10 mm 이하의 작은 폐결절에 대한 CT 유도 폐침생검술 결과 : 결절 유형과의 관계
국민건강보험 일산병원 영상의학과
홍용국
CT Guided Percutaneous Needle Biopsy of Small (≦10 mm) Pulmonary Nodules : Correlation with CT Attenuation Types
Yong Kook Hong
Department of Radiology, National Health Insurance Service Ilsan Hospital, Goyang, Korea
Background: Improving CT technology and image quality, small pulmonary nodules are detected more frequently. The need for pat- hologic diagnosis of small pulmonary nodules is increasing for early detection of small lung cancers. CT guided percutaneous needle biopsy is a relatively safe and noninvasive procedure to obtain the pathologic diagnosis. We performed this study to eval- uate the usefulness of CT guided percutaneous needle biopsy of small pulmonary nodules smaller than 10 mm.
Methods: Smaller than 10 mm sized sixty-one pulmonary nodules performed CT guided percutaneous needle biopsy were reviewed retrospectively. We evaluated diagnostic accuracy, complication, pathologic diagnosis, according to nodular patterns of CT densities.
Results: In 56 of 61 nodules, useful pathologic diagnoses were obtained. Twenty-eight of 56 nodules were malignant. All of 14 subsolid nodules obtained pathologic diagnosis were malignant. Two of 9 ground glass nodules and 3 of 45 solid nodules were non-diagnostic. Closed-tube thoracostomy were needed in 4 of 61 patients after procedures because of pneumothorax.
Conclusion: CT guided percutaneous needle biopsy is a useful procedure for pathologic diagnosis of small pulmonary nodules, even smaller than 10 mm, with relatively high accuracy and low complication rate. Subsolid nodules showed high probability of lung cancer, but less accuracy to obtain pathologic diagnosis.
Key Words: Pulmonary nodule, Percutaneous needle biopsy
책임저자 : 홍용국
10444 경기도 고양시 일산동구 일산로 100 국민건강보험 일산병원 영상의학과 전화 : (031)900-0863, 팩스 : (031)900-0856 E-mail : [email protected]
*본 연구는 국민건강보험 일산병원의 연구비 지원으로 이루어 졌음 (NHIMC 2017CR029).
서 론
CT의 기술 발달로 작은 결절이나 밀도가 높지 않은 간유리 결절들의 발견이 증가하고 있다. 발견된 작은 폐 결절은 크기, CT 밀도, 위험인자에 따라 향후 계획이 결정된다.1 10 mm 이하의 결절은 주로 추적 검사를 하게 되며, 결절의 크기, CT 밀도, 위험인자에 따라 추적 검사의 기간과 간격이 정해지게 된다. CT유도 경피적 폐 침생검은 결절의 크기가 작은 경우
진단율이 떨어질 수 있으나 비교적 간편하며, 합병증이 적어 10 mm 이하의 작은 결절에 대해서도 8 mm 이상의 고형결절 이거나, 추적 CT에서 크기가 커지거나, 고형부위가 증가하는 비고형성 결절에 대해 가장 먼저 시행할 수 있는 조직 검사다.
이 연구에서는 CT 유도 폐 침생검을 시행한 경우 중 10 mm 이하의 작은 결절의 생검을 후향적으로 검토하여 진단율, 합 병증 등을 조사하고, 결절의 CT밀도에 따른 유형별로 병리 결과, 진단율 등의 차이를 분석하였다.
