Received: April 31, 2016 Accepted: May 26, 2016.
Corresponding author: Youn Seon Choi
Department of Family Medicine, Korea University Guro Hospital, 148 Gurodong-ro, Guro-gu, Seoul 08308, Korea Tel: +82-2-2626-2807, Fax: +82-2-837-3966, E-mail: [email protected]
Co-Corresponding author: Kyung Hee Lee
Department of Hemato-Oncology, Yeungnam University Medical Center, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-623-8001, Fax: +82-53-627-4954, E-mail: [email protected]
*These two authors contributed equally to this work.
We are very grateful to all of the institutions that participated.
This study was partially supported by the Korean Society for Hospice & Palliative Care. The sponsor did not have any role in the design or conduct of the study including the collection, management, analysis, and interpretation of the data, or in the preparation, review, or approval of this article.
Copyright Ⓒ 2016 The Korean Academy of Clinical Geriatrics
This is an open access article distributed under the term s of the Creative Com m ons Attribution Non-Com m ercial License (http://creativecom m ons.org/ licenses/by-nc/4.0) which perm its unrestricted non-com m ercial use, distribution, and reproduction in any m edium , provided the original work is properly cited.
중등도 이상의 암성통증을 호소하는 노인 환자에 대한 고용량의 마약성 진통제의 이용: 전향적 관찰 연구
김정은1, 최윤선1,*, 이경희2,*, 김준석3, 고수진4, 백선경5, 김시영5, 송홍숙6, 임보라미7
1고려대학교 구로병원 가정의학과, 2영남대학교병원 혈액종양내과, 3고려대학교 구로병원 혈액종양내과, 4울산대학교 의과대학
울산대학교병원 혈액종양내과학교실, 5경희대학교 혈액종양내과, 6계명대학교 의과대학 내과학교실, 7고려대학교 의과대학 통
계학교실
Use of High-dose Opioids as a Treatment for Elderly Patients with Moderate to Severe Cancer Pain: A Prospective Observational Study
Jung Eun Kim1, Youn Seon Choi1,*, Kyung Hee Lee2,*, Jun Suk Kim3, Su-Jin Koh4, Sun Kyung Baek5, Si-Young Kim5, Hong Suk Song6, Bo Rami Lim7
1Department of Family Medicine, Korea University Guro Hospital, Seoul, 2Department of Hemato-Oncology, Yeungnam University Medical Center, Daegu, 3Department of Hemato-Oncology, Korea University Guro Hospital, Seoul, 4Department of Hemato-Oncology, Ulsan University Hospital, Ulsan University College of Medicine, Ulsan, 5Department of Hemato-Oncology, Kyunghee University Medical Center, Seoul, 6Department of Internal Medicine, Keimyung University School of Medicine, Daegu, 7Department of Biostatistics, College of Medicine, Korea University, Seoul, Korea
Background: Despite the large number of elderly individuals who are dying of cancer in Korea, the quality of pain manage- ment remains poor. Thus, in this study, the safety and efficacy of using high-dose opioids to treat has been evaluated pain in elderly patients with cancer.
Methods: Data from cancer patients (N=94) aged ≥65 years who were administered high-doses of opioids (≥120 mg/day) were collected at 38 hospitals between February 2009 and March 2010. After 8 weeks, changes in pain severity were examined using a numeric rating scale; in addition, the opioid dosages, quality of life parameters, and opioid-based adverse events were investigated.
Results: Ninety-two patients were prescribed opioids at the beginning of the study and followed for 8 weeks. The mean pain intensity changed from 5.61±1.56 at baseline to 4.02±2.17 (P<0.001) after 8 weeks. The mean opioid dosage, expressed as oral morphine equivalents, changed from 178.86±76.88 at baseline to 288.54±389.09 (P=0.0025) after
8 weeks. The quality of life parameters, including daily activities, ambulation, and sleep, improved significantly after 8 weeks (P<0.001). At baseline, 44 patients (47.8%) complained of adverse effects such as constipation, dizziness, and nausea; the frequency of adverse events did not increase after 8 weeks.
Conclusion: The use of high-dose opioids for treating cancer pain is safe, effective, and tolerable in elderly patients.
