ISSN 0378-6471 (Print)⋅ISSN 2092-9374 (Online)
https://doi.org/10.3341/jkos.2020.61.1.41
Original Article
당뇨황반부종에서 유리체 내 주사제에 따른 치료 전후 고반사점 변화 비교
Comparision of Hyperreflective Foci after Treatment of Diabetic Macular Edema Patients between Intravitreal Injections
김민진1⋅박기범1⋅이명연2⋅이성진1
Minjin Kim, MD1, Kibum Park, MD1, Myeong Yeon Yi, MD2, Sung Jin Lee, MD, PhD1
순천향대학교 의과대학 서울병원 안과학교실1, 수안과의원2
Department of Ophthalmology, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine1, Seoul, Korea Soo Eye Clinic2, Seoul, Korea
Purpose: To compare the outcomes in patients with diabetic macular edema (DME) treated with intravitreal dexamethasone im- plants and intravitreal bevacizumab injections.
Methods: A retrospective cohort study was designed using 66 patients with DME treated with intravitreal dexamethasone (n = 35; 35 eyes) and intravitreal bevacizumab (n = 31; 31 eyes). Post-treatment changes in hyperreflective foci in the inner and outer retina were characterized using optical coherence tomography, central macular thickness, outer limiting membrane, and photo- receptor inner segment-outer segment junctions. Visual acuities were analyzed 4 weeks after bevacizumab injections and 8 weeks after dexamethasone injections.
Results: Both groups showed a decrease in the number of hyperreflective foci after treatment: from 10.6 ± 11.8 to 6.3 ± 5.9 (p = 0.005) in the intravitreal dexamethasone implant group and from 11.6 ± 8.5 to 7.7 ± 6.7 (p < 0.001) in the intravitreal bev- acizumab injection group. The mean central macular thickness in the dexamethasone group changed significantly from 586.8 μm to 297.7 μm after treatment and the visual acuity improved significantly from 0.33 logMAR to 0.38 logMAR after treatment (p < 0.001 and p = 0.018, respectively). The mean central macular thickness in the bevacizumab group showed a significant de- crease from 467.1 μm to 353.2 μm after treatment (p < 0.001), but there was no significant change in the visual acuities: 0.34 logMAR to 0.32 logMAR after treatment (p = 0.464).
Conclusions: Both intravitreal dexamethasone implants and bevacizumab treatments in patients with DME showed improved outcomes including a decrease in hyperreflective foci shown by optical coherence tomography.
J Korean Ophthalmol Soc 2020;61(1):41-50
Keywords: Bevacizumab, Dexamethasone, Diabetic macular edema, Hyperreflective foci
■Received: 2019. 7. 4. ■ Revised: 2019. 8. 16.
■Accepted: 2019. 12. 30.
■Address reprint requests to Sung Jin Lee, MD, PhD Department of Ophthalmology, Soonchunhyang University Seoul Hospital, #59 Deasakwan-ro, Yongsan-gu, Seoul 04401, Korea
Tel: 82-2-709-9354, Fax: 82-2-710-3196 E-mail: [email protected]
*Conflicts of Interest: The authors have no conflicts to disclose.
ⓒ2020 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
당뇨망막병증환자들에서 당뇨황반부종은 의미 있는 시 력 손상을 일으키는 가장 흔한 원인이다.1 당뇨황반부종은 혈액-망막장벽기능의 감소로 혈관벽의 투과성이 증가하여 혈장의 누출 및 혈장단백질의 혈관 외 침착에 의해 발생한 다. 다양한 생화학적, 분자생물학적 기전에 의한 저산소증, 혈류 변화, 망막 허혈, 염증 반응 등이 발생기전에서 매우 중요한 역할을 하는 것으로 알려져 있다.2-4
스펙트럼영역 빛간섭단층촬영(spectral-domain optical co-
herence tomography, SD-OCT)은 망막을 구성하는 각 층별 형태의 고해상도 영상을 얻고 두께를 객관적으로 측정하는 비침습적 도구로 널리 이용되고 있으며,5 이러한 빛간섭단 층촬영에서 관찰되는 고반사점(hyperreflective foci)이 당뇨 망막병증, 황반변성, 망막분지정맥폐쇄 등 여러 질환들에서 보고되고 있다.6-8 혈관 망막장벽에서 누출된 지단백질로 경 성삼출물의 전구체라는 견해와 염증 환경으로 인해 활성화 된 미세아교세포 또는 광수용체세포의 퇴행산물이라는 견 해 등 고반사점의 기전에 대한 여러 가설들이 제시되고 있 으나 정확히 밝혀진 바는 없다.6,9,10
당뇨황반부종의 치료에 있어서 혈관내피세포 성장인자 억제제 주사 치료 후 고반사점의 개수가 감소하였다는 보 고가 있었으며,7 유리체내 베바시주맙주입술과 비교하여 덱사메타손삽입물이 치료 횟수와 해부학적 결과 면에서 이 점이 있음을 보여준 연구도 있었다.11 이에 본 연구에서는 당뇨황반부종에서 위치에 따라 고반사점을 분류하고 유리 체내 베바시주맙주입술 또는 덱사메타손삽입물 치료 후 고 반사점, 망막의 미세구조, 중심황반두께 및 시력 변화를 비 교하고자 하였다.
