CASE REPORT
저위전방절제술 후에 발생한 특발성 후복막강 섬유증과 모자 용종증 1예
송림화, 전병우, 박지현, 김다민, 장동경, 김영호, 김재준, 김진용
성균관대학교 의과대학 삼성서울병원 내과학교실
A Case of Cap Polyposis Complicated with Idiopathic Retroperitoneal Fibrosis
Limhwa Song, Byung Woo Jhun, Jihyeon Park, Damin Kim, Dong Kyung Chang, Young Ho Kim, Jae Jun Kim and Jin Yong Kim Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
An optimal treatment for cap polyposis has not been established. Several treatment approaches, including anti-inflammatory agents, antibiotics, immunomodulators, and endoscopic therapy have been described. Surgical resection of the affected colon and rectum may be indicated for patients with persistent disease. Repeat surgery is indicated in cases of recurrence after surgery. However, symptomatic polyposis may still recur, and spontaneous resolution of cap polyposis is possible. We report a case of recurrent cap polyposis complicated with retroperitoneal fibrosis after inadequate low anterior resection with a positive resection margin. Surgical approaches for the treatment of cap polyposis should be carefully considered before treatment.
(Korean J Gastroenterol 2011;58:275-279)
Key Words: Cap polyposis; Retroperitoneal fibrosis; Prednisolone; Low anterior resection
Received April 27, 2011. Revised July 24, 2011. Accepted July 28, 2011.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
교신저자: 김진용, 135-710, 서울시 강남구 일원동 50, 성균관대학교 의과대학 삼성서울병원 내과학교실
Correspondence to: Jin Yong Kim, Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 50, Irwon-dong, Gangnam-gu, Seoul 135-710, Korea. Tel: +82-2-3410-1629, Fax: +82-2-3410-6983, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
INTRODUCTION
Cap polyposis is a rare, benign colorectal condition charac- terized by multiple polyps covered with a thick layer of fi- brinopurulent exudates. The diagnosis may be established during colonoscopy by typical colonoscopic findings.1 The most commonly involved sites are the sigmoid colon and rec- tum, but the condition sometimes extends as far as the cecum. An optimal treatment for cap polyposis has not been established. Several alternative approaches, including an- ti-inflammatory agents, antibiotics, immunomodulators, and endoscopic therapy have been described. Surgical resection of the affected colon and rectum may be indicated for pa- tients with persistent disease. Géhénot et al.2 and Campbell
et al.3 reported a case of recurrence after surgery. Repeat surgery may be helpful in such cases, but there is no con- sensus regarding treatment for refractory cap polyposis.4
Retroperitoneal fibrosis is a rare disease characterized by ureteral obstruction due to the presence of retroperitoneal tissue, consisting of chronic inflammation and marked fi- brosis.5 The pathogenesis of idiopathic retroperitoneal fib- rosis is unclear. On the other hand, secondary retroperitoneal fibrosis may be caused by different factors.6 Major abdomi- nal surgeries, including colectomy, lymphadenectomy, and aortic aneurysmectomy are known to induce retroperitoneal fibrosis.7,8
We report a case of cap polyposis with retroperitoneal fib- rosis after surgical treatment by low anterior resection.
Fig. 1. Abdomino-pelvic CT finding. (A) It showed soft tissue infiltrations (arrow) surrounding the presacral space. (B) Associated hydronephroureterosis was noted.
Fig. 2. Colonoscopic image. Sessile polyps with caps of purulent exudates were observed.
CASE REPORT
A 45-year-old woman with hematochezia and pain in both flanks was transferred to our hospital. She had experienced chronic constipation and straining on defecation for several years, which was occasionally managed with aloe and sitz baths. In September 2008, she had been admitted to anoth- er hospital for the evaluation of constipation, where colono- scopy revealed multiple polyps of various sizes with exudates from distal the rectum to the sigmoid colon. Microscopic ex- amination of biopsy specimens from a large polyp showed serrated adenoma. Low anterior resection and loop ileos- tomy were performed due to the size of the polyp. Microscopic examination of the surgical specimens also showed serrated adenoma with low grade dysplasia: 6×4.5 cm in size, with in- volvement of the distal resection margin and regional lymph node of reactive hyperplasia without tumor cells. The pa- tient’s constipation was resolved after surgery. In December 2008, she underwent ileostomy takedown. After surgery, she
complained of lower abdominal pain and persistent mucoid diarrhea that occurred more than 10 times per day. After a few weeks of medical treatment, she was transferred to our hospital.
