Relationship Between Bone Mineral Density and
Risk Factors of Atherosclerosis and Cardiovascular Disease in Korean Postmenopausal Women
Eun Hee Kong, Ji Young Lee2, Woong Hwan Choi3, Young Lim Oh1, Heung Yeol Kim1 Department of Family Medicine, Department of Obstetrics & Gynecology1, College of Medicine, Kosin University, Busan,
Department of Obstetrics and Gynecology2, Konkuk University, Seoul,
Department of Internal Medicine3, Hanyang University, College of Medicine, Seoul, Korea
Objectives: We investigated the associations between bone mineral density (BMD) and the risk factors for atherosclerosis and cardiovascular disease (CVD) in Korean postmenopausal women who were enrolled in a health promotion center of a university hospital from January, 2007 to December, 2009.
Methods: The risk factors of atherosclerosis and CVD were a current smoker, no regular exercise, obesity, abdominal obesity, hypercholesterolemia, low levels of high density lipoprotein cholesterol, high levels of low density lipoprotein cholesterol, hypertriglyceridemia, hypertension, and diabetes mellitus. Metabolic syndrome was used as an endpoint of the risk factors for atherosclerosis and CVD. The BMD measures of the subjects were assessed using dual-energy X-ray absorptiometry. Data on their lifestyle, their current medical diseases and their medications was collected during a personal interview with using a questionnaire at the initial examination. Height, body weight, waist circumference, blood pressure, fasting blood glucose and the serum lipid profiles were measured.
Results: In the adjusted analysis with including age and the body mass index, blood pressure and the triglyceride level had a close correlation with BMD (P<0.05). After adjustment for age, waist circum- ference, systolic- and diastolic blood pressure, BMD revealed significant correlation with the presence of metabolic syndrome (P=0.037).
Conclusion: BMD measures in Korean postmenopausal women with no prior history of cardiovascular disease were inversely related to metabolic syndrome, independent of age, waist circumference, systolic- and diastolic blood pressure, total cholesterol and triglyceride as risk factors for atherosclerosis and CVD.
Key Words: Risk factors of cardiovascular disease, Bone mineral density, Postmenopausal women
Received: June 22, 2010 Revised: June 30, 2010 Accepted: July 1, 2010
Corresponding Author: Heung Yeol Kim, Department of Obstetrics
& Gynecology, College of Medicine, Kosin University, 34 Amnam-dong, Seo-gu, Busan 602-702, Korea
Tel: +82-51-990-6226, Fax: +82-51-990-3300 E-mail: [email protected]
Atherosclerosis and osteoporosis are degenerative diseases common in the elderly population, and their prevalence is increasing1,2. Vascular and skeletal bio-
logy may share some common pathophysiological mecha- nisms, suggested by similarities between vascular calcification and bone formation3. Arterial tissue is calcified in an organized, regulated process by mecha- nisms similar to those involved in the mineralization of bone. Vascular disease is accompanied by loss of bone mineral density (BMD), more severe in the hip and lower extremity more affected by atherosclerosis4. Low bone mass has been related to increased cardiovascular
mortality5,6, cardiovascular morbidity7-12, and subclinical markers of atherosclerosis, including vascular calcifi- cation13-21 in cross-sectional as well as longitudinal epidemiologic studies.
Although several lines of evidence suggest a link between cardiovascular disease (CVD) and osteoporosis, the nature of this link and the mechanisms involved are still not clearly elucidated22. Postmenopausal women with osteoporosis are at increased risk for acute cardiovascular events independent of their age and cardiovascular risk profile, and the increase in risk is proportional to the severity of osteoporosis at the time of the diagnosis9. The metabolic syndrome is a cluster of conditions with detrimental effects on cardiovascular health and a known association with low-grade inflam- mation23,24. The metabolic syndrome includes obesity, dyslipidemia, impaired glucose tolerance, and hyperten- sion25. The proinflammatory state associated with the metabolic syndrome may lead to a reduction in bone mass26. Until now there were few studies that investiga- ted associations between BMD and risk factors of atherosclerosis and CVD in postmenopausal women in Korea. The aim of the present study was to investigate relationship between BMD and risk factors of atherosclerosis and CVD, to test association between BMD and metabolic syndrome as an endpoint of risk factors for atherosclerosis and CVD in 193 Korean postmenopausal women providing full-set of data for such analyses.
