al.7 reported an 81% implant success rate and an 89% prosthesis success rate in the maxilla dur- ing a 5~9-year loading period, and a 91% implant success rate and a 100% prosthesis success rate in the mandible. In cases restored with overdentures, Hemmings et al.8 reported that 68 implants were placed in 25 overdentures in the mandible and that the success rate was 92.7%. Wright et al.9 reported that in 98 implants placed in the mandible for overdenture restoration, three implants failed, which gave a 96.9%
success rate. Jemt et al.10 reported that in a 5-year prospective multicenter study, the success rate of implants placed in the mandible for overdentures was 96.4%. In another study, Jemt et al.11 reported an 83%
implant success rate for implants placed in the maxil- lary bone with severe resorption for overdentures.
Palmqvist et al.12 reported that during average an 3-year loading period, maxillary overdentures showed a 92% success rate and implants a 70% success rate. In this study, conducted with GSII implants placed in completely edentulous patients, the survival rate of the entire implants was 98.7%, and the success rate of the prosthesis was 100%. Although the follow-up period in this study was shorter than those mentioned above, good survival and success rates were obtained.
In the Osstem® GSII implant used in this study, the dual-thread design with a combination of a micro- thread and macrothread was selected; it is a sub- merged fixture, with an internal hex connection method. For the surface treatment method, the RBM was applied, and because it has a straight body, the
depth of placement could be readily controlled. It has four blades with cutting edges having excellent self- tapping ability and is available with various diameters and lengths. It was developed to be used readily even in the disadvantageous oral environment.
Recently, several studies on Osstem® GSII implants have been reported. In 2009, Kwon et al.13 reported clinically and radiologically successful results at 6 and 12 months follow-up after GSII placement and pros- thetic restoration in 27 patients. In 2008, Kim et al.14 reported a high success rate with GSII in a short-term retrospective study using GSII, USIII, and SSIII.
In this study, Osstem® GSII implants were placed in both the maxilla and the mandible. The implants were placed more commonly in the maxilla than in the mandible, and compared to the premolars and molars, more implants were placed in the front teeth area.
Implants 11.5 mm and 13 mm in length and 4 mm in diameter were used primarily. The upper prosthesis was restored by fixed bridges, and both initial and subsequent stability were shown to be good.
In one case, the implant was removed in a 68-year- old female patient, and an implant 4 mm in diameter and 10 mm in length was placed in the right maxillary molar area. The cause of the failure was determined to be inadequate initial stability. Another failed case involved a 51-year-old male patient who was a heavy smoker. An implant 4 mm in diameter and 8.5 mm in length was placed in the right mandibular molar area, and the prosthesis was completed with a fixed bridge.
The implant, however, was subsequently removed, and the cause of the failure may have been infection in the vicinity of the implant and the subsequent bone loss
due to the infection.
In this study, a 100% success rate was achieved in cases restored with overdentures, and a 99% success rate in cases restored with fixed bridges. These rates were higher than those previously reported.
This study was a multicenter prospective study con- ducted to address the shortcomings of various short- term retrospective studies previously reported.
However, this study has the limit that the number of subject cases was small and the follow-up period is short. By continuous collaboration between the cen- ters, further research with longer-term observation is required.
Conclusion
In this study, a prospective evaluation was per- formed on 150 implants placed in 34 edentulous patients who visited dental hospitals and clinics in various areas of Korea between January 2007 and December 2008 and who consented to the placement of the Osstem® GSII implant. The following results were obtained.
1. Patients in their 50 s and 60 s were the most common. Most patients had a unilateral completely edentulous jaw.
2. The bone quality in the placement area was type II and III in many cases.
3. Implants were placed in the maxillary and man- dibular anterior tooth area in most cases, and more implants were placed in the maxilla compared to the
mandible.
4. Implants 11.5 mm or 13 mm in length and 4 mm in diameter were used primarily.
5. In this study, more cases were restored with fixed bridges than overdentures. In cases restored by over- dentures, the success rate was 100% and in cases restored with fixed bridges, the success rate was 99%.
6. GSII implants showed excellent initial and subse- quent stability (after the second surgery, 3 months after prosthesis placement).
7. At the time of the last follow-up, the survival rate of implants was 98.7%. Four cases showed excess resorption of the alveolar crest bone within 1 year of functioning; when they were included in the failure category, the success rate was 97.2%. At the time of the last follow-up, no case showed failure of the pros- thesis.
The results indicated that the Osstem® GSII implant system were useful for implant restoration in edentu- lous patients.
References
1. Lekholm U, Zarb GA. Patient selection and preparation. In: Brånemark PI, Zarb GA, Albrektson T, (eds). Tissue-integrated protheses:
osseointegration in clinical dentistry. Chicago: Quintessence; 1985. p.
199-209.
2. Albrektsson T, Zarb G, Worthington P, et al. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986; 1: 11-25.
3. Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: a mixed-longitudinal study covering 25 years. J Prosthet Dent. 1972; 27: 120-132.
V
4. Sennerby L, Roos J. Surgical determinants of clinical success of osseointegrated oral implants: a review of the literature. Int J Prosthodont. 1998; 11: 408-420.
5. Awad MA, Lund JP, Shapiro SH, et al. Oral health status and treatment satisfaction with mandibular implant overdentures and conventional dentures: a randomized clinical trial in a senior population. Int J Prosthodont. 2003; 16: 390-396.
6. Zarb GA, Schmitt A. The edentulous predicament. I: A prospective study of the effectiveness of implant-supported fixed prostheses. J Am Dent Assoc. 1996; 127: 59-65.
7. Adell R, Lekholm U, Rockler B, et al. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981; 10: 387-416.
8. Hemmings KW, Schmitt A, Zarb GA. Complications and maintenance requirements for fixed prostheses and overdentures in the edentulous mandible: a 5-year report. Int J Oral Maxillofac Implants. 1994; 9: 191- 196.
9. Wright PS, Watson RM, Heath MR. The effects of prefabricated bar
design on the success of overdentures stabilized by implants. Int J Oral Maxillofac Implants. 1995 ; 10: 79-87.
10. Jemt T, Chai J, Harnett J, et al. A 5-year prospective multicenter follow- up report on overdentures supported by osseointegrated implants. Int J Oral Maxillofac Implants. 1996; 11: 291-298.
11. Jemt T, Book K, Lindén B, et al. Failures and complications in 92 consecutively inserted overdentures supported by Brånemark implants in severely resorbed edentulous maxillae: a study from prosthetic treatment to first annual check-up. Int J Oral Maxillofac Implants. 1992;
7: 162-167.
12. Palmqvist S, Sondell K, Swartz B. Implant-supported maxillary overdentures: outcome in planned and emergency cases. Int J Oral Maxillofac Implants. 1994; 9: 184-190.
13. Kwon MA, Kim YD, Jeong CM, Lee JY. Clinical and radiographic evaluation of implants with dual-microthread: 1-year study. J Korean Acad Periodontol. 2009; 39: 27-36.
14. Kim YK, Yun PY, Kwon MJ. Short-term retrospective clinical study of Osstem® GS II, US III, SS III implants. Implantology. 2008; 12: 12-22.
Reprint requests : Su-Gwan Kim
Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University, 375, Seosuk-dong, Dong-gu, Gwangju 501-759, Korea
Tel : 82-62-220-3815 Fax : 82-62-228-7316 E-mail : [email protected] Received for publication : Jun. 6, 2011 Accepted for publication : Jun. 21, 2011