Key Words: Cancer pain, Opioids, Efficacy, Safety, Elderly
INTRODUCTION
Incidence rates of cancer in Korea have significantly in- creased over the last decade. Of the individuals with cancer in Korea, ∼70% of them are older than 60 years. Moreover, 25% of elderly individuals are dying of cancer.1,2) Despite the prevalence and consequences of pain among older pa- tients, clinicians remain ineffective at assessing and treating pain.3)
Although the three-level pain/analgesic ladder published by the World Health Organization4) in 1986 states that physicians must attempt to select the analgesic that is best suited to a patient’s problem when treating pain, inappro- priate pain treatments are still being administered, with about 50% of patients receiving inadequate pain relief.5) The obstacles blocking optimal pain management vary, but the primary physician-related factors are as follows: insuffi- cient knowledge of pain management methods, concern about opioid regulations, fear of addiction or side effects, and the concern that opioids hasten death. Despite the obstacles, previous studies generally agree that opioids such as mor- phine, oxycodone, fentanyl, and hydromorphone are widely used to treat moderate to severe cancer pain in elderly patients.6,7)
However, the pharmacological characteristics of each opioid receptor vary between individuals, leading to different, patient-specific levels of opioid efficacy and tolerability.8,9) Additionally, elderly people may be more sensitive to pain;
therefore, the pharmacological effects and reactions in the elderly will be different from those in younger individuals.
Specifically, the manner in which people perceive and re- spond to pain changes as they age, which can cause delays in diagnosis and poor recovery from severe pain. Many eld- erly patients have impaired cognitive functioning, confusion,
memory loss, deteriorated eyesight and hearing, and numer- ous other types of dysfunctions that affect organs including the liver and kidney;10-12) these impairments can lead to compliance problems, difficulties in the accurate assessment or management of pain, and adverse events. Thus, opioids may be over-prescribed or under-prescribed to elderly pa- tients or may interact with the other medicinal drugs that the patient is already taking.
Moreover, the aging process can affect the body’s ca- pacity to metabolize or excrete drugs.6) About 60% of older patients with cancer usually suffer from decreased renal function, with drug clearance rates in the elderly typically being <90 mL/min.13) Furthermore, the decreased liver mass and reduced metabolic capacity of cytochrome P450 in elderly patients means that their metabolic capacity for drugs is reduced by 30∼40%.6) The aging process in the elderly also increases the levels of pro-inflammatory cyto- kines such as interleukin 6, tumor necrosis factor, and C-re- active protein.14) Such increases can then lead to an in- creased incidence of catabolism-related conditions including sarcopenia and hypoproteinemia.10) The above-mentioned is- sues support the development of pain medications with im- proved side-effect profiles for elderly patients.
Recently, several studies reported that opioid usage, even at high doses, does not influence the survival rates among patients with advanced cancer.15,16) Given the lack of clinical studies on the efficacy and tolerability of high-dose opioid treatments as pain management strategies for elderly pa- tients with cancer, we performed a sub-analysis to evaluate the efficacy, tolerability, and quality of life (QoL) of elderly patients who received high-dose opioids, as cancer-pain treatments.
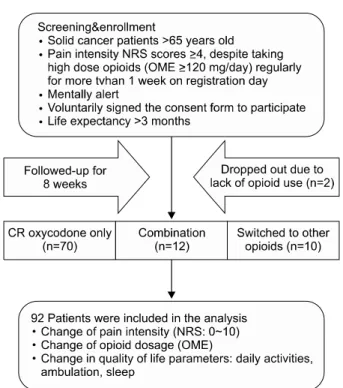
Figure 1. Flowchart for patient recruitment.
MATERIALS AND METHODS
1. Design and subjects
Back et al.17) evaluated the efficacy, tolerability, and QoL of elderly patients who received high-dose opioids, including controlled-release (CR) oxycodone, as cancer-pain treatments by using data from a non-interventional, prospective ob- servational study in cancer patients. This study suggested that over an 8-week period, the use of larger doses of CR oxycodone for cancer pain management is efficient, safe, and tolerable in outpatient clinics. A previous original study en- rolled 486 patients, 318 of whom were followed-up for 8 weeks and 168 of whom dropped out before study com- pletion (8-week follow-up rate: 65.4%).17) The inclusion cri- teria for the present sub-analysis study were as follows: ≥65 years old, diagnosed with a solid tumor including lympho- ma, mentally alert, voluntarily provided informed and sign- ed consent, completed a patient questionnaire, had a limited life expectancy of >3 months, and suffered from moderate or severe cancer pain. Patient eligibility required the pa- tients to have rated their cancer pain above a 4 using a nu- meric rating scale (NRS)18) within 24 h of the registration day, regardless of their use of oral opioids. The patients must also have registered an NRS score of ≥4 even after taking a high opioid dose, expressed as oral morphine equi- valents (OMEs), of ≥120 mg/day19) regularly for >1 week as of the registration day. Patients were excluded if they had the following: hematological malignancies; another in- tervention for pain control such as nerve block, patient- controlled analgesia, or an operation on registration day;
cardiopulmonary diseases or cognitive impairment; or a his- tory of psychological problems. The remaining patients were selected for analysis. The data collected from 94 patients at 38 hospitals (see Appendix 1 for the list of institutions) from February 2009 to March 2010 were analyzed, and the flowchart for patient recruitment is shown in Figure 1.