대상과 방법
2013년 1월부터 2015년 12월까지 당뇨황반부종을 진단 받은 후 유리체내 베바시주맙주입술 또는 덱사메타손삽입 물을 1회 시행 받은 환자 66명 66안을 대상으로 후향적 의 무기록 조사를 시행하였다. 양안이 모두 포함 가능한 환자 의 경우 단안만을 무작위로 선정하여 분석하였다. 위 연구 는 순천향대학교 서울병원 임상연구윤리위원회의 승인(승 인 번호: 2019-06-021)을 받았다. 황반부종을 일으킬 수 있 거나 시력에 영향을 줄 수 있는 다른 안질환이 있는 경우, 최근 1년 이내 백내장수술이나 유리체수술 과거력이 있는 경우, 각막혼탁, 심한 백내장, 유리체출혈 등 매체 혼탁이 있는 경우, 스펙트럼빛간섭단층촬영 사진에서 미세구조를 구분하기 어려운 화질을 보이는 경우는 대상에서 제외하였 다.
모든 대상 환자를 초진 시 최대교정시력(logMAR), 안압 을 측정하였고 세극등현미경검사와 안저검사를 시행하였 다. 빛간섭단층촬영(Spectralis OCT, Heidelberg engineer- ing, Inc, Heidelberg, Germany)은 산동제 점안 후 어두운 방에서 한 명의 숙련된 검사자에 의해 시행되었다. 중심황 반두께는 volume scan data로부터 계산된, 중심으로부터 반 경 500 μm 원 안의 평균 망막두께인 center subfield mean thickness로 정의하였다. 외경계막과 타원체영역(ellipsoid zone)의 손상 정도는 중심와로부터 좌우 750 μm 이내의 범
위에서 평가하였고 연속적인 고반사 선이 유지되는 경우를 정상, 50% 미만의 결손 또는 비연속 구간이 관찰되는 경우 를 부분 손상, 50% 이상의 결손 또는 비연속 구간이 관찰 되는 경우를 완전 손상으로 정의하였다. 망막하액의 유무 또한 평가하였다.
고반사점의 개수는 중심와를 통과하는 horizontal scan의 중심와 좌우 750 μm 이내의 범위에서 두 명의 판독자가 측 정하였으며 두 판독 결과의 평균값을 연구에 사용하였다. 고반사점은 경계가 명확하고 반사 정도는 망막색소상피와 같거나 강하며 크기는 지름 20-40 μm의 점으로 정의하였 다. 지름 20 μm 이하의 경우 잡음신호와 구분이 어려웠고, 40 μm를 초과하는 경우 안저 사진에서 전형적인 경성삼출 물과 일치하여 배제하였다. 위치에 따라 내망막(내경계막- 외과립층), 외망막(외경계막-타원체영역), 망막하(망막하액~
망막색소상피층)의 세 군으로 분류하였다.
두 약제 간의 치료 효과가 최대인 시기의 차이가 있음을 고려하여, 유리체내 베바시주맙(Avastin®, Genetech Inc., San Francisco, CA, USA) 주입술은 1.25 mg/0.05 mL의 용량으 로 시행 후 4주째, 유리체내 덱사메타손(Ozurdex®, Allergan, Irvine, CA, USA) 삽입물은 0.7 mg의 용량으로 시행 후 8주 째 최대교정시력, 안압검사, 안저촬영 및 스펙트럼빛간섭단 층촬영 검사를 시행하였으며, 술 전과 술 후 최대교정시력, 안압, 중심황반두께, 망막하액 유무, 외경계막, 타원체영역, 위치에 따른 고반사점 개수의 변화를 관찰하였다.
통계분석은 SPSS version 18.0 (SPSS Inc., Chicago, IL, USA)을 이용하였다. 치료 전과 후의 각 인자들의 수치 비 교를 위해 paired t-test와 McNemer-Bowker test를, 두 군 간의 각 인자들의 수치 비교를 위해 independent t-test와 Fisher’s exact test를 이용하였다. 치료 전 인자들과 치료 후 시력 및 중심황반두께 변화량의 연관성은 각 그룹의 치료 전후의 값을 계산하여 두 그룹 간의 차이를 가지는 종속변 수(시력, 안압, 중심황반두께, 고반사점 개수, 망막하액, 외 경계막 결손, 타원체영역 결손)를 탐색하였다. 치료 전 고 반사점의 개수와 치료 시작 전의 중심황반두께, 시력의 호 전과 황반부종의 감소 정도에 대한 상관관계를 Spearman rank correlation으로 분석하였다. 이때, p값이 0.05 미만인 경우를 통계적으로 유의한 것으로 간주하였다.
결 과
총 66명 66안의 대상군 중 남자 41명, 여자 25명이었고 평균 연령은 62.3 ± 11.2세였다. 유리체내 베바시주맙주입 술군에 31명, 덱사메타손삽입물군에 35명이 해당하였다.
