INTRODUCTION
Rotator cuff tears are commonly accompanied by biceps tendon pathology. When conservative treatment for biceps pathology and rotator cuff tears fails, tenotomy or tenodesis combined with rotator cuff repair should be considered as a treatment option [1,2]. Biceps tenotomy is indicated for irreparable rotator cuff tears or advanced age patients unwilling to undergo rehabilitation after rotator cuff repair [3,4]. Patients who have full-thickness biceps tendon tears, severe biceps tendinopathy, biceps tendon subluxation, partial tendon tears affecting ≥ 50%
of the tendon diameter or irreparable superior labrum
anterior to posterior (SLAP) lesions are indicated for biceps tenodesis [5–8]. Open or arthroscopic biceps tenodesis has also been recommended for young, active patients, for aesthetic restoration, and for avoiding painful outcome [5–9].
Since Gilcreest [10] first described tenodesis of the long head of the biceps to the coracoid process, tenotomy and tenodesis have been the subject of debate. The efficacy of tenodesis has been demonstrated in many domestic studies; however, the use of tenotomy with tenodesis has not been sufficiently investigated.
In our research, we compared two groups of patients who underwent biceps tenodesis combined with rotator Background: The present study aims to evaluate the clinical outcomes of tenodesis followed by tenotomy and tenodesis without tenotomy for biceps long head tendon lesions during arthroscopic small- to medium-sized full-thickness rotator cuff repair.
Methods: This study was conducted on 33 patients who were available for at least 1-year regular follow-up after tenodesis of the long head of the biceps during arthroscopic small- to medium-sized full thickness rotator cuff repair between November 2009 and November 2010. Group I consisted of 20 patients who underwent tenodesis with tenotomy and group II consisted of 13 patients who underwent tenodesis without tenotomy. The outcomes were evaluated by visual analogue scale (VAS), UCLA scores, Speed’s test, and direct tenderness on the bicipital groove.
Results: At the last follow-up, the VAS decreased from a preoperative mean of 7.5 to a postoperative mean of 3.0 in group I and from a preoperative mean of 8.0 to a postoperative mean of 3.2 in group II (P < 0.05). The UCLA score increased from a preoperative mean of 15.7 to a postoperative mean of 32.3 in group I and from a preoperative mean of 13.8 to a postoperative mean of 29.4 in group II (P < 0.05). The number of positive Speed’s test decreased from 13 preoperatively to 5 postoperatively in group I and from 9 preoperatively to 2 postoperatively in group II (P < 0.05). The number of patients with direct tenderness on the bicipital groove decreased from 17 preoperatively to 3 postoperatively in group I and from 12 preoperatively to 4 postoperatively in group II (P < 0.05).
Conclusion: The use of tenotomy in combination with tenodesis for biceps long head tendon lesions had no significant impact on the clinical outcomes of arthroscopic rotator cuff repair.
Keywords: Shoulder joint; Biceps long head tendon; Arthroscopic tenodesis
Comparison of clinical outcomes of arthroscopic biceps long head tenodesis with or without tenotomy
Sang-Hun Ko, Kwang-Hwan Jung, Hang Ki Kang
Department of Orthopedic Surgery, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea
Copyright © 2015 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received May 28, 2014; Revised October 7, 2014; Accepted November 6, 2014
Correspondence to: Kwang-Hwan Jung, Department of Orthopedic Surgery, Ulsan University Hospital, University of Ulsan College of Medicine, 877 Bangeojinsunhwan-doro, Dong-gu, Ulsan 682-714, Korea. Tel: +82-52-250-7129, Fax: +82-52-235-2823, E-mail:
[email protected] Arthroscopy and
Orthopedic Sports Medicine
AOSM
cuff repair. Most tenodesis techniques require detachment of the tendon of the long head of the biceps from the supraglenoid tubercle. However, Wolfgang [11] proposed the use of the upper portion of the biceps tendon as a graft for additional blood supply to the hypovascular area in the rotator cuff during repair. Actually, labral branches of the suprascapular artery may supply blood to the long head of the biceps [12]. In addition, detachment of the biceps tendon may cause instability and dysfunction, resulting in significant upward migration of the humeral head and 5.1% reduction in the acromiohumeral space [13,14]. The purpose of our research was to determine the influence of tenotomy on the clinical results of tenodesis performed in
combination with arthroscopic rotator cuff repair based on comparison of the tenodesis with tenotomy group and tenodesis without tenotomy group.