MATERIALS AND METHODS
1. Subjects
We identified 193 subjects with the postmenopausal state who visited a health promotion center of an university hospital from January, 2007 to December, 2009. We used following profiles as risk factors27,28 of atherosclerosis and CVD: current smoker; no regular exercise; obesity (body mass index, BMI≥25);
abdominal obesity (waist circumference≥85 cm in
women); hypercholesterolemia≥240 mg/dL; low high density lipoprotein (HDL) cholesterol<35 mg/dL; high low density lipoprotein (LDL) cholesterol≥160 mg/dL;
hypertriglyceridemia≥200 mg/dL; hypertension (blood pressure≥140/90 mmHg or use of antihypertensive medication); diabetes mellitus (fasting glucose≥126 mg/dL or use of antidiabetic medication).
Exclusion criteria included having a history of: (1) taking drugs known to influence bone metabolism in the past 2 years, such as vitamin D, calcium, cortico- steroids, bisphosphonates and hormone replacement therapy; (2) musculoskeletal, thyroid, parathyroid, adrenal, hepatic, or renal disease; (3) malignancy; and (4) history of coronary heart disease or stroke.
We defined metabolic syndrome as an endpoint of risk for atherosclerosis and cardiovascular disease. We identified subjects with the metabolic syndrome according to the criteria of the Adult Treatment Panel III using NHANES III25. Subjects were considered to have the metabolic syndrome if they had three or more of the following abnormalities: abdominal obesity (waist circumference>80 cm in women); hypertrigly- ceridemia≥150 mg/dL; low HDL-cholesterol <50 mg/dL in women; high blood pressure≥130/85 mmHg or use of antihypertensive medication; or high fasting glucose
≥110 mg/dL or use of antidiabetic medication (insulin or oral agents).
2. Anthropometric measurements
Body weight and height were measured to the closest 0.1 kg and 0.1 cm, respectively, in subjects wearing light indoor clothing and no shoes at the time of bone densitometry measurements. BMI (kg/m2) was calcula- ted as body weight (in kg) divided by height squared (in m). Resting blood pressure was measured 2 times by OMRON T5-MⓇ (OMRON Corp., Japan) in the seated position, and the average of the 2 measurements was used in the analysis.
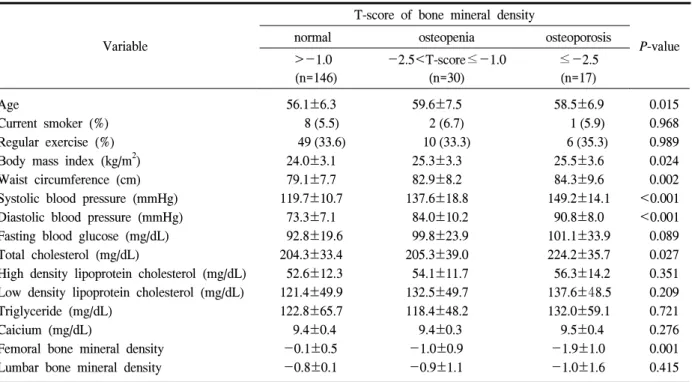
Table 1. Characteristics of subjects according to T-score of bone mineral density in postmenopausal women (n=193)
Variable
T-score of bone mineral density
P-value
normal osteopenia osteoporosis
>-1.0 (n=146)
-2.5<T-score≤-1.0 (n=30)
≤-2.5 (n=17) Age
Current smoker (%) Regular exercise (%) Body mass index (kg/m2) Waist circumference (cm) Systolic blood pressure (mmHg) Diastolic blood pressure (mmHg) Fasting blood glucose (mg/dL) Total cholesterol (mg/dL)
High density lipoprotein cholesterol (mg/dL) Low density lipoprotein cholesterol (mg/dL) Triglyceride (mg/dL)
Caicium (mg/dL)
Femoral bone mineral density Lumbar bone mineral density
56.1±6.3 8 (5.5) 49 (33.6) 24.0±3.1 79.1±7.7 119.7±10.7 73.3±7.1 92.8±19.6 204.3±33.4 52.6±12.3 121.4±49.9 122.8±65.7 9.4±0.4
-0.1±0.5 -0.8±0.1
59.6±7.5 2 (6.7) 10 (33.3) 25.3±3.3 82.9±8.2 137.6±18.8 84.0±10.2 99.8±23.9 205.3±39.0 54.1±11.7 132.5±49.7 118.4±48.2 9.4±0.3
-1.0±0.9 -0.9±1.1
58.5±6.9 1 (5.9) 6 (35.3) 25.5±3.6 84.3±9.6 149.2±14.1 90.8±8.0 101.1±33.9 224.2±35.7 56.3±14.2 137.6±48.5 132.0±59.1 9.5±0.4
-1.9±1.0 -1.0±1.6
0.015 0.968 0.989 0.024 0.002
<0.001
<0.001 0.089 0.027 0.351 0.209 0.721 0.276 0.001 0.415 Data shown are mean±SE or percentages.