대상 및 방법
1. 대상
2013년 1월부터 2016년 12월까지 4년간에 걸쳐 CT유도 하 경피적 생검을 시행한 671명 중 결절의 크기가 10 mm 이하
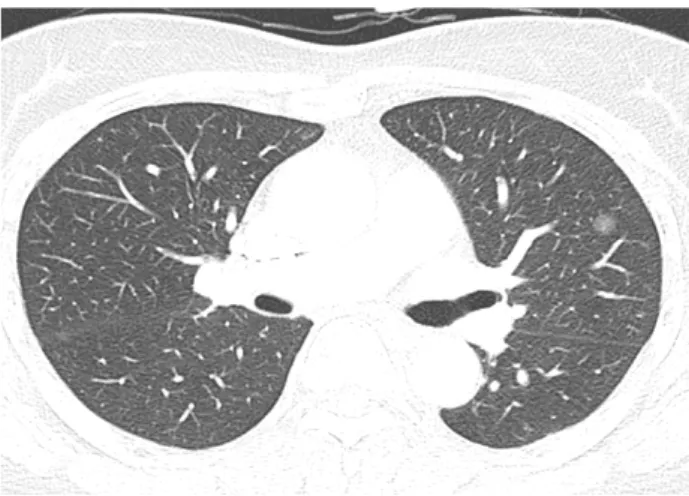
Fig. 1. Axial CT image of a ground glass nodule. CT image shows a 10 mm sized ground glass nodule in anterior segment of left upper lobe. CT guided percutaneous needle biopsy was perfor- med. The pathologic diagnosis was adenocarcinoma.
인 61명을 대상으로 후향적으로 분석하였다. 국민건강보험 일산병원 연구윤리심의위원회의 승인을 얻었다. 67명 중 여 자가 35명 남자가 26명이었다. 나이는 39세에서 85세였으면 평균 67.6세였다.
2. 방법
CT는 Somatom sensation 64 또는 Somatom definition flash (Siemens medical Solutions, Forchheim, Germany) scanner를 이용하여 촬영하였으며, 촬영 조건은 detector collimation 0.75 mm, image increment 1.0 mm, pitch 1.0, tube voltage 120
KVp, tube current 60 mA, matrix 512×512였고, reconstru- ction은 medium sharp algorithm을 이용하여 2 mm 두께로 axial 영상을 얻었고, window level –700, width 1350으로 영 상을 분석하였다.
결절의 CT 음영에 따라 간유리음영결절, 부분고형결절, 고형 결절로 나누었다. 간유리 음영결절은 결절음영 내부에 폐혈관이 보이는 경우, 고형결절은 결절의 음영이 높아 내부 의 폐 구조가 보이지 않는 경우, 부분고형결절은 간유리음영 과 고형결절이 함께 있는 경우로 하였다. 간유리 음영 결절과 부분고형 결절을 합하여 아고형결절로 분류하였다. 결절의 크기, 위치, 모양 등도 분석하였다.
3. CT 유도 경피적 생검
조직 검사는 먼저 이전에 시행한 CT을 참조하여 적절한 체위를 결정하고, 이 체위에서 CT 영상을 얻어 적합한 피부 부위에 표식을 하고 국소마취 후 CT 유도하에 18 gauge dis- posable core biopsy needle을 생검총에 장착하여 폐 결절 부위 까지 바늘을 진입 시킨 후 생검총을 발사하여 조직을 얻었다.
육안적으로 충분한 양의 조직이 나올 경우 시술을 끝냈으며, 조직이 충분치 않다고 생각될 경우 1-2회 더 시행하였다. 조 직 검사 직후 그리고 다음날 단순흉부촬영을 시행하였다.
4. 결과 분석
생검을 시행한 조직의 병리 검사 결과를 분석하였다. 시술 직후와 다음날 시행한 흉부단순촬영을 통해 합병증 유무를 분석하였다. 결절의 유형별 병리 결과을 분석하였고, 성공률 과 합병증 발생 빈도를 분석하였다.
결 과
결절의 크기는 5 mm에서 10 mm 사이였으며, 평균 9.0
(±1.4)이었다. 이중 8 mm 미만은 9개이었고, 나머지 52개는 8 mm 이상, 10 mm 이하였다.
결절의 위치는 좌상엽의 첨후분엽에 8개, 좌상엽의 전분엽 에 6개, 좌하엽의 상분엽에 7개, 좌하엽의 전내기저분엽에 3개, 좌하엽의 외기저분엽에 2개, 좌하엽의 후기저분엽에 5 개, 우상엽 첨분엽에 7개, 우상엽 후분엽에 4개, 우상엽 전분 엽에 1개, 우중엽 외분엽에 7개, 우중엽 내분엽에 1개, 우하엽 상분엽에 4개, 우하엽 전기저분엽에 2개 우하엽 외기저분엽 에 1개, 우하엽 후기저분엽에 3개 등으로 비교적 고르게 분포 하였다.