METHODS
Inclusion and exclusion criteria
This study was conducted on patients who underwent biceps tenodesis during arthroscopic rotator cuff repair between November 2009 and November 2010. All the patients had biceps pathology refractory to conservative treatment such as pain medication, physical therapy, rest, and local injections. And all the patients had not a history
Table 1. Tenodesis with tenotomy (patient’s status)
Patients No. Sex Age (yr) Dominant arm Trauma Hx. Duration (mo) SS tear IS tear SBS tear Biceps tear 1
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
M M F M F M M M M M M M M F M M M M F F
72 72 74 52 63 62 52 55 50 53 61 54 56 57 61 47 41 58 60 52
N Y Y N Y Y Y Y Y Y Y Y Y Y Y Y Y Y N Y
Y Y Y Y Y Y Y Y Y N Y Y N Y Y Y Y Y Y Y
< 6
< 6
< 6 6–12
< 6 6–12
> 12
> 12
> 12
< 6
< 6
< 6 6–12
< 6 6–12 6–12 6–12 6–12
< 6
> 12
Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
Y N N Y Y N Y Y N Y N N Y Y N N N N N Y
Y Y N N Y Y N Y N Y Y Y Y Y Y Y N N Y N
Complete S/L Partial
S/L S/L Complete
S/L Complete Complete
S/L S/L Complete Complete
S/L S/L S/L S/L S/L S/L S/L The difference was statistically significant (P < 0.05).
Hx., history; SS, supraspinatus; IS, infraspinatus; SBS, subscapularis; M, male; F, female; Y, yes; N, no; S/L, subluxation.
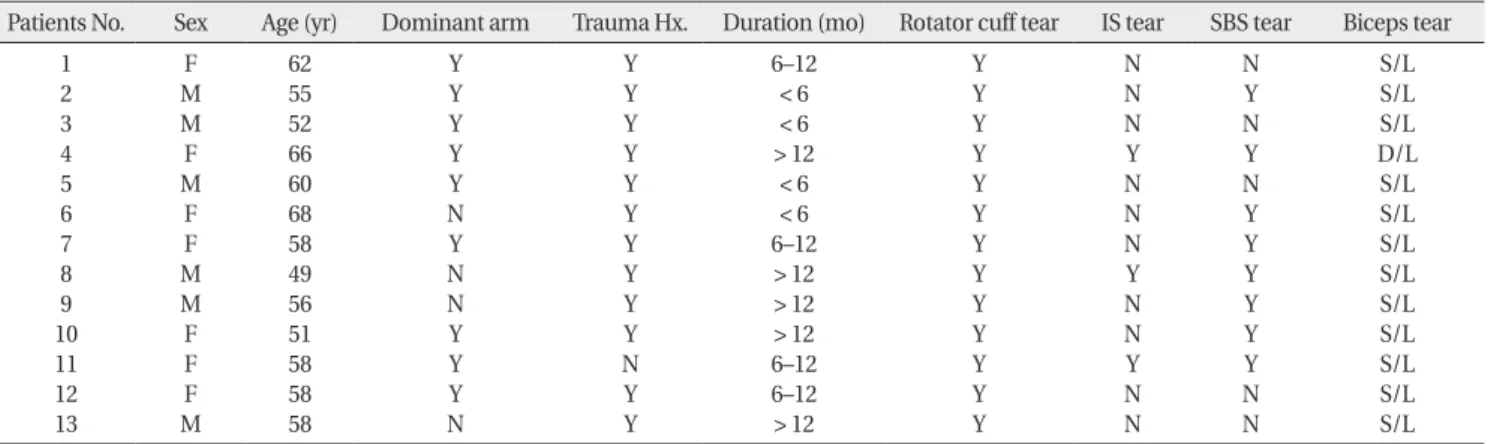
Table 2. Tenodesis without tenotomy (patient’s status)
Patients No. Sex Age (yr) Dominant arm Trauma Hx. Duration (mo) Rotator cuff tear IS tear SBS tear Biceps tear 1
2 3 4 5 6 7 8 9 10 11 12 13
F M M F M F F M M F F F M
62 55 52 66 60 68 58 49 56 51 58 58 58
Y Y Y Y Y N Y N N Y Y Y N
Y Y Y Y Y Y Y Y Y Y N Y Y
6–12
< 6
< 6
> 12
< 6
< 6 6–12
> 12
> 12
> 12 6–12 6–12
> 12
Y Y Y Y Y Y Y Y Y Y Y Y Y
N N N Y N N N Y N N Y N N
N Y N Y N Y Y Y Y Y Y N N
S/L S/L S/L D/L S/L S/L S/L S/L S/L S/L S/L S/L S/L The difference was statistically significant (P < 0.05).