Note: P-value by ANOVA.
3. Biochemical measurements
Blood samples were collected in the morning after fasting overnight (>12 h). Serum fasting glucose, total cholesterol, triglyceride, HDL cholesterol, and calcium were measured. LDL cholesterol was calculated by Friedewald formula (LDL-C=TC-HDL-C-0.45xTG).
4. Bone mineral density (BMD)
Lumbar BMD (L-BMD) and femoral BMD (F-BMD) were measured by dual energy X-ray absorptiometry (DXA) using a Lunar Prodigy AdvanceTM (GE Medical System, Madison, WI, USA). The results were given in grams of mineral bone matrix/cm2 and standarad deviations relative to the mean bone mineral density found in: (1) a young adult population of the same gender with peak bone mass (T-score) and (2) a population in the same age group and of the same size and gender (Z-score).
5. Measurement of Covariates
Information on age, smoking habits, weekly exercise, medication, prevalent diabetes and cardiovascular dise- ases (stroke, coronary events, intermittent claudication, unstable angina) were collected during personal inter- view using a questionnaire at the initial examination.
6. Statistical analysis
Statistical analysis was performed with the PASWⓇ Regression 17.0 version (SPSS Inc., Chicago, IL, USA). Values are expressed as mean±SE or percen- tages. Baseline characteristics of subjects by BMD were compared by ANOVA. The association with BMD and risk factors of atherosclerosis and CVD was assessed by linear regression analysis. We used multivariable logistic regression models to assess factors showing the relationship between the BMD and risk factors of atherosclerosis and CVD. P<0.05 was considered statistically significant.
Table 2. Relationship between bone mineral density and the risk factors of atherosclerosis and cardiovascular disease in postmenopausal women (n=193)
Variable Beta coefficients P-value
Waist circumference (cm) Systolic blood pressure (mmHg) Diastolic blood pressure (mmHg) Fasting blood glucose (mg/dL) Total cholesterol (mg/dL)
High density lipoprotein cholesterol (mg/dL) Low density lipoprotein cholesterol (mg/dL) Triglyceride (mg/dL)
0.075 0.368 0.312 0.003 0.031 0.020 0.063 -0.152
0.408 <0.001 0.001 0.956 0.577 0.727 0.316 0.017 Note: P-value by linear regression analysis, adjusted by age, body mass index
Table 3. Odds ratios (95% confidence interval) for metabolic syndrome by grade of the T-score of BMD in postmenopausal women (n=193)
T-score of bone mineral density
normal osteopenia osteoporosis P
>-1.0 (n=146)
-2.5<T-score≤-1.0 (n=30)
≤-2.5 (n=17)
Model 1* 1 1.06 (1.03~1.23) 1.19 (1.08~1.31) 0.037
Model 2† 1 1.12 (1.01~1.24) 1.31 (1.13~1.51) <0.001
*Model 1: Adjusted for age, waist circumference, systolic blood pressure, and diastolic blood pressure; †Model 2:
Adjusted as model 1 plus total cholesterol and triglyceride.
Note: P-value by multivariable logistic regression analysis
RESULTS
1. Demographic characteristics
Demographic characteristics of the population by T-score of BMD are shown in Table 1. The means of BMI, waist circumference, systolic- and diastolic blood pressure, total cholesterol, and F-BMD were different among groups by T-score of BMD. There were no significant differences among the groups in smoking, regular exercise, fasting blood glucose, HDL-chole- sterol, LDL-cholesterol, Triglyceride, serum calcium and L-BMD.