The patient’s concentrations of acute-phase reactants were high: ESR, 64 mm/hour (normal: 0-27 mm/hour); CRP, 11.3 mg/dL (0-0.3 mg/dL). Enhanced abdomino-pelvic com- puted tomographic scans located ill-defined soft-tissue at- tenuations around the aortic bifurcation and presacral space, resulting in bilateral hydronephroureterosis (Fig. 1).
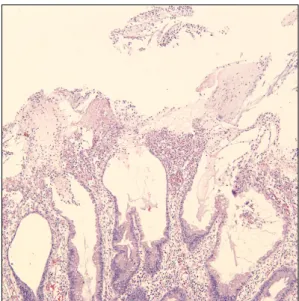
On retrograde pyelography, both ureters was medially dis- placed and narrowed. Bilateral double-J stent insertion was performed to resolve both hydronephroses. Colonoscopy re- vealed multiple, variable reddish sessile polyps with white fi- brinopurulent exudates (Fig. 2). Histolpathologic evaluation revealed hyperplastic glands without dysplasia and exudates of the mucosal surface (Fig. 3).
The patient underwent laparoscopic retroperitoneal biop- sy and adhesiolysis to exclude malignancy, resulting in a dif-
Fig. 3. Pathologic finding of colonoscopic biopy. It showed the surface of polyps covered by exudates (H&E, ×100).
Fig. 4. Pathologic findings of retrope- ritoneal biopsy. (A) It showed fibroblast and lymphocyte infiltration in fibrosis (H&E, ×100). (B) Numerous blood vessels and peripheral nerves were observed due to secondary post- inflammatory change (H&E, ×100).
Fig. 5. Follow-up endoscopic images.
It showed resolved cap polyposis.
ferential diagnosis of retroperitoneal fibrosis. Microscopic examinations of surgical specimens revealed fibroblasts and
lymphocyte infiltration. We observed hyperplasia of numer- ous blood vessels and peripheral nerves due to secondary post-inflammatory changes (Fig. 4). Autoimmune disease and several other causes of secondary retroperitoneal fib- rosis were excluded by blood tests. Based on these findings, we made a final diagnosis of cap polyposis with idiopathic ret- roperitoneal fibrosis.
The patient was treated with oral metronidazole for 10 days for Helicobacter pylori (H. pylori) eradication. However, her symptoms did not improve. An initial daily dose of pre- dnisolone 50 mg was administered to treat the patient’s ret- roperitoneal fibrosis. Ill-defined soft-tissue attenuation aro- und the aortic bifurcation and presacral space were de- creased at a follow-up enhanced CT examination 8 weeks af- ter the initiation of treatment. Surprisingly, the patient’s cap polyposis was much improved at follow-up colonoscopy 6 weeks after the treatment (Fig. 5).
DISCUSSION
Cap polyposis, which was first described in 15 patients by Williams et al.9 in 1985, is a benign colorectal condition char- acterized by multiple polyps covered with thick layer of fi- brinopurulent exudates.
The pathogenesis is unclear. Local ischemia to the colonic mucosa due to abnormal colonic motility and repeated trau- ma caused by straining during defecation are important fac- tors in the development of cap polyposis.10 Inflammatory bowel diseases and infectious agents such as H. pylori or Escherichia coli 018 are also possible causes in the absence of abnormal colonic motility.2,11 Similar to the present case, Cap polyposis has been described following pelvic surgery.2
The diagnosis of cap polyposis is established during colo- noscopy by recognizing the typical colonoscopic findings of erythematous polyps with adherent mucoid caps.
Drug therapies to treat cap polyposis are usually un- successful. In our patient, treatment with a soluble fiber sup- plement and avoidance of straining during defecation were ineffective. Symptomatic improvement after treatment with metronidazole12 alone or in combination with betametha- sone enemas13 have previously been reported. Symptoms and polyps may also disappear after eradication therapy for H. pylori.14 However, optimal treatment had not been es- tablished. Interestingly, Ohkawara et al.4 reported sponta- neous resolution of cap polyposis. Administration of budeso- nide enema was ineffective in our patient, and while H. pylori was identified in stomach biopsy specimens, eradication therapy was also ineffective. Patients with solitary cap polyps respond well to endoscopic polypectomy, while patients with multiple polyps and concurrent anorectal pathology require surgical resection.15 A previous study reported that four pa- tients who underwent anterior resection were all symp- tom-free at a median of 48 months (range, 18-72 months) af- ter surgery.15 However, cap polyposis may occur after pelvic surgery,2 and symptomatic polyposis can also recur.3,16 Kim et al.17 reported a case of cap polyposis that was remarkably improved after a single infliximab infusion and did not recur for 3 years. Our patient underwent low anterior resection, and then developed symptomatic polyposis with bilateral ureter- al obstruction due to retroperitoneal fibrosis.
