Tuberc Respir Dis 2011;71:322-327
CopyrightⒸ2011. The Korean Academy of Tuberculosis and Respiratory Diseases. All rights reserved.
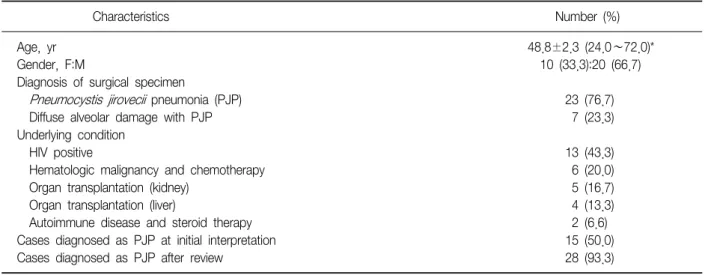
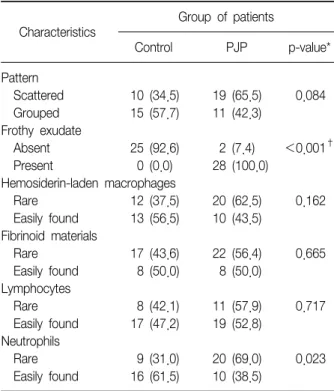
Value of Bronchoalveolar Lavage Fluid Cytology in the Diagnosis of Pneumocystis jirovecii Pneumonia: A Review of 30 Cases
Ji-Youn Sung, M.D.
1, Joungho Han, M.D.
1, Young Lyun Oh, M.D.
1, Gee Young Suh, M.D.
2, Kyeongman Jeon, M.D.
2, Taeeun Kim, M.D.
31