치료 전의 최대교정시력은 베바시주맙주입술군이 0.34 ±
Characteristic Bevacizumab (n = 31)
Dexamethasone
implant (n = 35) p-value*
Age (years) 63.5 ± 10.7 61.0 ± 11.9 0.416
Sex (male:female) 14:17 27:8 0.026
Right:left 16:15 16:19 0.817
VA (logMAR) 0.34 ± 0.21 0.33 ± 0.26 0.820
HTN (eyes) 13 (41.9) 16 (45.7) 0.847
Duration of diabetes (years) 13.52 ± 9.2 15.17 ± 9.5 0.179
HbA1c (%) 8.3 ± 1.4 8.2 ± 1.4 0.230
DMR grading (moderate to severe NPDR:PDR) 20:15 17:14 0.857
PRP status (eyes) 12 (38.7) 14 (40.0) 0.915
Pretreatment
Intravitreal anti-VEGF (Avastin) 14 17 0.782
Subconjunctival steroid (triamcinolone) 1 2 0.628
IOP (mmHg) 15.5 ± 3.00 17.7 ± 2.80 0.004
CMT (μm) 467.1 ± 124.4 586.8 ± 204.7 0.005
Number of HF
Inner 10.0 ± 7.6 7.9 ± 7.9 0.272
Outer 1.5 ± 1.9 1.8 ± 2.4 0.486
Subretina 0.2 ± 0.5 0.9 ± 3.5 0.228
Total 11.6 ± 8.5 10.6 ± 11.8 0.692
Values are presented as mean ± standard deviation or number (%) unless otherwise indicated.
VA = visual acuity; logMAR = the log of the minimum angle resolution; HTN = hypertension; DMR = diabetic retinopathy; NPDR = non proliferative diabetic retinopathy; PDR = proliferative diabetic retinopathy; PRP = panretinal photocoagulation; VEGF = vascular endothe- lial growth factor; IOP = intraocular pressure; CMT = central macular thickness; HF = hyperreflective foci.
*Categorical variables compared using the chi-square test, and continuous variables with the independent t-test.
Table 1. Basic characteristics according to treatment group
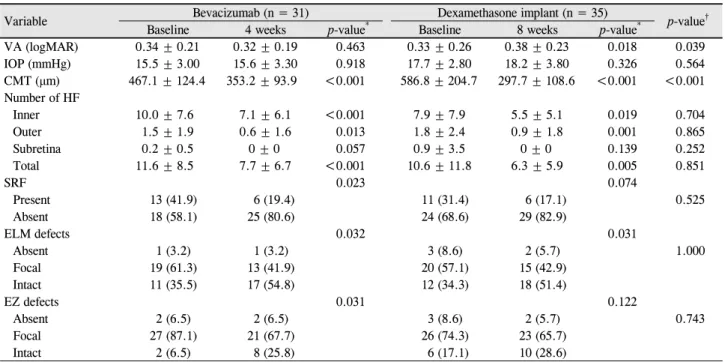
Variable Bevacizumab (n = 31) Dexamethasone implant (n = 35) p-value†
Baseline 4 weeks p-value* Baseline 8 weeks p-value*
VA (logMAR) 0.34 ± 0.21 0.32 ± 0.19 0.463 0.33 ± 0.26 0.38 ± 0.23 0.018 0.039
IOP (mmHg) 15.5 ± 3.00 15.6 ± 3.30 0.918 17.7 ± 2.80 18.2 ± 3.80 0.326 0.564
CMT (μm) 467.1 ± 124.4 353.2 ± 93.9 <0.001 586.8 ± 204.7 297.7 ± 108.6 <0.001 <0.001 Number of HF
Inner 10.0 ± 7.6 7.1 ± 6.1 <0.001 7.9 ± 7.9 5.5 ± 5.1 0.019 0.704
Outer 1.5 ± 1.9 0.6 ± 1.6 0.013 1.8 ± 2.4 0.9 ± 1.8 0.001 0.865
Subretina 0.2 ± 0.5 0 ± 0 0.057 0.9 ± 3.5 0 ± 0 0.139 0.252
Total 11.6 ± 8.5 7.7 ± 6.7 <0.001 10.6 ± 11.8 6.3 ± 5.9 0.005 0.851
SRF 0.023 0.074
Present 13 (41.9) 6 (19.4) 11 (31.4) 6 (17.1) 0.525
Absent 18 (58.1) 25 (80.6) 24 (68.6) 29 (82.9)
ELM defects 0.032 0.031
Absent 1 (3.2) 1 (3.2) 3 (8.6) 2 (5.7) 1.000
Focal 19 (61.3) 13 (41.9) 20 (57.1) 15 (42.9)
Intact 11 (35.5) 17 (54.8) 12 (34.3) 18 (51.4)
EZ defects 0.031 0.122
Absent 2 (6.5) 2 (6.5) 3 (8.6) 2 (5.7) 0.743
Focal 27 (87.1) 21 (67.7) 26 (74.3) 23 (65.7)
Intact 2 (6.5) 8 (25.8) 6 (17.1) 10 (28.6)
Values are presented as mean ± standard deviation or number (%).
VA = visual acuity; logMAR = the log of the minimum angle resolution; IOP = intraocular pressure; CMT = central macular thickness;
HF = hyperreflective foci; SRF = subretinal fluid; ELM = external limiting membrane; EZ = ellipsoid zone.