Hx., history; IS, infraspinatus; SBS, subscapularis; M, male; F, female; Y, yes; N, no; S/L, subluxation; D/L, dislocation.
of surgery on the affected shoulder. Physical examination revealed, in addition to rotator cuff abnormality, bicipital groove pain or positive results on at least one of the three biceps tests (Speed’s test, Yergason’s test, direct tenderness on the biceps groove, and biceps instability test). Plain radiographs (anteroposterior view, neutral/external/
internal rotation views, lateral view of the scapula, and axillary view) and magnetic resonance imaging (MRI) scans were obtained for preoperative assessment: the MRI showed rupture, subluxation, or tendinitis of the long head of the biceps. Arthroscopic findings of severe tendinitis, partial or full-thickness biceps tears, or bicep instability were regarded as indications for tenodesis.
Patients with a ≥ 5 cm rotator cuff tear or a previous history of distal clavicle resection due to clavicle arthritis, labral repair, or arthroscopic shoulder surgery were excluded from the study.
Patients were assigned to either tenodesis with tenotomy group (group I) or tenodesis without tenotomy group (group II) by computerized randomization. Demographic characteristics of group I and group II are presented in Tables 1 and 2, respectively. In group I, there were 15 males and 5 females with a mean age of 57.6 years (range, 41–74 years). The lesion was located in the dominant arm in 17 patients. Thirteen patients had biceps tendon subluxation, 1 had a partial-thickness biceps tendon tear, and 6 had a full-thickness tear. In group II, there were 6 males and 7 females with a mean age of 57.8 years (range, 49–68 years). The lesion was in the dominant arm in 9 patients. Twelve patients had bicep tendon subluxation and 1 patient had biceps tendon dislocation.
Assessments
Preoperative assessments were performed the day before surgery and postoperative assessments were done at the final follow-up. The mean duration of follow-up was 16 months. All the patients were evaluated for arm do- minance, history of trauma, duration of symptoms, type of lesion, pre- and postoperative range of motion (ROM), visual analogue scale (VAS), UCLA score, Speed’s test, and direct tenderness on the bicipital groove. The level of activity was classified as sedentary, light, and strenuous.
Statistical analysis was done using SPSS Statistics for Windows version 17.0 (SPSS Inc., Chicago, IL, USA). The two-sample t-test and Mann-Whitney U-test were used to determine statistical significance within 95% confidence interval.
The VAS and UCLA score were used to assess the pre-
and postoperative shoulder pain, function, ROM, muscle strength, and patient satisfaction. The UCLA score was recorded as poor (0–20), fair (21–27), good (23–33), and excellent (34–35), and the VAS was graded on a scale of 0 (no pain) to 10 (unbearable pain). The presence of bicipital groove tenderness and Speed’s test results were denoted as positive (+) or negative (–).