This study was conducted in accordance with the Decla- ration of Helsinki and was approved by the Local Research Ethics Committees of Korea University Guro Hospital (KUGH08166) and Yeungnam University Medical Center (PCR-09-15).
2. Clinical examinations
Demographic and clinical information was obtained from hospital data repositories, while the patients included in the study provided the following information during their first visit: data on age and sex; cancer-related history including tumor characteristics (primary cancer site and stage); type of treatment received (surgery, chemotherapy, or radiation); the Eastern Cooperative Oncology Group (ECOG) performance status (PS); pain characteristics (pain intensity, type of pain, and source of pain); pattern of prescription drug use during the previous week; and opioid-induced adverse events in- cluding nausea, vomiting, constipation, dizziness, urinary re- tention, respiratory depression, and delusion. All patients were administered a questionnaire to assess their pain in- tensity and QoL including activities, walking, and sleep.
The ECOG PS is an observer-rated scale of a patient’s physical abilities, with scores ranging from 0 (able to per- form all normal activities) to 4 (completely disabled);20) a high score represents interference with QoL. We used part of the Korean version of the EORTC QLQC30 (version 3.0),21) which assesses the QoL experienced by patients dur- ing cancer and its treatment in Korea. The QoL score ranged from 0 to 10, with a high score representing poor
Table 1. Demographic and clinical characteristics of the subjects (N=92)
Characteristics
Mean±SD/N (%) All patients
(N=92)
Men (N=62)
Women (N=30)
Age 70.17±4.39 69.61±4.19 71.33±4.63
Primary cancer
Lung 20 (21.74) 13 (20.97) 7 (23.33)
Stomach 12 (13.04) 10 (16.13) 2 (6.67)
Rectal 10 (10.87) 7 (11.29) 3 (10.00)
Pancreas 9 (9.78) 4 (6.45) 5 (16.67)
Liver 5 (5.43) 5 (8.06) 0 (0.00)
Kidney 5 (5.43) 4 (6.45) 1 (3.33)
Head & neck 5 (5.43) 4 (6.45) 1 (3.33)
Lymphoma 4 (4.35) 2 (3.23) 2 (6.67)
Breast 3 (3.26) 0 (0.00) 3 (10.00)
Thyroid 1 (1.09) 0 (0.00) 1 (3.33)
Other 22 (23.91) 15 (24.19) 7 (23.33)
Cancer stage
Stage I∼II 3 (3.26) 1 (1.61) 2 (6.67) Stage III 15 (16.3) 5 (8.06) 6 (20.00) Stage IV 74 (80.43) 52 (83.87) 22 (73.33) Current anticancer treatment
None 47 (51.09) 29 (46.77) 18 (60.00)
At least one 45 (48.91) 33 (53.23) 12 (40.00)
Surgery 2 (4.44) 1 (3.03) 1 (8.33)
Chemotherapy 41 (91.11) 31 (93.94) 10 (83.33) Radiation 9 (20.00) 7 (21.21) 2 (16.67)
Others 1 (2.22) 0 (0.00) 1 (8.33)
ECOG PS 1.53±0.72 1.41±0.67 1.77±0.77
Pain intensity (NRS 0∼10) 5.61±1.56 5.52±1.45 5.80±1.77 Type of pain
Somatic 66 (71.74) 46 (74.19) 20 (66.67) Visceral 43 (46.74) 27 (43.55) 16 (53.33) Neuropathic 23 (25.00) 11 (17.74) 12 (40.00) Source of pain
Cancer-related 86 (93.48) 60 (96.77) 26 (86.67) Treatment-related 19 (20.65) 10 (16.13) 9 (30.00)
Other 8 (8.70) 3 (4.84) 5 (16.67)
Pattern of prescription
Oxycodone only 70 (76.09) 51 (82.26) 19 (63.33)
Mixed 12 (13.04) 6 (9.68) 6 (20.00)
Switched 10 (10.87) 5 (8.06) 5 (16.67) N: number of patients, SD: standard deviation, ECOG PS: Eastern Cooperative Oncology Group performance status, NRS: Numeric Rating Scale.
QoL at 24 h before the visit. Patients also provided clinical information on their average pain using the NRS (scores from 0∼10) and on the presence of symptoms associated with opioid therapy. We assessed the opioid dosage by us- ing the mean opioid dosage, expressed as OMEs, and the use of adjuvant analgesics. According to the Ministry of Health and Welfare Cancer Pain Management Guidelines in Korea, 120 mg of oral morphine is equivalent to 80 mg of oral oxycodone or 24 mg of oral hydromorphone, and has a potency of 120 OMEs.22) Assessments were performed at each visit over the 8-week period (at least two visits, one at the beginning of the study and one after the 8-week period, with additional visits depending on the pain of the patient).