*Categorical variables compared using the McNemar-Bowker test, and continuous variables with the paired t-test; †categorical variables com- pared pre-treatment and post-treatment delta values of each parameter between bevacizumab group and dexamethasone group, using the Fisher’s exact test, and continuous variables with the independent t-test.
Table 2. Comparison of clinical parameters at pre and post-injection between groups
A B
C D
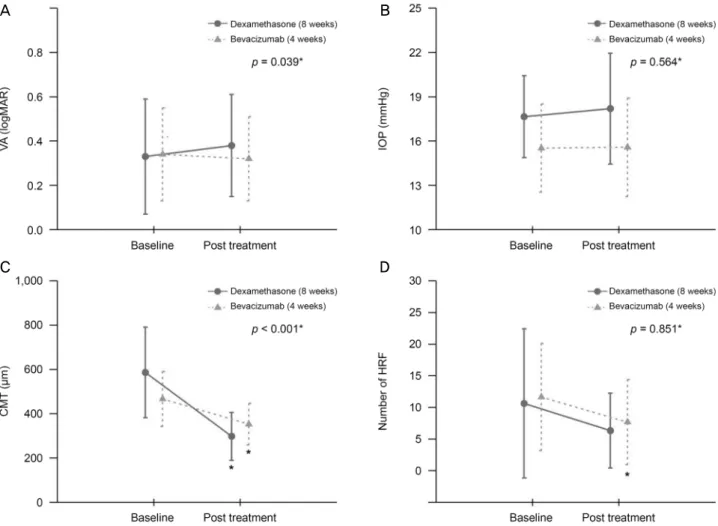
Figure 1. Changes in parameters of both groups after injection. (A) Visual acuity. (B) Intraocular pressure. (C) Spectral domain opti-
cal coherence tomography (SD-OCT) measurements of central macular thickness. (D) SD-OCT measurements of total number of hyperreflective foci. VA = visual acuity; logMAR = the log of the minimum angle resolution; IOP = intraocular pressure; CMT= central macular thickness; HRF = hyperreflective foci. *Categorical variables compared pre-treatment and post-treatment delta values of each parameter between bevacizumab group and dexamethasone group, using the independent t-test.
0.21 logMAR, 덱사메타손삽입물이 0.33 ± 0.26 logMAR, 고반사점 개수는 베바시주맙주입술군이 11.6 ± 8.5개, 덱사 메타손삽입물군이 10.6 ± 11.8개로 두 군 간의 차이는 없었 으며 두 명의 판독자에 따른 고반사점 개수의 편차는 2개 이내였다. 안압은 베바시주맙주입술군이 15.5 ± 3.00 mmHg, 덱사메타손삽입물군이 17.7 ± 2.80 mmHg, 중심황반두께는 베바시주맙주입술군이 467.1 ± 124.4 μm, 덱사메타손삽입 물이 586.8 ± 204.7 μm로 두 군 간 차이를 보였다(Table 1).
치료 후 시력은 치료 전에 비해 베바시주맙주입술군에서 는 유의한 호전을 보이지 않았으나(p=0.463), 덱사메타손삽 입물군에서는 유의한 호전이 있었으며(p=0.018), 두 군에서 시력의 변화 정도 또한 의미 있는 차이를 보였다(p=0.039, Table 2, Fig. 1A). 베바시주맙주입술군과 덱사메타손삽입 물군 모두 주사 전후로 안압의 차이를 보이지 않았고(각각 p=0.326, p=0.918), 두 군 간 차이도 유의하지 않았다(p=0.564,
Table 2, Fig. 1B). 치료 후 두 군 모두에서 중심황반두께의 감소가 의미 있게 나타났고(각각 p<0.001, p<0.001), 특히 덱사메타손삽입물군에서 더 크게 감소하였다(p<0.001, Table 2, Fig. 1C). 망막하를 제외한 내망막, 외망막 및 전체 고반 사점의 개수는 두 군 모두에서 치료 전에 비해 치료 후 유 의하게 감소하였으나(Fig. 2, 3), 두 군 간 차이를 보이지는 않았다(Table 2, Fig. 1D). 또한 베바시주맙주입술군과 덱사 메타손삽입물군의 치료 전후 안저 사진 소견상의 경성삼출 물 변화를 보면 베바시주맙주입술군에서는 큰 차이가 없는 경우가 많았던 반면, 덱사메타손삽입물군에서는 치료 후 현저하게 경성삼출물이 감소한 경우를 확인할 수 있었다 (Fig. 2, 3). 망막하액 유무, 외경계막과 타원체영역 손상은 치료 후 베바시주맙주입술군에서 통계적으로 유의하게 회 복되었으나(각각 p=0.023, p=0.032, p=0.031, Table 2, Fig. 4), 덱사메타손삽입물군에서는 외경계막 구조만 치료 후 유의
A B
C
D
Figure 2. A 27-year-old male presented with diabetic macular edema injected dexamethasone implant. (A) Fundus photography at
initial visit. Yellowish fibrinous materials are seen at the parafoveal area. The visual acuity is 20/200. (B) Fundus photography at eight weeks follow up. Yellowish fibrinous materials are much decreased. The visual acuity is 20/100. (C) Horizontal sectional im- age of optical coherence tomography (OCT) images at initial visit. The OCT shows sparse hyperreflective foci (arrows) distribution in the inner, outer and subretinal layers. Also subretinal fluid (SRF) is seen. (D) Horizontal sectional image of OCT images at eight weeks follow up. Hyperreflective foci are almost resolved and just small numbers (arrows) of hyperreflective foci remained. SRF is also nearly resolved.하게 변화하였다(p=0.031, Table 2, Fig. 4).