Operative technique
The surgery was performed using 4 to 6 portals with the patient placed in the beach chair position under general anesthesia. A posterior portal was created 2 to 3 cm inferior and 1 cm medial to the posterolateral corner of the acromion. After making an approximately 2 to 3 mm skin incision, a blunt trocar was inserted with a rotating motion towards the coracoid process for visualization of the humeral head and the biceps tendon. Then, the trocar was advanced anteriorly through the joint capsule located within the triangular space formed by the biceps tendon, glenoid fossa, and the subscapularis and an anterior portal was established via an outside-in technique to visualize the glenoid fossa, glenohumeral ligament, and the subscapularis. For visualization of the subacromial space, with the sleeve slightly pulled outside the joint capsule, the trocar was advanced upward and rotated in a medial to lateral fashion to release adhesions in the bursa. If desired, using a spinal needle, a lateral portal was created 3 cm lateral to the lateral border of the acromion for visualization of the rotator cuff, acromion, and coracoacromial ligament. In all patients, rotator cuff tears and biceps tendon tears affecting ≥ 50% of the tendon diameter or dislocation were observed. Rotator cuff repair and coracoplasty were performed in all patients. After localizing the biceps groove, the long head of the biceps was exteriorized using a forceps. A suture lasso (Arthrex, Naples, FL, USA) was introduced from the superior portal and passed through the long head of the biceps. Then, a No. 1 polydioxanone suture (PDS; Ethicon, Somerville, NJ, USA) was passed and extracted using a grabber through the lateral portal. The withdrawn PDS limb was loaded into the shuttle relay system with a FiberWire or TigerWire (Arthrex) and passed through the long head of the biceps. After debriding the area proximal to the bicipital groove using a burr, fixation was performed using an interference screw and PushLock (Arthrex) or PopLock (Linvatec, Largo, FL, USA) (Fig. 1). In group I, following visualization of the biceps lesions (Fig. 2), tenotomy was performed additionally by releasing the attachments to
the supraglenoid tubercle and superior labrum.
Postoperative management
The protocol for postoperative care was the same in both groups. The operated arm was supported using an ab duction orthosis for 6 postoperative weeks. From the 1st postoperative day, passive forward flexion and external rotation were allowed as tolerated. Aggressive exercises were not allowed until 6 weeks after surgery to avoid damage to the repair. At 6 weeks after surgery, active exercises were initiated with the orthosis removed.
From the 10th to 12th postoperative week, isotonic strengthening exercises and rehabilitation of the rotator cuff, deltoid, and scapular stabilizers were started, which was continued for 6 months. Moderate or strenuous
activities were prohibited until the 1st postoperative year for restoration of the shoulder strength.
RESULTS
In group I (tenodesis with tenotomy), the postoperative UCLA scores were excellent in 8 patients and good in 3 patients. The mean VAS decreased from 7.5 (range, 6–9) preoperatively to 3.0 (range, 1–6) postoperatively, and the mean UCLA score increased from 15.7 (range, 9–21) preoperatively to 32.3 (range, 27–35) postoperatively, indicating statistically significant improvement (P <
0.05). The mean forward flexion was improved from 110o (range, 80o–130o) preoperatively to 164o (range, 135o–170o) at the last follow-up (P < 0.05). The mean range of external rotation was improved from 41o (range, 30o–45o) preoperatively to 55o (range, 20o–60o) at the last follow-up (P < 0.05). Internal rotation increased from a range of S1- T12 preoperatively to T12-T5 at the last follow-up (Table 3). In group II (tenodesis without tenotomy), the mean VAS decreased from 8.0 (range, 6–9) preoperatively to 3.2 (range, 1–6) postoperatively, and the mean UCLA score increased from 13.8 preoperatively to 29.4 postoperatively, indicating statistically significant improvement (P <
0.05). The mean forward flexion was improved from 96o (range, 10o–130o) preoperatively to 155o (range, 120o–170o) at the last follow-up (P < 0.05). The mean range of external rotation was improved from 36o (range, 15o–45o) preoperatively to 50o (range, 20o–60o) at the last follow- up (P < 0.05). Internal rotation increased from a range of S1-T12 preoperatively to T12-T5 at the last follow- up (Table 4). Regarding the intergroup comparison, the mean postoperative VAS was lower in group I than in group II (2.9 vs. 3.2), and the mean postoperative UCLA Fig. 1. Arthroscopic views from a lateral portal. (A) Tenotomized biceps long head tendon in the biceps groove area. (B) Biceps long head tenodesis using a knot less screw.
A B
Fig. 2. Arthroscopic view from a posterior portal showing a degenerative and complete tear of the biceps long head tendon.
score was higher in group I than in group II (32.3 vs.
29.4) (Tables 3, 4). The Speed’s test was positive in 13 patients preoperatively and in 5 patients postoperatively in group I and in 9 patients preoperatively and in 2 patients postoperatively in group II. Bicipital groove tenderness was present in 17 patients preoperatively and in 3 patients postoperatively in group I and in 12 patients
preoperatively and in 4 patients postoperatively in group II (Tables 3, 4). No statistically significant intergroup difference was noted with regard to the VAS, UCLA score, Speed’s test, and bicipital groove tenderness (P > 0.05).