결절의 CT 밀도에 의한 유형은 고형 결절이 45개로 가장 많았고, 간유리음영 결절이 9개, 부분고형 결절이 7개였다.
61개의 결절 중 56개(92%)에서는 병리적 결과를 얻을 수 있 었으며, 5개(8%)에서는 병리적으로 유용한 결과를 얻기 못했 다. 병리적으로 결과를 얻은 56개의 결절 중 악성결절은 28개 이었으며, 이 중 원발성 폐암이 24개, 전이성 폐암이 4개이었 다. 24개의 원발성 폐암 중 폐선암이 18개으로 가장 많았고, 소세포암이 1개, 편평상피암이 1개, 상피내선암이 3개, 유상 피 혈관 내피종이 1개였다. 비염증성 양성 결절은 6개이었고 이 중 비정형샘종이 1개, 양성종양인 과오종이 5개이었다.
22개의 염증성 결절 중 7개의 결절은 결핵이었으며, 7개의 결절은 기질화 폐염이었고, 나머지 8개의 결절은은 섬유화 또는 급성 또는 만성 염증성 병변이었다.
간유리음영 결절 9개 중 5개는 폐선암, 2개는 상피내선암 이었으며, 2개의 결절에서는 유용한 병리결과를 얻지 못했다 (Fig. 1). 부분고형결절 7개 모두는 선암이었다(Fig. 2). 고형결
Table 1. Pathologic diagnosis according to nodular patterns Pattern of nodule
(number of nodules) Pathology (number of nodules) Ground glass (9) adenocarcinoma (5)
adenocarcinoma in situ (2) non-diagnostic (2)
Part-solid (7) adenocarcinoma (7) Solid (45) adenocarcinoma (6)
small cell carcinoma (1) squamous cell carcinoma (1) epithelioid hemangioendothelioma (1) adenocarcinoma in situ (1)
atypical adenomatous hyperplasia (1) metastasis (4)
hamartoma (5) tuberculosis (7)
organizing pneumonia (7) fibrosis (4)
acute/chronic inflammation (4) non-diagnostic (3)
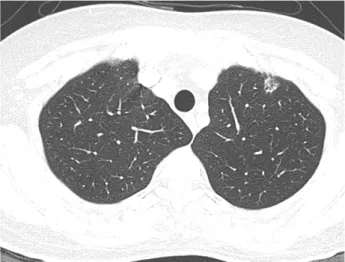
Fig. 2. Axial CT image of a part-solid nodule. CT image demonst- rates a 10 mm sized subsolid nodule in apicoposterior segment of left upper lobe. CT guided percutaneous biopsy was perfor- med. The pathologic diagnosis was adenocarcinoma.
Fig. 3. CT guided biopsy of the solid nodule. An 8 mm sized solid nodule was demonstrated in the anterior segment of left upper lobe. The biopsy needle was inserted into the nodule under CT guidance. The pathologic diagnosis is adenocarcinoma.
절 45개 중 42개에서 유용한 병리 결과를 얻을 수 있었고, 3개의 결절에서 유용한 병리결과를 얻지 못했다(Fig. 3). 고형 결절의 병리 결과로는 원발성 폐암이 10개, 전이성 암이 4개, 비정형샘종이 1개, 과오종이 5개, 결핵이 7, 기질화 폐렴이 7개, 섬유화나 급성 또는 만성 염증이 8개였다. 생검 결과 비정 형샘종증식증이었던 고형결절 1개과 상피내선암이었던 간유 리음영 1개는 수술 후 폐 선암으로 확진 되었다(Table 1).
61명의 환자 중 16명(17,6%)에서 시술 직후 시행한 CT에 서 기흉이 발견되었다. 12명은 소량의 기흉으로 수 일 이내에
특별한 처치 없이 흡수되었으며, 4명(5,5%)에서 흉관 삽관을 시행하였다.