The presence of symptoms associated with opioid therapy and changes in the prescriptions for opioid, non-opioid, and adjuvant analgesics were examined during the 8 weeks.
Patients could receive opioids with adjuvant analgesics as rescue medications during the 8 weeks, and opioids were ti- trated until an effective dose was obtained.
3. Statistical analysis
The demographic characteristics of the study subjects, their pain characteristics, and their ECOG PS at baseline are presented as the means and standard deviations or as numbers with percentages. We compared the pain intensity, ECOG PS, QoL parameters, and CR oxycodone dosages be- tween baseline and 8 weeks using paired t-tests. We com- pared pain and symptom control by opioid type after 8 weeks. Additionally, we assessed the frequency of adverse events resulting from the use of opioids and the prevalence of serious adverse events at baseline and 8 weeks. We de- termined the frequency of adverse events from opioid use using McNemer’s test. A P value of <0.05 was considered significant. All statistical analyses were performed using SAS ver. 9.2 (SAS Institute, Cary, NC, USA).
RESULTS
1. Patient population and clinical characteristics We enrolled a total of 94 patients: 92 were followed-up for 8 weeks and two dropped out because they stopped
opioid treatment. As shown in Table 1, 62 (67%) of the patients were men and 30 (32.6%) were women. The pri- mary diagnoses were lung cancer (21.7%), stomach cancer (13.0%), and rectal cancer (10.9%). The mean age of the
Table 2. Frequency of adverse events with the use of high-dose opioids in elderly patients with cancer (N=92)
Adverse events N (%)
P value Baseline 8 weeks
Constipation 28 (63.64) 26 (65.00) 0.2188
Dizziness 10 (22.73) 3 (7.50) 0.0391*
Nausea 9 (20.45) 5 (12.50) 0.6875
Dry mouth 7 (15.91) 2 (5.00) 0.0625
Vomiting 4 (9.09) 3 (7.50) 0.6250
Asthenia 3 (6.82) 3 (7.50) 1.0000
Somnolence 3 (6.82) 2 (5.00) 1.0000
Urinary retention 3 (6.82) 1 (2.50) 1.0000
Sweating 1 (2.27) 0 (0.00) -
Hypotension 1 (2.27) 0 (0.00) -
Respiratory depression 0 (0.00) 1 (2.50) -
Delusion 0 (0.00) 0 (0.00) -
Headache 0 (0.00) 0 (0.00) -
Pruritus 0 (0.00) 0 (0.00) -
Other 8 (18.18) 10 (25.00) 0.3438
Total 44 (47.83) 40 (43.48) 0.3458
*Statistically significant.
participants was 70.17±4.39 years (69.61±4.19 years for men and 71.33±4.63 years for women). The mean ECOG PS was 1.53±0.72. The mean NRS score was 5.61±1.56.
At baseline, 70 (76.1%) patients were only taking CR oxy- codone, 12 (13.0%) were taking other medications with CR oxycodone, and 10 (10.9%) had switched from CR oxy- codone to other opioid medications.
2. Safety and toxicity of high-dose opioids in elderly patients with cancer
Most of the adverse effects were mild to moderate at the 8-week follow-up. As shown in Table 2, 44 patients (47.8%) reported adverse effects at baseline including constipation (63.6%), dizziness (22.7%), and nausea (20.5%). After 8 weeks, 40 (43.5%) patients reported adverse effects includ- ing constipation (65.0%), nausea (12.5%), and dizziness (7.5%). The frequencies of adverse events from opioid use were not different between baseline and 8 weeks, except for dizziness. As shown in Table 2, dizziness decreased sig- nificantly after 8 weeks of opioid use (P=0.039). Drugs such as anti-emetics and laxatives were prescribed for adverse events. Of the 92 patients, 25 received anti-emetics and 52 received laxatives at baseline. After 8 weeks, 23 patients
had received anti-emetics, including 17 patients who had re- ceived baseline treatment and six new patients. Fifty-nine of the 92 patients were treated with laxatives, including 45 who had received baseline treatment and 14 new patients.
No opioid-related deaths occurred during the study period.
We evaluated the frequency of adverse events according to increases in the patients’ capacity for CR oxycodone.
Adverse effects were reported by 44 patients (47.8%) at baseline including constipation, dizziness, nausea, and vomiting.
Adverse effects were reported by 37 patients (40.2%) who had a mean opioid dosage greater than 120 OME but less than 240 OME, six patients (6.5%) with a dosage greater than 240 OME but less than 480 OME, and one patient (1.1%) with a dosage greater than 480 OME. The occur- rence of adverse effects after 8 weeks was reported by 40 patients (43.5%) including 33 patients who complained of adverse events at baseline and seven new patients. Adverse effects were reported by 32 patients (34.8%) with a mean opioid dosage greater than 120 OME but less than 240 OME, seven patients (7.6%) with a dosage greater than 240 OME but less than 480 OME, and one patient (1.1%) with a dosage greater than 480 OME. No significant differ- ences in the percent frequency of adverse events were ob- served based on the opioid dose between baseline and 8 weeks.