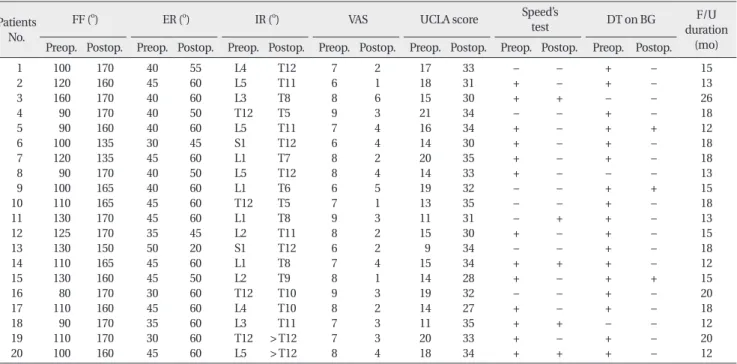
During the follow-up, there was no notable intergroup difference in gender, age, arm dominance, trauma history, and ROM that was improved in all directions (P Table 4. Tenodesis without tenotomy (range of motion, VAS, UCLA score, Speed’s test and DT on BG of pre- and postoperation)
Patients No.
FF (o) ER (o) IR (o) VAS UCLA score Speed’s
test DT on BG F/U
duration Preop. Postop. Preop. Postop. Preop. Postop. Preop. Postop. Preop. Postop. Preop. Postop. Preop. Postop. (mo)
1 2 3 4 5 6 7 8 9 10 11 12 13
120 90 10 90 130 100 110 120 90 120 100 90 80
170 160 160 120 170 170 170 160 120 160 160 150 150
45 45 30 30 15 45 30 45 30 45 20 45 45
60 60 45 45 20 60 45 50 45 60 35 60 60
L3 L5 S1 L5 T12 L4 L4 T12 L1 L5 L3 L5 L3
T12 T7 T11 T12 T5 T9 T8 T7 T6 T12 T11 T10 T9
8 8 9 8 7 7 8 6 9 9 9 9 7
2 3 3 5 6 2 3 1 5 4 3 2 2
14 13 8 15 17 18 17 22 11 11 9 14 11
33 34 31 19 28 29 30 35 18 34 23 34 35
+ + – + + + + – + – + – +
– – – – + – – – + – – – –
+ + + + + – + + + + + + +
– – – + + – + – + – – – –
12 12 12 19 13 16 25 19 24 26 24 12 16 The difference was statistically significant (P < 0.05).
VAS, visual analogue scale; DT, direct tenderness; BG, bicipital groove; FF, forward flexion; ER, external rotation; IR, internal rotation; F/U, follow-up;
Preop., preoperative; Postop., postoperative; L, lumbar spine vertebra; S, sacral spine vertebra; T, thoracic spine vertebra.
Table 3. Tenodesis with tenotomy (range of motion, VAS, UCLA score, Speed’s test and DT on BG of pre- and postoperation) Patients
No.
FF (o) ER (o) IR (o) VAS UCLA score Speed’s
test DT on BG F/U
duration Preop. Postop. Preop. Postop. Preop. Postop. Preop. Postop. Preop. Postop. Preop. Postop. Preop. Postop. (mo)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
100 120 160 90 90 100 120 90 100 110 130 125 130 110 130 80 110 90 110 100
170 160 170 170 160 135 135 170 165 165 170 170 150 165 160 170 160 170 170 160
40 45 40 40 40 30 45 40 40 45 45 35 50 45 45 30 45 35 30 45
55 60 60 50 60 45 60 50 60 60 60 45 20 60 50 60 60 60 60 60
L4 L5 L3 T12 L5 S1 L1 L5 L1 T12 L1 L2 S1 L1 L2 T12 L4 L3 T12 L5
T12 T11 T8 T5 T11 T12 T7 T12 T6 T5 T8 T11 T12 T8 T9 T10 T10 T11
> T12
> T12 7 6 8 9 7 6 8 8 6 7 9 8 6 7 8 9 8 7 7 8
2 1 6 3 4 4 2 4 5 1 3 2 2 4 1 3 2 3 3 4
17 18 15 21 16 14 20 14 19 13 11 15 9 15 14 19 14 11 20 18
33 31 30 34 34 30 35 33 32 35 31 30 34 34 28 32 27 35 33 34
– + + – + + + + – – – + – + + – + + + +
– – + – – – – – – – + – – + – – – + – +
+ + – + + + + – + + + + + + + + + – + +
– – – – + – – – + – – – – – + – – – – –
15 13 26 18 12 18 18 13 15 18 13 15 18 12 15 20 18 12 20 12 The difference was statistically significant (P < 0.05).