고 찰
폐 결절은 CT 밀도에 따라 고형, 부분 고형, 간유리음영으 로 나눌 수 있다.1-3 간유리 음영 결절과 부분 고형 결절을 합하 여 아고형 결절로 분류한다. 고형결절은 CT 밀도가 높아 결절 내부의 폐혈관음영이 소실된 경우이고, 간유리 음영은 폐 결절 의 CT 밀도가 높지 않아 결절 내부의 폐혈관음영이 보이는 경우다. 부분고형은 간유리 음영과 고형음영이 함께 있는 결절 을 말한다. CT 밀도에 의한 결절의 유형에 따라 결절의 병리학 적 진단의 유형이 다르고, 결절의 폐암 가능성이 다르다.2-7 CT의 기술 발달로 작은 결절이나 밀도가 높지 않은 간유리 결절들의 발견이 증가하고 있다. 발견된 작은 폐의 결절은 크기, CT 밀도, 위험인자에 따라 향후 계획이 결정된다.1 Fleis- chner Society의 2017년 가이드라인에 따르면 고형 결절의 경우, 크기가 6 mm 이하고 위험인자가 없는 경우는 추적 CT 가 필요하지 않으며, 위험인자가 있는 경우는 12개월 후 추적 CT를 시행하는 것을 권장한다.1 고형결절이 6 mm 이상, 8 mm 이하인 경우는 6-12개월 후, 18-24개월 추적 CT를 권장 한다.1 8 mm 이상인 경우는 3개월 추적 CT, PET-CT, 또는 생검을 권장한다.1 부분고형 결절은 6 mm 이상에서 3-6개월 추적 CT후 변화가 없으면 1년 간격으로 5년간 추적 CT를
시행할 것을 권하고 있으며, 간유리 결절은 6 mm 이상인 경 우 1년 후 추적 CT를 시행 후 변화가 없으면 2년 간격으로 5년 추격 관찰하는 것을 권장하고 있다.1 크기가 증가하거나, 고형부분이 증가하는 아고형성 결절, 또는 고형부분이 8 mm 이상인 지속되는 부분 고형 결절은 PET-CT, 생검, 또는 절제 술이 권장된다.1
IASCL 8th edition 폐암 병기에 따르면 결절의 최대 직경이 2 cm 이하이고, 폐나 내측 흉막에 둘려 싸여있으면 T1a, 2 cm 초과 3 cm 이하인 경우는 T1b 병기였으나, 2016년 제안된 8차 개정에 의하면 결절의 직경이 1 cm 이하는 T1a, 1 cm 초과 2 cm 이하인 경우는 T1b, 2 cm 초과 3 cm 이하인 경우는 T1c로 정하고 있다.8 이는 2 cm 이하의 작은 결절에서도 크기 가 예후에 영향을 미치기 때문이다. 따라서 1 cm 이하의 작은 결절의 폐암 여부를 결정하는 것이 중요하다.
CT 유도하의 경피적 침 생검은 수술적 생검에 비해 시술이 간단하며, 합병증이 적으면서도 진단율이 비교적 높아(88- 100%) 폐 결절의 조직검사에 유용한 방법이지만, 크기가 작 은 경우 결절에 대한 접근성이 낮고 조직 진단율이 낮아 15 mm에서 74-95% 정도로 알려져 있다.9-12 1 cm 이하의 작은 결절, 특히 간유리 결절의 경우는 흉강경 또는 개흉술에 의한 조직 검사도 어려워 먼저 CT 유도하에 경피적으로 위치 표시 를 시행한 후 수술적 생검을 시행하기도 한다.13-21
본 연구에서는 10 mm 이하의 작은 결절에서도 61명 중 56명, 약 92%의 비교적 높은 경우에서 유용한 병리 결과를 얻을 수 있었다. 병리적 결과를 얻지 못한 5명 중 간유리음영 결절이 2명(22%), 고형 결절이 3예(7%)였다. 간유리음영의 작은 결절일 경우 고형결절이나, 부분고형결절에 비해 경피 적 폐 침생검으로 유용한 병리적 결과를 얻지 못할 가능성이 높은 것으로 보인다.