We compared the adverse events of CR oxycodone with those of other opioids. Of the 92 patients who received opioids, 70 received only CR oxycodone, 12 received CR oxycodone and another opioid, and 10 received opioids oth- er than CR oxycodone. Of the 70 patients who received on- ly CR oxycodone, 28 (40.0%) experienced adverse effects; of the 10 patients who received an opioid other than CR oxy- codone, seven (70.0%) reported adverse effects. Constipation, dizziness, and nausea were the most frequently reported opioid-related adverse events. No significant differences in the percent frequency of adverse events were observed by opioid type between baseline and 8 weeks.
3. Efficacy of high-dose opioids in elderly patients with cancer
The pain intensity, as rated using the NRS, improved
Table 3. Changes in pain severity, opioid dosage, and quality of life parameters during the use of high-dose opioids in elderly patients with cancer (N=92)
OME at Baseline Mean±SD/N (%)
P value
Baseline 8 weeks
Pain intensity (NRS 0∼10) OME≥120 5.61±1.56 4.02±2.16 <0.0001*
120≤OME<240 5.38±1.50 3.73±2.15
240≤OME 6.38±1.53 5.00±1.95
Mean dosage (OME) OME≥120 178.86±76.88 288.54±389.09 0.0025*
120≤OME<240 145.56±27.35 191.77±136.74
240≤OME 291.43±83.86 615.71±691.19
ECOG PS OME≥120 1.53±0.71 1.48±0.78 0.4868
120≤OME<240 1.49±0.69 1.51±0.81
240≤OME 1.66±0.80 1.38±0.67
Quality of life
Daily activity OME≥120 5.00±1.96 3.85±2.32 <0.0000*
120≤OME<240 4.76±1.93 3.58±2.33
240≤OME 5.81±1.86 4.76±2.10
Ambulation OME≥120 4.20±2.38 3.39±2.52 0.0012*
120≤OME<240 3.82±2.24 3.14±2.51
240≤OME 5.48±2.42 4.24±2.41
Sleep OME≥120 3.79±2.67 2.46±2.32 <0.0001*
120≤OME<240 3.58±2.58 2.17±2.14
240≤OME 4.52±2.93 3.43±2.69
N: number of patients, OME: oral morphine equivalent, SD: standard deviation, NRS: Numeric Rating Scale, ECOG PS: Eastern Cooperative Oncology Group performance status. *Statistically significant. P values were calculated with the paired t-test.
Figure 2. Mean opioid dosage (oral morphine equivalent) based on the change in pain severity in elderly patients with cancer (N=92).
from a score of 5.61±1.56 at baseline to 4.02±2.16 (P<
0.0001) at 8 weeks. As for the patients’ QoL, their ratings for pain intensity in their daily activities decreased from 5.00±1.96 at baseline to 3.85±2.32 at 8 weeks (P<0.0001), those for ambulation decreased from 4.20±2.38 to 3.39±
2.52 (P=0.0012), and those for sleep decreased from 3.79±
2.67 to 2.46±2.32 (P<0.001). The mean opioid dose increased significantly from 178.86±76.88 OME to 288.54±389.09 OME (P=0.0025; Table 3). We isolated the effects of CR oxycodone and compared them to the effects of other opioid analgesic medications that were used for pain control. The mean pain intensity, ECOG PS, QoL, and opioid dose were not significantly different between the CR oxycodone only group and the group that used other opioid medications.
The frequency of adjuvant analgesic use was not different between the groups.
The pain intensity of 57 patients with moderate to severe cancer pain decreased and their mean opioid dosage in- creased from 173.68 to 247.47 OME (Figure 2). The pain intensities of 17 patients did not change despite an increase
in their mean opioid dosage from 201.18 to 458.33 OME.