Corticosteroids are the most useful drugs for the treat- ment of idiopathic retroperitoneal fibrosis. However, the opti-
mal dose and duration of steroid therapy are not established.
In our patient, an initial daily dose of prednisolone 50 mg was administered.18
This is the first report of cap polyposis with retroperitoneal fibrosis after surgery. Our patient’s cap polyposis was much improved after 6 weeks. The present case of cap polyposis was benign and had a self-limiting course.
REFERENCES
1. Esaki M, Matsumoto T, Kobayashi H, et al. Cap polyposis of the colon and rectum: an analysis of endoscopic findings. Endosco- py 2001;33:262-266.
2. Géhénot M, Colombel JF, Wolschies E, et al. Cap polyposis occur- ring in the postoperative course of pelvic surgery. Gut 1994;
35:1670-1672.
3. Campbell AP, Cobb CA, Chapman RW, et al. Cap polyposis--an un- usual cause of diarrhoea. Gut 1993;34:562-564.
4. Ohkawara T, Kato M, Nakagawa S, et al. Spontaneous resolution of cap polyposis: case report. Gastrointest Endosc 2003;
57:599-602.
5. Gilkeson GS, Allen NB. Retroperitoneal fibrosis. A true con- nective tissue disease. Rheum Dis Clin North Am 1996;
22:23-38.
6. Vaglio A, Salvarani C, Buzio C. Retroperitoneal fibrosis. Lancet 2006;367:241-251.
7. Hautekeete ML, Babany G, Marcellin P, et al. Retroperitoneal fib- rosis after surgery for aortic aneurysm in a patient with periarter- itis nodosa: successful treatment with corticosteroids. J Intern Med 1990;228:533-536.
8. Wilson MC, Berry AR, McNair TJ, Thomson JW. Obstructive urop- athy after pan-proctocolectomy for ulcerative colitis. Gut 1980;
21:808-809.
9. Williams GT, Bussey HJ, Morson BC. Inflammatory 'cap' polyps of the large intestine. Br J Surg 1985;72:S133.
10. Oriuchi T, Kinouchi Y, Kimura M, et al. Successful treatment of cap polyposis by avoidance of intraluminal trauma: clues to pathogenesis. Am J Gastroenterol 2000;95:2095-2098.
11. Akamatsu T, Nakamura N, Kawamura Y, et al. Possible relation- ship between Helicobacter pylori infection and cap polyposis of the colon. Helicobacter 2004;9:651-656.
12. Shimizu K, Koga H, Iida M, et al. Does metronidazole cure cap polyposis by its antiinflammatory actions instead of by its anti- biotic action? A case study. Dig Dis Sci 2002;47:1465-1468.
13. Kajihara H, Uno Y, Ying H, Tanaka M, Munakata A. Features of cap polyposis by magnifying colonoscopy. Gastrointest Endosc 2000;52:775-778.
14. Oiya H, Okawa K, Aoki T, Nebiki H, Inoue T. Cap polyposis cured by Helicobacter pylori eradication therapy. J Gastroenterol 2002;37:463-466.
15. Ng KH, Mathur P, Kumarasinghe MP, Eu KW, Seow-Choen F. Cap polyposis: further experience and review. Dis Colon Rectum 2004;47:1208-1215.
16. Konishi T, Watanabe T, Takei Y, Kojima T, Nagawa H. Confined progression of cap polyposis along the anastomotic line, im- plicating the role of inflammatory responses in the patho- genesis. Gastrointest Endosc 2005;62:446-447.
17. Kim ES, Jeen YT, Keum B, et al. Remission of cap polyposis main- tained for more than three years after infliximab treatment. Gut
Liver 2009;3:325-328.
18. van Bommel EF, Siemes C, Hak LE, van der Veer SJ, Hendriksz TR. Long-term renal and patient outcome in idiopathic retro- peritoneal fibrosis treated with prednisone. Am J Kidney Dis 2007;49:615-625.