2. Bone mineral density and the risk factors of atherosclerosis and cardiovascular disease
As shown in Table 2, BMD was not associated with
waist circumference, fasting blood glucose, total cholesterol, HDL-cholesterol, and LDL-cholesterol. In adjusted analysis including age and body mass index, blood pressure and triglyceride had a close correlation with BMD (P<0.05).
3. Multiple regression analysis of risk factors independently associated with femoral BMD
After adjustment for age, waist circumference, systolic- and diastolic blood pressure, BMD revealed significant correlation with the presence of metabolic syndrome (P=0.037) (Table 3). In analyses stratified by BMD, the odds ratio was higher in women with the metabolic syndrome than controls after adjustment for age, waist circumference, systolic- and diastolic blood pressure, total cholesterol and triglyceride (P<0.001)
(Table 3).
DISCUSSION
In Korean postmenopausal women, we observed that a decrease in BMD was related to increased risk for metabolic syndrome as an endpoint of risk factors for atherosclerosis and CVD. These associations were consistent with previous findings. Diagnosis of osteoporosis indicate an increase in risk for cardiovascular disease, even when adjusted for age, prior cardiovascular disease, hypertension, hyper- lipidemia, diabetes, smoking6,11,14,15,19,29,30
, suggesting that the increased risk cannot be explained by common risk factors. These analyses, adjusted for sex, age, BMI, and genetic relationships, revealed that subjects with a CVD history had significantly lower femoral neck BMD31.
Cardiovascular disease and osteoporosis are linked by a common denominator acting in parallel on both vascular and bone cells32,33. These conditions progress silently until a fracture or myocardial infarction occurs34,35. The association may be only indirect, such that individuals having specific lifestyles or behaviors may be at risk for both disorders, or it may be more direct, with common biological processes contributing jointly to accelerated loss of bone and increased cardiovascular risk31. Reports on this association focused mostly on white postmenopausal women and less is known about the presence of such relationships in other ethnic groups22. We examined it in Korean postmenopausal women. There was significantly different in BMI, waist circumference, systolic- and diastolic blood pressure, total cholesterol, and F-BMD among postmenopausal women in Korea. Waist circumference is the most important factor in this association, suggesting that inflammatory cytokines secreted from visceral fat might be an important factor in bone loss36. Therefore, the diagnosis of osteoporosis may draw attention to vascular disease, regardless of
demographic and lifestyle characteristics of the subject.
The increase in risk for cardiovascular events associated with prior fracture suggests that the association with increased hospitalization and mortality37 may be at least in part attributable to coronary and stroke events.
Estimates of the relative risk for vertebral and hip fractures are about 5- and 3-fold more common, respectively, in subjects with vascular calcification. The vertebral fractures are generally only those coming to clinical attention. Since routine radiography is not performed, symptomless, prevalent, or incident vertebral fractures, which may represent up to two-thirds of all morphometric vertebral deformities, may have been undetected. The mechanism by which osteoporosis and cardiovascular disease may be linked is not fully understood38,39, although age, diabetes, dyslipidemia, and hypertension are all established risk factors for cardiovascular disease that also have been associated with decreased BMD or increased fracture risk38. There are several potential limitations to this cross-sectional study. First, the subjects were not recruited from the community at large, but were selected from patients who visited to check their health conditions. Second, we have no direct histopathological demonstration due to atherosclerosis as an endpoint of risk factors for atherosclerosis and CVD. Further research should elucidate possible pathophysiological mechanisms linking osteoporosis and CVD. An understanding of these mechanisms will set the stage for the potential use of common preventive and therapeutic interventions targeted at both conditions.
CONCLUSION
BMD measures in Korean postmenopausal women with no prior history of cardiovascular disease were inversely related to metabolic syndrome, independent of age, waist circumference, systolic- and diastolic blood pressure, total cholesterol and triglyceride as risk factors for atherosclerosis and CVD.