For 18 patients, their pain intensity increased even after re- ceiving an increase in their mean opioid dosage. Opioid res- cue medications
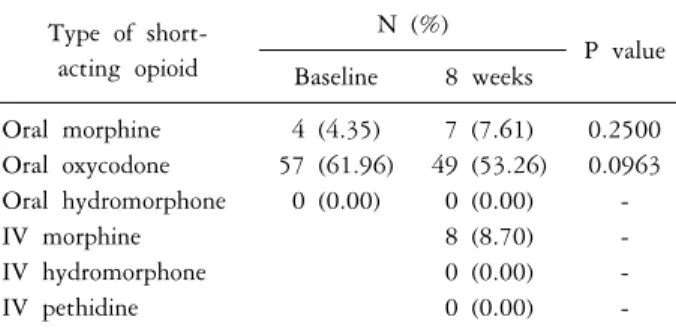
Immediate-release oxycodone was used as the rescue med- ication for most patients. Initially, 61 (66.3%) patients re-
Table 4. Use of short-acting opioids in elderly patients with cancer
Type of short- acting opioid
N (%)
P value Baseline 8 weeks
Oral morphine 4 (4.35) 7 (7.61) 0.2500 Oral oxycodone 57 (61.96) 49 (53.26) 0.0963 Oral hydromorphone 0 (0.00) 0 (0.00) -
IV morphine 8 (8.70) -
IV hydromorphone 0 (0.00) -
IV pethidine 0 (0.00) -
N: number of patients, IV: intravenous. *Statistically significant.
P values were calculated with the General Linear Model.
ceived at least one dose of rescue medication, 57 consumed immediate-release oxycodone, and four consumed oral mor- phine as a rescue medication. Immediate-release oxycodone was commonly used after 8 weeks (Table 4). No significant changes in rescue-medication use (number, amount, or type) were observed between baseline and 8 weeks.
DISCUSSION
Oxycodone, hydromorphone, fentanyl, buprenorphine, and methadone have been prescribed at similar levels to those of morphine since the 1990s; in particular, the number of pre- scriptions for oxycodone has increased tremendously. Here, CR oxycodone was also used effectively and safely in elderly patients with cancer pain, supporting that high-dose CR oxycodone for cancer-pain management in the elderly is ef- fective, safe, and tolerable.
The common adverse events of oxycodone use include nausea, headache, constipation, and dizziness. While intoxication coma, pulmonary edema, or cardiovascular failure may ap- pear in severe cases and cause death, these severe adverse events are rare.23) Comparative studies revealed that CR oxycodone significantly improved the QoL of patients with osteoarthritis, including their mood, sleep, enjoyment of life, and physical activities.24) Oxycodone in larger doses was also considered safe and effective in a palliative care unit25) and an outpatient clinic.17) Thus, the efficacy and tolerability of oxycodone are superior to those of other strong opioids in- cluding morphine sulfate, codeine, and tramadol for can-
cer-related pain.26)
Here, none of the subjects’ laboratory analyses, electro- cardiogram results, or physical examinations showed any of the previously reported adverse events related to the use of CR oxycodone, thus pain control and the acceptability of oxycodone therapy were maintained at satisfactory levels.23,27) Moreover, we found that 47.8% (44/92) of the patients re- ported adverse effects at baseline and 43.5% (40/92) noted adverse effects from opioid use after 8 weeks. These adverse effects are typically reported by patients treated with opioid medications.9,14,26) Oxycodone-related neurological symptoms, including drowsiness, lightheadedness, and dizziness, oc- curred less often than did gastrointestinal symptoms.28,29) In the present study, the observed serum concentrations of oxycodone and its corresponding metabolites were not asso- ciated with toxicity. As the dosage of CR oxycodone in- creased, the patients’ pain intensity lessened and their QoL improved, while the frequency of adverse effects did not increase.
The physicians increased the CR oxycodone dose accord- ing to the frequency and intensity of pain, although some patients still complained of pain, hence short-acting opioids had to be prescribed. In our study, 57 patients with moder- ate to severe cancer pain improved, but 35 patients, includ- ing 18 patients with more intense pain compared to that at baseline, continued to experience pain even after receiving an increase in their mean opioid dosage. The pain intensity of 57 patients with moderate to severe cancer pain de- creased and their mean opioid dosage increased from 173.68 to 247.47 OME. However, the pain intensity of 17 patients did not change despite an increase in their mean opioid dosage from 201.18 to 458.33 OME, and 18 patients expe- rienced worse (more intense) pain after receiving an increase in their mean opioid dosage. These findings indicate that cancer pain is complex owing to the influence of numerous factors including a patient’s emotional and psychosocial status.30) One of the purposes of pain management strategies for pa- tients with cancer is to improve their QoL; accordingly, the elderly patients with cancer in our study had an improved QoL following the use of high-dose opioids for pain control.
At baseline, three patients with stage II cancer, 15 with
stage III cancer, and 74 with stage IV cancer suffered mod- erate to severe pain in our study. After 8 weeks, two pa- tients with stage II cancer and moderate to severe pain im- proved, whereas one patient continued to experience pain even after receiving an increased opioid dosage. The pain of the four patients with stage III cancer who were experienc- ing moderate to severe pain improved to a mild rating, but six patients complained of moderate pain, and five patients continued to experience severe pain even after receiving an increased opioid dosage. Patients with stage II and III can- cers did not undergo a curative operation, percutaneous electrical nerve stimulation, spinal nerve block, surgical spi- nal-cord tractotomy, vertebroplasty, or any other comple- mentary therapy.