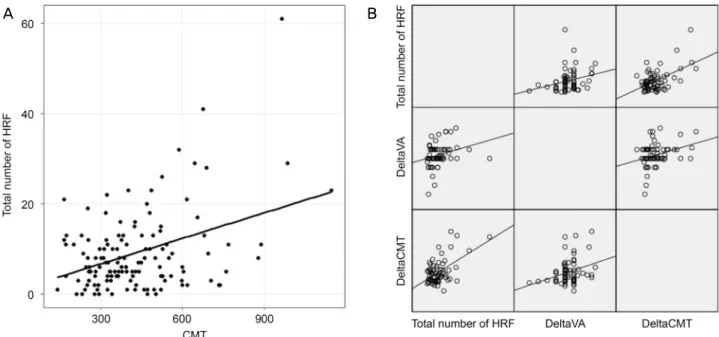
전체 대상군의 치료 전 중심황반두께와 고반사점의 개수 의 상관관계를 Spearman rank correlation 분석한 결과, 약 한 양의 상관관계(r=0.189)를 보였다(p=0.029, Fig. 5A). 전 체 대상군의 고반사점 개수와 치료 전후 시력 변화 정도, 치료 전후 중심황반두께의 상관관계 또한 둘 다 약한 양의 상관관계(각각 r=0.300, r=0.293)를 보였다(각각 p=0.014, p=0.017, Fig. 5B). 치료 전후 시력 변화와 중심황반두께 변화
도 약한 양의 상관관계(r=0.268)를 보였다(p=0.030, Fig. 5B).
고 찰
저자들은 본 연구를 통해 당뇨황반부종환자 중 유리체내 베바시주맙주입술과 덱사메타손삽입물을 시행한 두 군에 서 치료 전후를 비교한 결과, 시력의 경우 덱사메타손삽입 물군에서만 유의한 호전을 보였으며, 중심황반두께와 고반
A B
C
D
Figure 3. A 57-year-old male presented with diabetic macular edema injected bevacizumab. (A) Fundus photography at initial visit.
Retinal dot hemorrhages are seen at four quadrants. The visual acuity is 20/70. (B) Fundus photography at 4 weeks follow up.
Previously seen retinal dot hemorrhages are much decreased. The visual acuity is 20/40. (C) Horizontal sectional image of optical coherence tomography (OCT) images at initial visit. The OCT shows sparse hyperreflective foci (arrows) distribution in the all reti- nal layers. (D) Horizontal sectional image of OCT images at four weeks follow up. Numbers of hyperreflective foci are decreased.
사점 개수는 두 군 모두에서 의미 있는 감소를 보였음을 알 수 있었다. 특히, 중심황반두께는 덱사메타손삽입물군에서 유의하게 더 감소하였지만, 고반사점 개수 감소는 두 군 간 의미 있는 차이가 없었다.
고반사점이 손상된 혈관망막장벽을 통해 누출된 지단백 질이라는 가설을 뒷받침하는 기존의 연구 결과를 살펴보면, 당뇨황반부종환자에서 고반사점의 존재가 처음으로 보고 된 이후,6 외망막에 위치한 고반사점이 외경계막이나 시세
포외절과 같은 망막의 미세구조의 파괴와 연관이 있음이 밝혀졌고 이는 특히 시력 손상과 상관관계가 있었다.10 Ota et al12은 고반사점이 황반하 경성삼출물 축적과 관계가 깊 다고 하였으며, De Benedetto et al13은 당뇨황반부종이나 시력 손상이 없는 초기 당뇨망막병증 환자에서의 고반사점 을 보고하였고, 특히 고반사점이 당뇨의 유병 기간보다는 당 대사 상태에 따른 지질누출 정도와 관계가 깊었다는 점 을 강조하였다.
Figure 4. Comparison of changes in parameters of both groups after injection. Subretinal fluid, external limiting membrane, inner
segment–outer segment junction changes after dexamethasone implant and injection groups for follow up eight and four weeks. SRF= subretinal fluid; ELM = external limiting membrane; ISOS = inner segment/outer segment. *Categorical variables compared pre-treatment and post-treatment delta values of each parameter between bevacizumab group and dexamethasone group, using the Fisher’s exact test, and continuous variables with the independent t-test.
A B
Figure 5. Correlation of pretreatment total number of hyperreflective foci and other parameters. (A) Correlation of central macular
thickness and total number of hyperreflective foci before treatment in all patients of both groups. Central macular thickness and total number of hyperreflective foci showed weak positive correlation (p = 0.029, r = 0.189). (B) Change in visual acuity before and af- ter treatment and total number of hyperreflective foci showed weak positive correlation (p = 0.014, r = 0.300). Change in central macular thickness before and after treatment and total number of hyperreflective foci showed weak positive correlation (p = 0.017, r = 0.293). Change in visual acuity before and after treatment and change in central macular thickness before and after treatment foci showed weak positive correlation (p = 0.030, r = 0.268). All correlations were analyzed with Spearman rank correlation.CMT = central macular thickness; HRF = hyperreflective foci; Delta VA = Change in visual acuity before and after treatment;
Delta CMT = change in central macular thickness before and after treatment.