REFERENCE
1. Braithwaite RS, Col NF, Wong JB. Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc 2003;51:364-70.
2. Wenger NK. Coronary heart disease: the female heart is vulnerable. Prog Cardiovasc Dis 2003;46:
199-229.
3. Demer LL, Tintut Y. Mineral exploration: search for the mechanism of vascular calcification and beyond: the 2003 Jeffrey M. Hoeg Award lecture.
Arterioscler Thromb Vasc Biol 2003;23:1739-43.
4. Laroche M, Moulinier L, Leger P, Lefebvre D, Mazieres B, Boccalon H. Bone mineral decrease in the leg with unilateral chronic occlusive arterial disease. Clin Exp Rheumatol 2003;21:103-6.
5. Mussolino ME, Madans JH, Gillum RF. Bone mineral density and mortality in women and men:
the NHANES I epidemiologic follow-up study.
Ann Epidemiol 2003;13:692-7.
6. Trivedi DP, Khaw KT. Bone mineral density at the hip predicts mortality in elderly men. Osteoporos Int 2001;12:259-65.
7. Farhat GN, Strotmeyer ES, Newman AB, Sutton- Tyrrell K, Bauer DC, Harris T, et al. Volumetric and areal bone mineral density measures are associated with cardiovascular disease in older men and women: the health, aging, and body composi- tion study. Calcif Tissue Int 2006;79:102-11.
8. Marcovitz PA, Tran HH, Franklin BA, O'Neill WW, Yerkey M, Boura J, et al. Usefulness of bone mineral density to predict significant coronary artery disease. Am J Cardiol 2005;96:1059-63.
9. Tankó LB, Christiansen C, Cox DA, Geiger MJ, McNabb MA, Cummings SR. Relationship between osteoporosis and cardiovascular disease in post- menopausal women. J Bone Miner Res 2005;20:
1912-20.
10. Magnus JH, Broussard DL. Relationship between bone mineral density and myocardial infarction in
US adults. Osteoporos Int 2005;16:2053-62.
11. Samelson EJ, Kiel DP, Broe KE, Zhang Y, Cupples LA, Hannan MT, et al. Metacarpal cortical area and risk of coronary heart disease: the Framingham Study. Am J Epidemiol 2004;159:589- 95.
12. Jorgensen L, Engstad T, Jacobsen BK. Bone mineral density in acute stroke patients: low bone mineral density may predict first stroke in women.
Stroke 2001;32:47-51.
13. Schulz E, Arfai K, Liu X, Sayre J, Gilsanz V.
Aortic calcification and the risk of osteoporosis and fractures. J Clin Endocrinol Metab 2004;89:4246- 53.
14. Tankò LB, Bagger YZ, Christiansen C. Low bone mineral density in the hip as a marker of advanced atherosclerosis in elderly women. Calcif Tissue Int 2003;73:15-20.
15. Kiel DP, Kauppila LI, Cupples LA, Hannan MT, O'Donnell CJ, Wilson PW. Bone loss and the progression of abdominal aortic calcification over a 25 year period: the Framingham Heart Study.
Calcif Tissue Int 2001;68:271-6.
16. Wong SY, Kwok T, Woo J, Lynn H, Griffith JF, Leung J, et al. Bone mineral density and the risk of peripheral arterial disease in men and women:
results from Mr. and Ms Os, Hong Kong. Osteo- poros Int 2005;16:1933-8.
17. van der Klift M, Pols HA, Hak AE, Witteman JC, Hofman A, de Laet CE. Bone mineral density and the risk of peripheral arterial disease: the Rotter- dam Study. Calcif Tissue Int 2002;70:443-9.
18. Jorgensen L, Joakimsen O, Rosvold Berntsen GK, Heuch I, Jacobsen BK. Low bone mineral density is related to echogenic carotid artery plaques: a population-based study. Am J Epidemiol 2004;160:
549-56.
19. Pennisi P, Signorelli SS, Riccobene S, Celotta G, Di Pino L, La Malfa T, et al. Low bone density and abnormal bone turnover in patients with
atherosclerosis of peripheral vessels. Osteoporos Int 2004;15:389-95.
20. Hirose K, Tomiyama H, Okazaki R, Arai T, Koji Y, Zaydun G, et al. Increased pulse wave velocity associated with reduced calcaneal quantitative osteo-sono index: possible relationship between atherosclerosis and osteopenia. J Clin Endocrinol Metab 2003;88:2573-8.