This study had several limitations. Firstly, the follow-up period was short; hence, data from long-term follow-ups are necessary to confirm our findings. Secondly, we could not estimate the changes in analgesic use that were due to ad- verse effects alone. Changes in analgesics, such as switching opioid type and the use of an adjuvant or rescue drugs in addition to opioids, were due to numerous associated fac- tors, including patient preference and the aggravation of a patient’s general condition according to their underlying cancer status. Furthermore, the present findings are based on elderly patients who had a poorer ECOG PS and a dis- ease that was more progressive. Finally, our study did not include a control group and was unable to clearly determine the causal relationship between the opioid dosage and in- cidence of side effects.
Despite the above-mentioned limitations, our findings from a non-interventional observational study in Korea sug- gest that the use of high-dose CR oxycodone for cancer-pain management in the elderly is effective, safe, and tolerable.
According to this observation, administering high-dose opioids to elderly individuals with cancer can reduce their pain in- tensity and improve their QoL including their daily living activities, ambulation, and sleep; however, close monitoring of adverse events is necessary for elderly patients with cancer.
Further studies should be performed, particularly regarding the use of high-dose opioids in elderly patients with cancer that have more complex pain situations.
REFERENCES
1. Jung KW, Won YJ, Kong HJ, Oh CM, Seo HG, Lee JS.
Cancer statistics in Korea: incidence, mortality, survival and prevalence in 2010. Cancer Res Treat 2013;45:1-14.
2. Plante GE, VanItallie TB. Opioids for cancer pain: the chal- lenge of optimizing treatment. Metabolism 2010;59:S47-S52.
3. Bernabei R, Gambassi G, Lapane K, Landi F, Gatsonis C, Dunlop R, et al. Management of pain in elderly patients with cancer. SAGE Study Group. Systematic assessment of geri- atric drug use via epidemiology. JAMA 1998;279:1877-82.
4. McGrath PA. Development of the World Health Organiza- tion Guidelines on Cancer pain relief and palliative care in children. J Pain Symptom Manage 1996;12:87-92.
5. Deandrea S, Montanari M, Moja L, Apolone G. Prevalence of undertreatment in cancer pain. A review of published literature. Ann Oncol 2008;19:1985-91.
6. Pergolizzi J, Böger RH, Budd K, Dahan A, Erdine S, Hans G, et al. Opioids and the management of chronic severe pain in the elderly: consensus statement of an International Expert Panel with focus on the six clinically most often used World Health Organization Step III opioids (buprenorphine, fentan- yl, hydromorphone, methadone, morphine, oxycodone). Pain Pract 2008;8:287-313.
7. Jost L, Roila F, ESMO Guidelines Working Group. Manage- ment of cancer pain: ESMO Clinical Practice Guidelines. Ann Oncol 2010;21:v257-60.
8. Pasternak GW. Molecular biology of opioid analgesia. J Pain Symptom Manage 2005;29:S2-S9.
9. Vella-Brincat J, Macleod AD. Adverse effects of opioids on the central nervous systems of palliative care patients. J Pain Palliat Care Pharmacother 2007;21:15-25.
10. Melton LJ 3rd, Khosla S, Crowson CS, O’Connor MK, O’Fallon WM, Riggs BL. Epidemiology of sarcopenia. J Am Geriatr Soc 2000;48:625-30.
11. Gibson MC, Schroder C. The many faces of pain for older, dying adults. Am J Hosp Palliat Care 2001;18:19-25.
12. Gianni W, Ceci M, Bustacchini S, Corsonello A, Abbatecola AM, Brancati AM, et al. Opioids for the treatment of chronic non-cancer pain in older people. Drugs Aging 2009;26:63-73.
13. Launay-Vacher V, Oudard S, Janus N, Gligorov J, Pourrat X, Rixe O, et al. Renal Insufficiency and Cancer Medications (IRMA) Study Group. Prevalence of renal insufficiency in cancer patients and implications for anticancer drug manage- ment: the renal insufficiency and anticancer medications (IRMA) study. Cancer 2007;110:1376-84.
14. Hamerman D, Berman JW, Albers GW, Brown DL, Silver D. Emerging evidence for inflammation in conditions fre- quently affecting older adults: report of a symposium. J Am Geriatr Soc 1999;47:1016-25.
15. Azoulay D, Jacobs JM, Cialic R, Mor EE, Stessman J. Opioids, survival, and advanced cancer in the hospice setting. J Am Med Dir Assoc 2011;12:129-34.
16. Bengoechea I, Gutiérrez SG, Vrotsou K, Onaindia MJ, Lopez
JM. Opioid use at the end of life and survival in a hospital at home unit. J Palliat Med 2010;13:1079-83.