반면 당뇨황반부종의 발생기전에 염증 반응이 주요한 역 할을 담당하고,13-15 고반사점이 이러한 염증 매개 물질에 의 한 산물이라는 가설을 지지하는 연구 결과들도 있다. Vujosevic et al17은 당뇨망막병증이 진행함에 따라 활성화된 미세아 교세포가 내망막에서 외망막으로 이동하는 것과 마찬가지 로 고반사점 또한 같은 방향으로 이동함을 밝혔으며, Coscas et al9은 고반사점이 전 망막층에 두루 분포하고 치료 후 빠 르게 그 수가 감소한다는 점에서 경성삼출물과 차이를 보 인다고 주장하였다.
본 연구에서는 염증 반응을 감소시키기 위한 덱사메타손 삽입물 치료와 베바시주밥주입술 치료를 시행 후 두 약제 에 대한 고반사점의 변화를 비교하였다. 당뇨황반부종 환 자에서 트리암시놀론 이식은 경성삼출물을 줄이는 데 효과 적이라는 반면,18-20 유리체내 베바시주맙 주입은 황반부 삼 출물의 크기를 줄이는 데 효과가 없었다는 보고가 있다.20 본 연구에서도 유리체내 덱사메타손삽입물을 시행한 환자 에서는 경성삼출물이 크게 감소하였지만 유리체내 베바시 주맙주입술을 시행한 환자에서는 경성삼출물의 양의 변화 가 뚜렷하지 않음을 관찰할 수 있었다(Fig. 2, 3). 이러한 차 이를 보이는 것은 두 약제의 작용 기전의 차이에 의한 것으 로 생각된다.
혈관내피세포 성장인자는 염증성 사이토카인의 일종으 로 미세아교세포의 활성화를 유도한다고 알려졌고,21 혈관 내피세포 성장인자 억제제인 베바시주맙은 염증을 억제하 는 효과가 있다. 베바시주맙 주입 치료와 덱사메타손삽입 물 치료 후 모두에서 염증 반응을 억제함으로써 황반부종 의 감소에 영향을 미쳤다고 볼 수 있으며 동반된 고반사점 의 감소는 이런 염증 반응 감소의 신호라고 볼 수 있을 것 이다.
빛간섭단층촬영에서 고반사점과 경성삼출물을 구분하기 위해서 본 연구에서는 고반사점의 개수를 셀 때 40 μm를 초과하는 경우를 제외하였는데, 베바시주맙 주입 후 경성 삼출물에는 큰 변화 없었으나 고반사점이 줄었다는 점에서 고반사점을 경성삼출물의 전구물질이 되는 지단백질의 누 출이라고 보기는 어려울 것이다. 또 경성삼출물은 주로 망 막의 외망상층에 위치하는 반면 본 연구에서 치료 후 고반 사점이 망막 전층에서 유의하게 감소하였다는 점도 이를 뒷받침한다. 따라서 본 연구의 결과는 고반사점이 지단백 질의 누출이라는 가설보다는 염증매개물질 또는 활성화된 미세아교세포라는 가설을 뒷받침할 것으로 보인다.
Hatz et al22은 덱사메타손삽입물 시술 후 장기간 관찰에 서 유의한 고반사점 개수의 차이가 없었다고 하였는데 이 는 고반사점의 개수를 셀 때 크기에 제한을 두지 않아 경성 삼출물도 고반사점에 포함이 되었을 가능성이 있다고 볼
수 있다. 타 연구에서 외경계막, 타원체영역, 망막하액 등 망막 외층의 미세구조는 유리체내 혈관내피세포 성장인자 억제제주입술이나 덱사메타손삽입물 치료 후 회복되는 것 으로 알려져 있어21,23 본 연구와 비슷한 결과를 보였다.
본 연구 결과, 치료 전 전체 고반사점 개수가 많을수록 치료 후 시력호전 변화가 크고 중심황반두께 감소가 더 유 의하게 많이 관찰되었다. 고반사점 수가 많을수록 치료 후 반응이 좋은 것으로 보아 당뇨황반부종환자에서 치료 전 고반사점의 개수가 유리체내 베바시주맙 주입 또는 덱사메 타손삽입물 치료 반응을 예측하는 새로운 지표로 이용될 수 있을 것이라 기대된다. 다른 연구들에서도 치료 전 고반 사점 수가 많을수록 치료 후 반응이 좋았다는 결과를 보였 고, 치료 시작 전의 고반사점의 개수가 혈관내피세포 성장 인자 억제제 치료의 반응을 예측하는 새로운 표지자 역할 을 할 수 있을 것이라고 제기해왔다.24 하지만 장기적으로 는 고반사점의 개수가 많을수록 불량한 시력예후를 보인다 는 연구들도 있었다.25,26 치료 전 고반사점이 많을수록 염증 반응이 활성화된 상태로 보고 염증을 억제하는 베바시주맙 이나 덱사메타손 같은 치료에 단기적으로 반응하여 중심황 반두께 감소와 시력호전을 보일 것이라 추측할 수 있다. 하 지만 고반사점이 많다는 것은 염증 반응이 활발하여 최종 적으로는 안 좋은 시력예후를 보일 수 있다고 하여 장기 효 과에 대해서는 더 많은 연구가 필요할 것으로 생각된다.