경피적 폐 침생검을 시행한 61명 중 중대한 시술 합병증을 보인 환자는 없었으며, 4명, 5.5%에서 흉관 삽입이 필요한 기 흉이 발생하였다. 크기가 작은 결절이 크기가 큰 결절에 비해 합병증의 빈도를 의미 있게 높이지는 않는 것으로 보인다.
간유리음영 결절 9예 중 유용한 병리 결과를 얻은 7예 모두 는 선암이거나 상피내선 암이었으며, 부분고형 7예 모두는 선암이었다. 고형결절 45예 중 원발성 폐암은 10예, 전이성 폐암은 4예로 31%에서 악성 종양이었다. 간유리 음영이나 부분 고형 등의 아고형성 병변은 비록 크기가 1 cm 이하의 작은 결절이라도 악성 종양의 가능성이 매우 높은 것을 확인 할 수 있었다.
경피적 폐 침생검에서 비정형샘종의 병리 결과를 얻은 1예
와 상피내선암의 결과를 얻은 1예는 수술에서 선암으로 확진 되었다. 크기가 작은 선암의 경우 결절내 병리의 불균일성에 의해 부분적으로 작은 검체를 얻는 폐 침생검에서 상피내선 암이나 비정형샘종으로 오진될 수 있는 것으로 보이며, 이러 한 병리 결과를 얻을 경우 수술적 절제를 고려해야 할 것으로 생각된다.
본 연구의 한계점으로는 첫째 경피적 침생검으로 기질화 폐렴이나 섬유화, 비정형샘종 등 양성질환의 병리를 얻은 환 자들에서 수술이나 충분한 기간의 추적 검사가 이루어지지 않은 경우가 있어 악성 종양의 위음성을 완전히 배제 하지 못했다, 둘째, 고형 결절에 비해 간유리음영 결절이나 부분고 형 결절의 아고형 결절의 수가 적어 유형에 따른 진단율의 정확한 통계적 의의를 구할 수 없었다. 셋째, 10 mm 이하의 모든 결절 중 악성이 의심 되는 경우에 생검을 시행함으로써 전체 병리 중 악성의 비율이 높아진 걸로 생각된다.
결론적으로 10 mm 이하의 작은 결절에서도 CT 유도 폐 침생검으로 92% 정도의 비교적 높은 비율로 유용한 병리결 과를 얻을 수 있고, 크기가 큰 결절에 비해 합병증의 빈도가 높지 않고 비침습적 시술이므로 크기가 커지거나, 부분 고형 결절 등 악성 종양이 의심되는 경우 적극적으로 폐 침생검을 고려할 경우 폐암의 조기 진단율을 올릴 수 있을 것이다.
REFERENCES
1. MacMahon H, Naidich DP, Goo JM, Lee KS, Leung ANC, Mayo JR, et al. Guidelines for Management of Incidental Pul- monary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology 2017;284(1):228-43.
2. Kim H, Park CM, Koh JM, Lee SM, Goo JM. Pulmonary subsolid nodules: what radiologists need to know about the imaging features and management strategy. Diagn Interv Radiol 2014;20(1):47-57.
3. Godoy MC, Naidich DP. Overview and strategic management of subsolid pulmonary nodules. J Thorac Imaging 2012;27(4):
240-8.
4. Kakinuma R, Noguchi M, Ashizawa K, Kuriyama K, Maeshima AM, Koizumi N, et al. Natural History of Pulmonary Subsolid Nodules: A Prospective Multicenter Study. J Thorac Oncol 2016;
11(7):1012-28.
5. Kobayashi Y, Sakao Y, Deshpande GA, Fukui T, Mizuno T, Kuroda H, et al. The association between baseline clinical- radiological characteristics and growth of pulmonary nodules with ground-glass opacity. Lung Cancer 2014;83(1):61-6.