21. Sanada M, Taguchi A, Higashi Y, Tsuda M, Kodama I, Yoshizumi M, et al. Forearm endothelial function and bone mineral loss in postmenopausal women. Atherosclerosis 2004;176:387-92.
22. Farhat GN, Cauley JA, Matthews KA, Newman AB, Johnston J, Mackey R, et al. Volumetric BMD and vascular calcification in middle-aged women:
the Study of Women's Health Across the Nation. J Bone Miner Res 2006;21:1839-46.
23. Lee WY, Park JS, Noh SY, Rhee EJ, Sung KC, Kim BS, et al. C-reactive protein concentrations are related to insulin resistance and metabolic synd- rome as defined by the ATP III report. Int J Cardiol 2004;97:101-6.
24. Mueller C, Laule-Kilian K, Christ A, Brunner-La Rocca HP, Perruchoud AP. Inflammation and long-term mortality in acute congestive heart failure. Am Heart J 2006;151:845-50.
25. Durso SC. A piece of my mind. A survivor's way.
JAMA 2002;288:287-8.
26. Ganesan K, Teklehaimanot S, Tran TH, Asuncion M, Norris K. Relationship of C-reactive protein and bone mineral density in community-dwelling elderly females. J Natl Med Assoc 2005;97:329-33.
27. Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories.
Circulation 1998;97:1837-47.
28. Folsom AR, Chambless LE, Ballantyne CM, Coresh J, Heiss G, Wu KK, et al. An assessment of incremental coronary risk prediction using C-reactive protein and other novel risk markers: the
atherosclerosis risk in communities study. Arch Intern Med 2006;166:1368-73.
29. Hak AE, Pols HA, van Hemert AM, Hofman A, Witteman JC. Progression of aortic calcification is associated with metacarpal bone loss during me- nopause: a population-based longitudinal study.
Arterioscler Thromb Vasc Biol 2000;20:1926-31.
30. von der Recke P, Hansen MA, Hassager C. The association between low bone mass at the meno- pause and cardiovascular mortality. Am J Med 1999;106:273-8.
31. Shen H, Bielak LF, Streeten EA, Ryan KA, Rumberger JA, Sheedy PF 2nd, et al. Relationship between vascular calcification and bone mineral density in the Old-order Amish. Calcif Tissue Int 2007;80:244-50.
32. Mody N, Tintut Y, Radcliff K, Demer LL.
Vascular calcification and its relation to bone calci- fication: possible underlying mechanisms. J Nucl Cardiol 2003;10:177-83.
33. Baldini V, Mastropasqua M, Francucci CM, D'Erasmo E. Cardiovascular disease and osteoporosis. J Endo- crinol Invest 2005;28:69-72.
34. NIH Consensus Development Panel on Osteoporo- sis Prevention, Diagnosis, and Therapy. Osteoporo- sis prevention, diagnosis, and therapy. JAMA 2001;
285:785-95.
35. Aronow WS. Silent MI. Prevalence and prognosis in older patients diagnosed by routine electro- cardiograms. Geriatrics 2003;58:24-6, 36-8, 40.
36. Kim HY, Choe JW, Kim HK, Bae SJ, Kim BJ, Lee SH, et al. Negative association between meta- bolic syndrome and bone mineral density in Koreans, especially in men. Calcif Tissue Int 2010;
86:350-8.
37. Ensrud KE, Thompson DE, Cauley JA, Nevitt MC, Kado DM, Hochberg MC, et al. Prevalent vertebral deformities predict mortality and hospitalization in older women with low bone mass. Fracture Intervention Trial Research Group. J Am Geriatr
Soc 2000;48:241-9.
38. McFarlane SI, Muniyappa R, Shin JJ, Bahtiyar G, Sowers JR. Osteoporosis and cardiovascular disease:
brittle bones and boned arteries, is there a link?
Endocrine 2004;23:1-10.
39. Abedin M, Tintut Y, Demer LL. Vascular calcifi- cation: mechanisms and clinical ramifications.
Arterioscler Thromb Vasc Biol 2004;24:1161-70.