VAS, visual analogue scale; DT, direct tenderness; BG, bicipital groove; FF, forward flexion; ER, external rotation; IR, internal rotation; F/U, follow-up;
Preop., preoperative; Postop., postoperative; L, lumbar spine vertebra; S, sacral spine vertebra; T, thoracic spine vertebra.
> 0.05). None of the patients had postoperative infection, intraoperative neurological or vascular damage, bicipital pain, cosmetic deformity (Popeye sign), and limitations in daily living activities.
DISCUSSION
The influence of the biceps long head tendon on shoulder pain has been controversed. Traditionally, it has been con- sidered as a major source of shoulder pain. Thus, treat- ment of biceps tendon pathology has been regarded as a prerequisite for pain-free shoulder. Although increasing understanding of the rotator cuff has led to less primary surgery of the biceps tendon, the current focus has been redirected to the long head of the biceps tendon based on numerous research and clinical experience [1]. Rotator cuff tears are commonly accompanied by biceps tendon pathology. Actually, rotator cuff tears increase pressure and friction on the biceps tendon, eventually resulting in the formation of biceps lesions [2,15,16]. In other words, biceps tendinopathy are more prevalent in the shoulder with rotator cuff tears because of the increased load on the biceps tendon in the shoulder affected by biomechanical alterations [17].
Tenotomy or tenodesis are frequently used for the treat ment of biceps tendon lesions. Biceps tenodesis is in dicated for young, active patients presenting with ≤ 50% degeneration of the biceps tendon fibers, medial subluxation of the biceps, subcapularis tears, biceps subluxation, or irreparable SLAP lesions [18,19].
Biceps tenotomy is performed for irreparable rotator cuff tears or senior patients unwilling to participate in postoperative rehabilitation [5–8]. Biceps tenotomy can be a appropriate alternative to biceps tenodesis in patients who have refractory chronic bicipital pain [20].
This procedure may cause distal migration of the long head of the biceps tendon, cosmetic deformity such as Popeye sign, or significant reduction in muscle strength, but it is a rapid procedure that does not necessitate fixation [21]. Biceps tenodesis is advantageous over biceps tenotomy with repect to avoidance of cosmetic deformity and cramping pain, retainment of elbow supination, flexion strength and length-tension relationship, and prevention of muscle atrophy [22].
Various tenodesis techniques have been suggested by many authors. Boileau et al. [5] and Lo and Burkhart [7]
described an arthroscopic technique using bioabsorbable interference screws for fixation of the biceps tendon in the humeral socket, which doubled the strength of the tendon compared to the suture anchor technique.
Checchia et al. [2] first introduced an arthroscopic tenodesis technique that does not necessitate additional fixation procedure by including biceps tendon soft tissue in the rotator cuff suture. These biceps tenodesis techniques require separation of the biceps from the glenoid tubercle of scapla. On the other hand, Wolfgang [11] proposed the use of upper biceps tendon as a graft for blood supply to the hypovascular area during rotator cuff repair. Actually, labral branches of the suprascapular artery can provide blood supply to the long head of the biceps [12]. In addition, detachment of the long head of the biceps causes instability and dysfunction that result in significant upward migration of the humeral head and 5.1% reduction in the acromiohumeral space [13,14].
Although conservative treatment options should not necessarily be ruled out, we believe aggressive surgical approaches may be required for painful biceps pathology due to the risk of functional loss and secondary com- plications, and if performed under proper indications, teno tomy and tenodesis would be effective for pain relief. We designed this study to evaluate the efficacy of tenotomy, but there were some inherent limitations that should be addressed in future studies: 1) the study popu- lation was small; 2) the follow-up period was short; and 3) it was difficult to determine whether the symptomatic relief was attributable to the rotator cuff repair or to the tenodesis.