이 연구의 제한점으로는 두 약제의 약효 지속 시간과 최 대 효과를 나타내는 시기가 각각 다를 것임을 고려하여 두 군 간의 경과 관찰시점을 다르게 하였다는 점, 적은 환자 수를 대상으로 후향적으로 4-8주의 짧은 기간을 경과 관찰 하였다는 점과, SD-OCT상에서 고반사점 개수를 셀 때 모 호한 정의로 인해 주관이 개입될 수 있었다는 점이 있다. 또한 술자가 당뇨황반부종에 대한 주사제를 선정 시 베바 시주맙주입술에 반응이 없었거나 혈관의 누출보다는 염증 반응에 의한 황밤부종이 심한 것으로 생각될 때 덱사메타 손을 고려하였다. 이러한 선택 편견에 의해 치료 전 중심황 반두께가 덱사메타손 그룹에서 더 두꺼웠던 제한점이 있다.
덱사메타손삽입물군에서 중심황반두께 감소 효과가 높았 고 이에 따라 치료 후 시력호전 정도도 높았던 것은 상기의 제한점에 의한 결과라고 추측된다.
정리하면 베바시주맙주입술군과 덱사메타손삽입물군 모 두에서 중심황반두께와 고반사점의 개수가 유의하게 감소 했고 시력은 덱사메타손삽입물군에서만 유의한 호전을 보 였다. 또한 치료 전 고반사점의 개수가 많을수록 치료 전 중심황반두께, 치료 전후 중심황반두께의 변화량, 치료 전 후 시력의 변화량이 크다는 양의 상관관계를 보였다. 고반 사점이 무엇인지에 대해서는 명확히 밝혀진 바는 없으나
염증 반응에 비례하게 증가한다고 생각되며 치료 전 고반 사점 개수가 많을수록 치료에 대한 반응이 좋다는 것을 알 수 있었다. 본 연구의 제한점을 보완하고 더 많은 표본을 대상으로 장기적인 연구를 통해 고반사점의 의의에 대한 연구가 필요할 것으로 생각된다.
REFERENCES
1) Moss SE, Klein R, Klein BE. The 14-year incidence of visual loss in a diabetic population. Ophthalmology 1998;105:998-1003.
2) Bhagat N, Grigorian RA, Tutela A, Zarbin MA. Diabetic macular edema: pathogenesis and treatment. Surv Ophthalmol 2009;54:1-32.
3) Mathews MK, Merges C, McLeod DS, Lutty GA. Vascular endo- thelial growth factor and vascular permeability changes in human diabetic retinopathy. Invest Ophthalmol Vis Sci 1997;38:2729-41.
4) van Hecke MV, Dekker JM, Nijpels G, et al. Inflammation and en- dothelial dysfunction are associated with retinopathy: the Hoorn Study. Diabetologia 2005;48:1300-6.
5) Chen TC, Cense B, Pierce MC, et al. Spectral domain optical co- herence tomography: ultra-high speed, ultra-high resolution oph- thalmic imaging. Arch Ophthalmol 2005;123:1715-20.
6) Bolz M, Schmidt-Erfurth U, Deak G, et al. Optical coherence to- mographic hyperreflective foci: a morphologic sign of lipid ex- travasation in diabetic macular edema. Ophthalmology 2009;116:
914-20.
7) Imesch M, Wolf-Schnurrbusch U, Framme C, Wolf S. Small dense particles in the retina observable by spectral-domain optical coher- ence tomography in central retinal vein occlusion. Invest Ophthalmol Vis Sci 2012;53:2671.
8) Ogino K, Murakami T, Tsujikawa A, et al. Characteristics of opti- cal coherence tomographic hyperreflective foci in retinal vein occlusion. Retina 2012;32:77-85.
9) Coscas G, De Benedetto U, Coscas F, et al. Hyperreflective dots: a new spectral-domain optical coherence tomography entity for fol- low-up and prognosis in exudative age-related macular degeneration.
Ophthalmologica 2013;229:32-7.
10) Uji A, Murakami T, Nishijima K, et al. Association between hyper- reflective foci in the outer retina, status of photoreceptor layer, and visual acuity in diabetic macular edema. Am J Ophthalmol 2012;
153:710-7.e1.
11) Framme C, Schweizer P, Imesch M, et al. Behavior of SD-OCT-de- tected hyperreflective foci in the retina of anti-VEGF-treated pa- tients with diabetic macular edema. Invest Ophthalmol Vis Sci 2012;53:5814-8.
12) Ota M, Nishijima K, Sakamoto A, et al. Optical coherence tomo- graphic evaluation of foveal hard exudates in patients with diabetic
maculopathy accompanying macular detachment. Ophthalmology 2010;117:1996-2002.