17. Baek SK, Shin HW, Choi YJ, Zang DY, Cho DY, Ryoo HM, et al. Noninterventional observational study using high- dose controlled-release oxycodone (CR oxycodone) for cancer pain management in outpatient clinics. Pain Med 2013;14:
1866-72.
18. Caraceni A, Cherny N, Fainsinger R, Kaasa S, Poulain P, Radbruch L, et al. Pain measurement tools and methods in clinical research in palliative care: recommendations of an Expert Working Group of the European Association of Palliative Care. J Pain Symptom Manage 2002;23:239-55.
19. Hanks G, Cherny NI, Christakis NA, Fallon M, Kassa S, Portenoy RK. Oxford textbook of palliative medicine. 4th ed.
New York: Oxford University Press; 2011.
20. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982;5:649-55.
21. Yun YH, Park YS, Lee ES, Bang SM, Heo DS, Park SY, et al. Validation of the Korean version of the EORTC QLQ-C30.
Qual Life Res 2004;13:863-8.
22. Ministry of Health and Welfare. Cancer pain management guideline. Seoul: Ministry of Health and Welfare in Korea;
2006.
23. Smith K, Hopp M, Mundin G, Leyendecker P, Bailey P, Grothe B, et al. Single- and multiple-dose pharmacokinetic evaluation of oxycodone and naloxone in an opioid ago- nist/antagonist prolonged-release combination in healthy adult
volunteers. Clin Ther 2008;30:2051-68.
24. Taylor R Jr, Raffa RB, Pergolizzi JV Jr. Controlled release formulation of oxycodone in patients with moderate to severe chronic osteoarthritis: a critical review of the literature. J Pain Res 2012;5:77-87.
25. Mercadante S, Ferrera P, David F, Casuccio A. The use of high doses of oxycodone in an acute palliative care unit. Am J Hosp Palliat Care 2011;28:242-4.
26. Wang YM, Liu ZW, Liu JL, Zhang L. Efficacy and toler- ability of oxycodone in moderate-severe cancer-related pain: a meta-analysis of randomized controlled trials. Exp Ther Med 2012;4:249-54.
27. Citron ML, Kaplan R, Parris WC, Croghan MK, Herbst LH, Rosenbluth RJ, et al. Long-term administration of controlled- release oxycodone tablets for the treatment of cancer pain.
Cancer Invest 1998;16:562-71.
28. Andreassen TN, Klepstad P, Davies A, Bjordal K, Lundström S, Kaasa S, et al. Is oxycodone efficacy reflected in serum concentrations? A multicenter, cross-sectional study in 456 adult cancer patients. J Pain Symptom Manage 2012;43:694- 705.
29. Anastassopoulos KP, Chow W, Ackerman SJ, Tapia C, Benson C, Kim MS. Oxycodone-related side effects: impact on degree of bother, adherence, pain relief, satisfaction, and quality of life. J Opioid Manag 2011;7:203-15.
30. Fischer DJ, Villines D, Kim YO, Epstein JB, Wilkie DJ.
Anxiety, depression, and pain: differences by primary cancer.
Support Care Cancer 2010;18:801-10.
Appendix 1. Institutions that participated in this study 1. Ajou University Medical Center
2. Bobath Memorial Hospital 3. Changwon Fatima Hospital
4. Chonnam National University Hospital 5. Chosun University Hospital
6. Chungnam National University Hospital 7. Daegu Catholic University Medical Center 8. Dankook University Hospital
9. Dong-A University Medical Center 10. Dongguk University Gyeongju Hospital 11. Ewha Womens University Tongdaemun Hospital 12. Gyeongsang National University Hospital 13. Inha University Hospital
14. Inje University Pusan Paik Hospital 15. Inje University Sanggye Paik Hospital 16. Inje University Seoul Paik Hospital 17. Kangbuk Samsung Medical Center 18. Kangdong Sacred Heart Hospital
19. Keimyung University Dongsan Medical Center 20. Konyang University Hospital
21. Korea University Ansan Hospital 22. Korea University Guro Hospital 23. Korea University Anam Hospital 24. Kwangju Christian Hospital 25. Kyung Hee Medical Center
26. Kyungpuk National University Hospital 27. Maryknoll Hospital
28. Pusan National University Hospital 29. Seoul National University Hospital
30. Soonchunhyang University Cheonan Hospital 31. Sunlin Hospital Handong University
32. The Catholic University of Korea Daejeon St. Mary’s Hospital 33. The Catholic University of Korea Holy Family Hospital 34. The Catholic University of Korea Kangnam St. Mary’s Hospital 35. The Catholic University of Korea St. Mary’s Hospital
36. The Catholic University of Korea Uijeongbu St. Mary’s Hospital 37. Ulsan University Hospital
38. Yeungnam University Medical Center