There was no significant difference with regard to the VAS, UCLA score, Speed’s test, and tenderness on the bicipital groove between the groups divided according to the use of tenotomy (P > 0.05). During the postoperative follow-up, no significant intergroup difference was noted in ROM that was improved in all measured directions.
Therefore, tenotomy did not appear to have significant influence on the treatment of biceps lesions identified during arthroscopic rotator cuff repair.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Burkhead WZ. The biceps tendon. In: Rockwood CA, Matsen FAI, editors. The shoulder. 4th ed. Philadelphia, PA: WB Saunders;
2008. p.791-836.
2. Checchia SL, Doneux PS, Miyazaki AN, et al. Biceps tenodesis associated with arthroscopic repair of rotator cuff tears. J Shoulder Elbow Surg 2005;14:138-44.
3. Barber FA, Byrd JW, Wolf EM, Burkhart SS. How would you treat the partially torn biceps tendon? Arthroscopy 2001;17:636-9.
4. Lo IKY, Burkhart SS. Arthroscopic biceps tenodesis: indications and technique. Oper Tech Sports Med 2002;10:105-12.
5. Boileau P, Krishnan SG, Coste JS, Walch G. Arthroscopic biceps tenodesis: a new technique using bioabsorbable interference screw fixation. Arthroscopy 2002;18:1002-12.
6. Gartsman GM, Hammerman SM. Arthroscopic biceps tenodesis:
operative technique. Arthroscopy 2000;16:550-2.
7. Lo IK, Burkhart SS. Arthroscopic biceps tenodesis using a bioabsorbable interference screw. Arthroscopy 2004;20:85-95.
8. Romeo AA, Mazzocca AD, Tauro JC. Arthroscopic biceps tenodesis. Arthroscopy 2004;20:206-13.
9. Richards DP, Burkhart SS. Arthroscopic-assisted biceps tenodesis for ruptures of the long head of biceps brachii: the cobra procedure. Arthroscopy 2004;20 Suppl 2:201-7.
10. Gilcreest E. Two cases of spontaneous rupture of the long head of the biceps flexor cubiti. Surg Clin North Am 1926;6:539-54.
11. Wolfgang GL. Surgical repair of tears of the rotator cuff of the shoulder. Factors influencing the result. J Bone Joint Surg Am 1974;56:14-26.
12. Rathbun JB, Macnab I. The microvascular pattern of the rotator cuff. J Bone Joint Surg Br 1970;52:540-53.
13. Kumar VP, Satku K, Balasubramaniam P. The role of the long
head of biceps brachii in the stabilization of the head of the humerus. Clin Orthop Relat Res 1989;(244):172-5.
14. Warner JJ, McMahon PJ. The role of the long head of the biceps brachii in superior stability of the glenohumeral joint. J Bone Joint Surg Am 1995;77:366-72.
15. Gill TJ, McIrvin E, Mair SD, Hawkins RJ. Results of biceps tenotomy for treatment of pathology of the long head of the biceps brachii. J Shoulder Elbow Surg 2001;10:247-9.
16. Mazzocca AD, Rios CG, Romeo AA, Arciero RA. Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy 2005;21:896.
17. Carpenter JE, Wening JD, Mell AG, Langenderfer JE, Kuhn JE, Hughes RE. Changes in the long head of the biceps tendon in rotator cuff tear shoulders. Clin Biomech (Bristol, Avon) 2005;20:162-5.
18. Murthi AM, Vosburgh CL, Neviaser TJ. The incidence of pathologic changes of the long head of the biceps tendon. J Shoulder Elbow Surg 2000;9:382-5.
19. Ozalay M, Akpinar S, Karaeminogullari O, et al. Mechanical strength of four different biceps tenodesis techniques.
Arthroscopy 2005;21:992-8.
20. Osbahr DC, Diamond AB, Speer KP. The cosmetic appearance of the biceps muscle after long-head tenotomy versus tenodesis.
Arthroscopy 2002;18:483-7.
21. Wolf RS, Zheng N, Weichel D. Long head biceps tenotomy versus tenodesis: a cadaveric biomechanical analysis. Arthroscopy 2005;21:182-5.
22. Mazzocca AD, Cote MP, Arciero CL, Romeo AA, Arciero RA. Clinical outcome after subpectoral biceps tenodesis with an interference screw. Am J Sports Med 2008;36:1922-9.