13) De Benedetto U, Sacconi R, Pierro L, et al. Optical coherence to- mographic hyperreflective foci in early stages of diabetic retinopathy.
Retina 2015;35:449-53.
14) Joussen AM, Poulaki V, Le ML, et al. A central role for in- flammation in the pathogenesis of diabetic retinopathy. FASEB J 2004;18:1450-2.
15) Kern TS. Contributions of inflammatory processes to the develop- ment of the early stages of diabetic retinopathy. Exp Diabetes Res 2007;2007:95103.
16) Tang J, Kern TS. Inflammation in diabetic retinopathy. Prog Retin Eye Res 2011;30:343-58.
17) Vujosevic S, Bini S, Midena G, et al. Hyperreflective intraretinal spots in diabetics without and with nonproliferative diabetic retin- opathy: an in vivo study using spectral domain OCT. J Diabetes Res 2013;2013:491835.
18) Avci R, Kaderli B. Intravitreal triamcinolone injection for chronic diabetic macular oedema with severe hard exudates. Graefes Arch Clin Exp Ophthalmol 2006;244:28-35.
19) Ciardella AP, Klancnik J, Schiff W, et al. Intravitreal triamcinolone for the treatment of refractory diabetic macular oedema with hard exudates: an optical coherence tomography study. Br J Ophthalmol 2004;88:1131-6.
20) Khairallah M, Zeghidi H, Ladjimi A, et al. Primary intravitreal tri- amcinolone acetonide for diabetic massive macular hard exudates.
Retina 2005;25:835-9.
21) Forstreuter F, Lucius R, Mentlein R. Vascular endothelial growth factor induces chemotaxis and proliferation of microglial cells. J Neuroimmunol 2002;132:93-8.
22) Hatz K, Ebneter A, Tuerksever C, et al. Repeated dexamethasone intravitreal implant for the treatment of diabetic macular oedema unresponsive to anti-VEGF therapy: outcome and predictive SD-OCT features. Ophthalmologica 2018;239:205-14.
23) Jeon S, Lee WK. Effect of intravitreal bevacizumab on diabetic macular edema with hard exudates. Clin Ophthalmol 2014;8:1479-86.
24) Schreur V, Altay L, van Asten F, et al. Hyperreflective foci on opti- cal coherence tomography associate with treatment outcome for anti-VEGF in patients with diabetic macular edema. PLoS One 2018;13:e0206482.
25) Chatziralli IP, Sergentanis TN, Sivaprasad S. Hyperreflective foci as an independent visual outcome predictor in macular edema due to retinal vascular diseases treated with intravitreal dexamethasone or ranibizumab. Retina 2016;36:2319-28.
27) Liu S, Wang D, Chen F, Zhang X. Hyperreflective foci in OCT im- age as a biomarker of poor prognosis in diabetic macular edema patients treating with Conbercept in China. BMC Ophthalmol 2019;19:157.
= 국문초록 =
당뇨황반부종에서 유리체 내 주사제에 따른 치료 전후 고반사점 변화 비교
목적: 당뇨황반부종환자의 빛간섭단층촬영에서 나타난 고반사점(hyperreflective foci)의 유리체내 덱사메타손삽입물과 유리체내 베바 시주맙주입술 후 변화를 비교하고자 하였다.
대상과 방법: 당뇨황반부종환자 66명, 66안을 대상으로 유리체내 덱사메타손삽입물군(35명, 35안), 유리체내 베바시주맙주입술군(31 명, 31안)으로 나누어 후향적 연구를 시행하였다. 빛간섭단층촬영에서 나타난 내망막, 외망막에 위치한 고반사점의 개수, 중심황반두 께, 외경계막 및 광수용체 내외측 경계부의 상태, 시력 등의 치료 전후의 변화를 약제에 따라 각각 약 4주 후와 8주 후에 조사하였다.
결과: 고반사점의 개수는 덱사메타손군의 경우 치료 전 10.6 ± 11.8개에서 치료 후 6.3 ± 5.9개로(p=0.005), 베바시주맙주입술군의 경우 치료 전 11.6 ± 8.5개에서 7.7 ± 6.7개로(p<0.001) 두 군 모두에서 유의하게 감소하였다. 덱사메타손삽입물군은 평균 중심황반두 께는 치료 전 586.8 μm에서 치료 후 297.7 μm로, 평균 시력은 치료 전 0.33 logMAR에서 치료 후 0.38 logMAR로 유의하게 호전되었 다(각각, p<0.001, p=0.018). 베바시주맙군은 평균 중심황반두께는 치료 전 467.1 μm에서 치료 후 353.2 μm로 유의하게 감소했으나 (p<0.001), 평균 시력은 치료 전 0.34 logMAR에서 치료 후 0.32 logMAR로 유의한 차이가 없었다(p=0.464).
결론: 유리체내 덱사메타손삽입물과 베바시주맙주입술 후 빛간섭단층촬영에서 나타난 고반사점은 유의하게 감소하였다.
<대한안과학회지 2020;61(1):41-50>
김민진 / Minjin Kim
순천향대학교 의과대학 순천향대학교 서울병원 안과학교실 Department of Ophthalmology, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine