165
• 교신저자:심봉석, 이화여자대학교 의학전문대학원 비뇨기과학교실 서울시 양천구 목동 911-1 우 158-710
Tel: 02-2650-5157, Fax: 02-2654-3682, E-mail: [email protected] Received: August 9, 2011
Revised: September 7, 2011 Accepted: September 16, 2011
급성 세균성 전립선염의 임상경과에 관한 다기관 연구
이화여자대학교 의과대학,
1가톨릭대학교 의과대학,
2국립경찰병원,
3경희대학교 의과대학,
4
서울대학교 의과대학,
5순천향대학교 의과대학,
6아주대학교 의과대학,
7
중앙대학교 의과대학,
8건국대학교 의과대학,
9단국대학교 의과대학,
10충남대학교 의과대학,
11
한림대학교 의과대학,
12원광대학교 의과대학,
13전남대학교 의과대학,
14
조선대학교 의과대학,
15고신대학교 의과대학,
16동국대학교 의과대학,
17
동아대학교 의과대학,
18인제대학교 의과대학,
19부산대학교 의과대학 비뇨기과학교실
이성주∙구진모∙심봉석∙조용현1∙한창희1∙민승기2∙이선주3∙손환철4∙김준모5∙최종보6 김태형7∙양상국8∙이길호9∙나용길10∙이성호11∙정희종12∙정승일13∙김철성14∙정재민15
서영진16∙조원열17∙민권식18∙이상돈19
[Abstract]
Clinical Outcome of Acute Bacterial Prostatitis; A Multicenter Study Seong Ju Lee, Jin Mo Koo, Bong Suk Shim, Yong Hyun Cho
1, Chang Hee Han
1, Seung Ki Min
2, Sung Joo Lee
3, Hwan Cheol Son
4,
Jun Mo Kim
5, Jong Bo Choi
6, Tae Hyoung Kim
7, Sang Kuk Yang
8, Kil Ho Lee
9, Yong Kil Na
10, Sung Ho Lee
11, Hee Jong Jung
12, Seung Il Jung
13,
Chul Sung Kim
14, Jae Min Chung
15, Young Jin Seo
16, Won Yeol Cho
17, Kweon Sik Min
18, Sang Don Lee
19From the Department of Urology, Ewha University, 1Catholic University, 2National Police Hospital,
3Kyung Hee University, 4Seoul National University, 5Soonchunhyang University, 6Ajou University,
7Chungang University, 8Konkuk University, 9Dankuk University, 10Chungnam National University, 11Hallym University,
12Wonkwang University, 13Chonnam National University, 14Chosun University, 15Kosin University, 16Dongguk University,
17Dong-A University, 18Inje University, 19Pusan National University
Purpose: Proper guidelines concerning antibiotic administration for acute bacterial prostatitis (ABP) are unclear.
We retrospectively analyzed treatment status and clinical outcomes to establish a proper treatment guideline.
Materials and Methods: The clinical records of 669 patients from 21 hospitals diagnosed with ABP
were reviewed. Prior manipulation, antibiotics administration, mean length of treatment, complication and procedure were analyzed.
Results: The mean age of 538 patients (80.4%) without manipulation (group 1) and 131 patients
(19.6%) with manipulation (group 2) was 58.3 years (range 19-88 years). Transrectal prostate biopsy was the most common cause of acute bacterial prostatitis (n=66; 50.4%). Of the clinical symptoms in the non-manipulation and manipulation groups, fever was most common (88.2% and 86.3%, respectively).
Acute urinary retention (14.3% and 28.1%, respectively) was significantly increased in the manipulation group (p<0.05). Escherichia coli was the most frequently isolated bacterium from urine (72.0% and 66.7%
of cases, respectively). Mean length of treatment was 6.5days and 7.9days, respectively; the difference was significant (p<0.05). Combination antibiotic therapy with third generation cephalosporin+aminoglycoside was used in 49.3% and 55.5% of cases, respectively. For single antibiotic therapy, second generation qui- nolones were used the most (35.5% and 34.3%, respectively). Sequale occurred in 29 group 1 patients (5.4%) and 20 group 2 patients (15.3%); the difference was significant (p<0.05).
Conclusions: Prior manipulation was associated with 20% of ABP patients. Regardless of manipulation,
clinical outcome was similar after treating with appropriate antibiotics. (Korean J UTII 2011;6:165-170)
Key Words: Anti-bacterial agents, Prostatitis, Treatment, Outcome
서 론
열성 요로감염 질환인 급성 전립선염은 실제 전 립선의 감염상태를 직접 확인하기 어려워 임상증 상에 따라 진단되어 치료방식이 결정된다.
1이는 전립선염의 5% 정도를 차지하고 치료하지 않으면 패혈증 같은 치명적인 결과까지 초래할 수 있으나 대부분 어렵지 않게 치료할 수 있다.
2-4현재는 전 신증상이 있으면 항생제 경정맥 투여로 치료를 시 작하고 이후 경구용 항생제로 전환한다.
5보통 항 생제는 2-4주간 투여하지만 아직까지 투여 방법 및 기간에 대한 지침이 정립되지 않은 상태이다.
6이에 저자들은 술기 여부에 따른 치료를 비교하 였고 급성 전립선염은 발병률이 낮기에 다기관 연 구를 통한 치료실태 및 임상경과를 파악하고 향후 치료지침을 위한 기초자료로 삼고자 하였다.
대상 및 방법
2007년 1월부터 2009년 12월까지 전국 21개 종합 병원을 대상으로 급성 전립선염으로 치료받은 환 자 669명의 의무기록을 후향적으로 조사하였다. 급 성 전립선염은 임상증상 (발열, 하부요로증상)과 혈 액검사 결과 (백혈구증가증)를 토대로 진단하였다.
증상과 요배양검사 양성인 경우 환자군에 포함시 켰고 증상은 있으나 이전 항생제 치료에 의한 요배 양검사 음성인 경우는 제외시켰다. 또한 급성 전립 선염과 직접적 연관이 없는 만성질환 (고혈압, 당 뇨)이 있는 경우 포함시켰고 다른 열성 요로감염 (신우신염, 고환염)이 동반된 경우는 제외시켰다.
발병 전 비뇨기과적 술기 여부에 따라 두 군으로 나누어 그에 따른 임상증상, 배양균, 투여 항생제 종류와 기간, 합병증 및 처치 등을 조사하였다.
통계학적 검증은 chi-square test, Student's t-test를
이용하였으며, p 값이 0.05 미만일 때 통계학적으로
유의한 것으로 판정하였다.
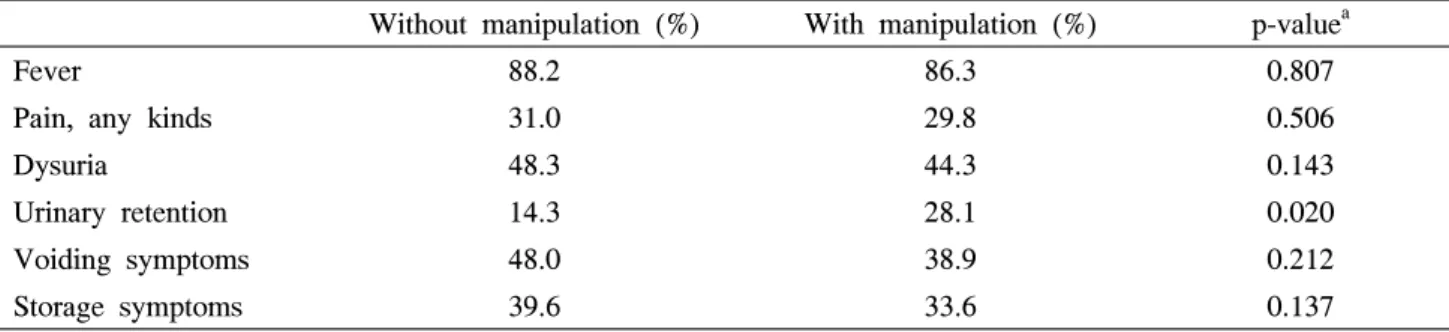
Table 2. Comparison of clinical symptoms between manipulation group and no manipulation group in patients
with acute bacterial prostatitis
Without manipulation (%) With manipulation (%) p-value
aFever 88.2 86.3 0.807
Pain, any kinds 31.0 29.8 0.506
Dysuria 48.3 44.3 0.143
Urinary retention 14.3 28.1 0.020
Voiding symptoms 48.0 38.9 0.212
Storage symptoms 39.6 33.6 0.137
a: chi-square test
-19 20-29 30-39 40-49 50-59 60-69 70- Age
200
150
100
50
0
with manipulation without manipulation
Fig. 1. Age distibution in patients with acute bacterial
prostatitis according to with or without manipulation.
Table 1. Prior manipulation in patients with acute
bacterial prostatitis
No. patients (%) Without manipulation 538 (80.4)
With manipulation 131 (19.6)
Prostate biopsy 66 (50.4) Foley catheterization 26 (19.8) Operation via urethra 11 ( 8.4) Cystoscopy 10 ( 7.6) Urodynamic study 9 ( 6.9) Digital rectal examination 4 ( 3.1) Others 5 ( 3.8)
결 과
비처치군 538명 (80.4%), 처치군 131명 (19.6%)으 로 평균연령은 58.3 (19-88)세였고 60대가 138명 (25.7%)으로 가장 많았으나 두 군 간 연령에 따른 유의성은 보이지 않았다 (p<0.05) (Fig. 1). 처치는 전립선조직검사가 66명 (50.4%)으로 가장 많았다 (Table 1). 임상증상은 두 군 모두 발열이 88.2%, 86.3%로 가장 흔했으며, 급성요폐가 14.3%, 28.1%
로 처치군에서 유의하게 많았다 (p<0.05) (Table 2).
배양균은 두 군 모두 대장균이 72.0%, 66.7%로 가 장 많았고 녹농균은 4.9%, 11.6%로 처치군에서 유 의하게 높은 비율을 보였다 (p<0.05) (Table 3). 입
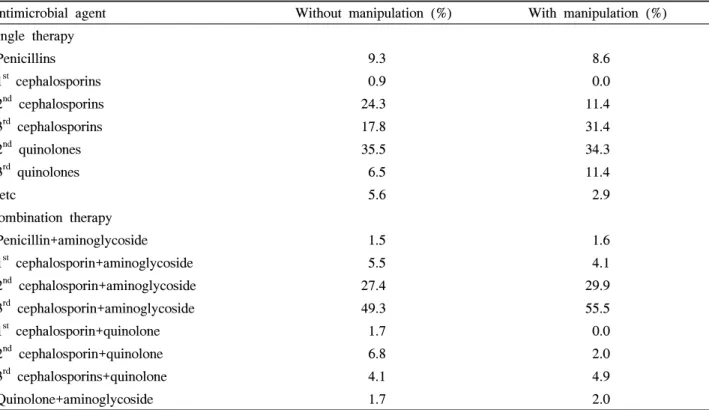
원치료는 각각 109명 (20.3%), 128명 (97.7%)이었고 치료 기간은 6.5일, 7.9일로 처치군에서 유의하게 길었다 (p<0.05) (Fig. 2). 항생제 처방은 3
rdcepha- losporin과 aminoglycoside 병합처방이 49.3%, 55.5%
였고 단독처방은 2
ndquinolones이 35.5%, 34.3%로
가장 많았다 (Table 4). 후유증으로는 농양이 29명
(5.4%), 20명 (15.3%)로 처치군에서 유의하게 많았
고 (p<0.05) 그에 따른 치료로 비처치군에서 경요도
배농, 회음부흡입, 약물치료 순으로 14명 (48.3%), 8
명 (27.6%), 7명 (24.1%)이 시행되었고, 처치군에서
8명 (40%), 9명 (45.0%), 3명 (15.0%)이 시행되었다
(Table 5).
Table 3. Microbiological spectrum according to urine culture in patients with acute bacterial prostatitis
Without manipulation (%) With manipulation (%) Total (%)
Negative 356 (66.2) 62 (47.3) 418 (62.5)
Positive 182 (33.8) 69 (52.7) 251 (37.5)
E. coli 72.0 66.7 70.5
K. pneumoniae 8.8 7.2 8.4
P. aeruginosa 4.9 11.6 6.8
E. faecalis 4.9 7.2 5.6
S. aureus 3.8 5.8 4.4
Proteus 1.6 1.4 1.6
Table 4. Distribution of prescribed antimicrobial agents in patients with acute bacterial prostatitis
Antimicrobial agent Without manipulation (%) With manipulation (%)
Single therapy
Penicillins 9.3 8.6
1st cephalosporins 0.9 0.0
2nd cephalosporins 24.3 11.4
3rd cephalosporins 17.8 31.4
2nd quinolones 35.5 34.3
3rd quinolones 6.5 11.4
etc 5.6 2.9
Combination therapy
Penicillin+aminoglycoside 1.5 1.6
1st cephalosporin+aminoglycoside 5.5 4.1
2nd cephalosporin+aminoglycoside 27.4 29.9
3rd cephalosporin+aminoglycoside 49.3 55.5
1st cephalosporin+quinolone 1.7 0.0
2nd cephalosporin+quinolone 6.8 2.0
3rd cephalosporins+quinolone 4.1 4.9
Quinolone+aminoglycoside 1.7 2.0
고 찰
전립선염의 분류에서 급성 전립선염은 5% 미만 으로 비뇨기적으로 드문 질환이지만 갑작스런 고열 과 오한, 하부요통, 회음부통증, 빈뇨, 요급박, 야간 뇨, 배뇨통 및 배뇨곤란 등 하부요로증상을 보이고 근육통, 관절통의 증상이 나타나므로 임상증상으로 진단이 가능하고 치료가 잘되는 것으로 알려져 있
다.
7-9본 연구에서도 고열이 주 증상이었고, 증상 발 현 후 대부분 3일 이내에 외래나 응급실을 경유하 여 입원하였으며, 평균 7일 이내에 퇴원하였다.
10요검사에서 대부분 농뇨 소견을 보이는데 본 연구 에서도 80%로 나타났으며 일반 균배양검사 양성률 은 37%로 기존 연구들에 비해 약간 낮은 수치를 보 였다.
11원인균은 80%가 E. coli로 알려져 있는데,
12,13본 연구에서도 E. coli가 가장 흔한 균으로 나타났다.
균배양 검사 양성률이 기존에 비해 낮게 나타난 것
Table 5. Formation incidence and management of prostatic abscess
Prostatic abscess Without manipulation (%) With manipulation (%) p-value
Formation incidence 29 (5.4) 20 (15.3) 0.032a
Management
Medical therapy 7 (24.1) 3 (15.0)
Perineal aspiration 8 (27.6) 9 (45.0)
Transurethral drainage 14 (48.3) 8 (40.0)
a: Student’s t-test
manipulation (-) manipulation (+) 25
20 15
10 5
0
admission after admission out-patient
Fig. 2. Mean length of antibiotics therapy in patients