6. Lee JH, Park CM, Lee SM, Kim H, McAdams HP, Goo JM.
Persistent pulmonary subsolid nodules with solid portions of 5 mm or smaller: Their natural course and predictors of inter- val growth. Eur Radiol 2016;26(6):1529-37.
7. Lee SM, Park CM, Goo JM, Lee HJ, Wi JY, Kang CH. Invasive pulmonary adenocarcinomas versus preinvasive lesions appea- ring as ground-glass nodules: differentiation by using CT featu- res. Radiology 2013;268(1):265-73.
8. Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, et al. The IASLC Lung Cancer Staging Pro- ject: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 2016;11(1):39-51.
9. Laurent F, Latrabe V, Vergier B, Montaudon M, Vernejoux JM, Dubrez J. CT-guided transthoracic needle biopsy of pul- monary nodules smaller than 20 mm: results with an automated 20-gauge coaxial cutting needle. Clin Radiol 2000;55(4):281-7.
10. Ng YL, Patsios D, Roberts H, Walsham A, Paul NS, Chung T, et al. CT-guided percutaneous fine-needle aspiration biopsy of pulmonary nodules measuring 10 mm or less. Clin Radiol 2008;
63(3):272-7.
11. Tsukada H, Satou T, Iwashima A, Souma T. Diagnostic accu- racy of CT-guided automated needle biopsy of lung nodules.
AJR Am J Roentgenol 2000;175(1):239-43.
12. Klein JS. Transthoracic needle aspiration biopsy for the cytolo- gic diagnosis of subsolid lung nodules. Cancer Cytopathol 2016;
124(7):451-2.
13. Findik G, Demiroz SM, Apaydin SMK, Erturk H, Biri S, Ince- kara F, et al. Computed Tomography-Guided Methylene Blue Labeling Prior to Thoracoscopic Resection of Small Deeply Placed Pulmonary Nodules. Do We Really Need Palpation?
Thorac Cardiovasc Surg 2017;65(5):387-91.
14. Hanauer M, Perentes JY, Krueger T, Ris HB, Bize P, Schmidt S, et al. Pre-operative localization of solitary pulmonary nodules
with computed tomography-guided hook wire: report of 181 patients. J Cardiothorac Surg 2016;11:5,016-0404-4.
15. Kim KS, Beck KS, Lee KY, Moon SW. CT localization for a patient with a ground-glass opacity pulmonary nodule expe- cting thoracoscopy: a mixture of lipiodol and India ink. J Tho- rac Dis 2017;9(4):E349-53.
16. Kleedehn M, Kim DH, Lee FT, Lubner MG, Robbins JB, Ziemlewicz TJ, et al. Preoperative Pulmonary Nodule Locali- zation: A Comparison of Methylene Blue and Hookwire Techni- ques. AJR Am J Roentgenol 2016;207(6):1334-9.
17. Klinkenberg TJ, Dinjens L, Wolf RFE, van der Wekken AJ, van de Wauwer C, de Bock GH, et al. CT-guided percutaneous hookwire localization increases the efficacy and safety of VATS for pulmonary nodules. J Surg Oncol 2017;115(7):898-904.
18. Lin MW, Chen JS. Image-guided techniques for localizing pul- monary nodules in thoracoscopic surgery. J Thorac Dis 2016;
8(Suppl 9):S749-55.
19. Qi H, Wan C, Zhang L, Wang J, Song Z, Zhang R, et al. Early effective treatment of small pulmonary nodules with video- assisted thoracoscopic surgery combined with CT-guided dual- barbed hookwire localization. Oncotarget 2017;8(24):38793- 801.
20. Sui X, Zhao H, Yang F, Li JL, Wang J. Computed tomography guided microcoil localization for pulmonary small nodules and ground-glass opacity prior to thoracoscopic resection. J Thorac Dis 2015;7(9):1580-7.
21. Wang T, Ma S, Yan T, Song J, Wang K, He W, et al. Compu- ted Tomography Guided Hook-wire Precise Localization and Minimally Invasive Resection of Pulmonary Nodules. Zhon- gguo Fei Ai Za Zhi 2015;18(11):680-5.