Tuberc Respir Dis 2010;69:250-255
CopyrightⒸ2010. The Korean Academy of Tuberculosis and Respiratory Diseases. All rights reserved.
결핵균과 비결핵성항산균 검출에 Real-time PCR의 유용성
1
경상대학교 의학전문대학원 내과학교실,
2경상대학교 건강과학연구원,
3경상대학교 의학전문대학원 진단검사의학교실
윤은영1, 조수희1, 고세일1, 백종하1, 김유은1, 마정은1, 이기동1, 조유지1, 정이영1,2, 김호철1,2, 이종덕1,2, 김선주2,3, 황영실1,2
Usefulness of Real-time PCR to Detect Mycobacterium tuberculosis and Nontuberculous Mycobacteria
Eun Young Yun, M.D.
1, Su Hee Cho, M.D.
1, Se Il Go, M.D.
1, Jong Ha Baek, M.D.
1, You Eun Kim, M.D.
1, Jeong Eun Ma, M.D.
1, Gi Dong Lee, M.D.
1, Yu Ji Cho, M.D.
1, Yi Yeong Jeong, M.D.
1,2, Ho Cheol Kim, M.D.
1,2, Jong Deok Lee, M.D.
1,2, Sun-Joo Kim, M.D.
2,3, Young Sil Hwang, M.D.
1,21
Department of Internal Medicine, Gyeongsang National University School of Medicine,
2Gyeongsang Institute of Health Sciences, Gyeongsang National University,
3Department of Laboratory Medicine, Gyeongsang National University School of Medicine, Jinju, Korea
Background: The purpose of this study was to evaluate recently developed real-time polymerase chain reaction (PCR) assay kit to detect Mycobacterium tuberculosis (MTB) and nontuberculous mycobacteria (NTM) in respiratory specimens.Methods: We assessed the positive rate of the real-time PCR assay to detect MTB and NTM in 87 culture-positive specimens (37 sputum, 50 bronchial washing), which were performed real-time PCR by using Real-QTM MTB&NTM Kit from January 2009 to June 2009, at Gyeongsang University Hospital. To compare the efficacy with the TB-PCR assay, we evaluated 63 culture-positive specimens (19 sputum, 44 bronchial washing) for MTB or NTM, which were performed TB-PCR by using ABSOLUTETM MTB II PCR Kit from March 2008 to August 2008.
Results: Among 87 specimens tested using real-time PCR, MTB and NTM were cultured in 58 and 29, respectively.
The positive rate of real-time PCR assay to detect MTB was 71% (22/31) and 92.6% (25/27) in AFB stain-negative and stain-positive specimens. For NTM, the positive rate of real-time PCR was 11.1% (2/18) and 72.7% (8/11) in AFB stain-negative and stain-positive specimens. Among 63 specimens performed using TB-PCR, MTB and NTM were cultured in 46 and 17, respectively. The positive rate of TB-PCR was 61.7% (21/34) and 100% (12/12) in AFB stain-negative and stain-positive specimens. TB-PCR was negative in all NTM-cultured 17 specimens.
Conclusion: TB/NTM real-time PCR assay is useful to differentiate MTB and NTM in AFB stain-positive respiratory specimens and it is as effective in detecting MTB with TB-PCR.
Key Words: Mycobacterium tuberculosis; Mycobacteria, Atypical; Polymerase Chain Reaction, Real-Time
Address for correspondence: Ho Cheol Kim, M.D.
Department of Internal Medicine, Gyeongsang National University School of Medicine, 92, Chilam-dong, Jinju 660-751, Korea
Phone: 82-55-750-8684, Fax: 82-55-750-8618 E-mail: [email protected]
Received: Jun. 11, 2010 Accepted: Aug. 5, 2010
서 론
결핵은 전세계적 보건문제이며 한국에서의 유병률은 지속적으로 감소하고 있지만 아직도 서구 선진국에 비해
서 높은 상황이다1,2. 폐결핵은 타인에게 감염되는 것을 줄 이고 조직의 파괴성 병변이나 후유증의 발생을 예방하기 위해 조기진단이 중요하지만 확진을 위해서는 미생물학 적 균의 동정이 필요하다.
항산균 도말 염색검사는 간단한 방법으로 신속하게 결 과를 확인할 수 있지만 민감도가 낮고 결핵균과 비결핵성 항산균(nontuberculous mycobacteria, NTM)과의 감별이 안 되며, 결핵균 배양검사는 검체에 존재하는 결핵균이 아주 적어도 검출되는 장점이 있고 특이도도 높지만 결과 를 확인하는데 시간이 오래 걸리는 단점이 있다3.
도말 및 배양검사의 단점을 보완한 결핵균 중합효소연 쇄반응법(TB-PCR)은 검체 내에 소수의 균이 존재하더라 도 진단이 가능하고 신속한 결과를 얻을 수 있어 조기진단 에 널리 이용되고 있으며, 민감도와 특이도가 높아 결핵의 진단에 널리 사용하고 있다4,5. 하지만 위양성의 위험이 있 고, 최근 빈도가 증가되고 있는 NTM을 직접 검출하지 못 하는 단점이 있다6.
항산균 도말 양성의 호흡기 검체에서 NTM을 조기에 확인하는 것은 임상적으로 중요한데 그 이유는 폐결핵으 로 오인하여 치료하는 경우가 있고, 폐결핵과 치료 약제도 다르며 최근 그 빈도가 점점 증가하는 추세이기 때문이다.
미국의 경우 항산균 도말 양성인 호흡기 검체에서 NTM 의 빈도는 약 25∼30% 정도이고7, 국내에서도 10% 이상 차지하는 것으로 보고되고 있으며 과거에 비해 그 빈도는 점점 증가하는 추세이다8,9. 현재 임상에서는 항산균 도말 염색결과가 양성이고 TB-PCR이 음성인 경우에 NTM으로 추정하고 있다10-12.
실시간 중합효소연쇄반응법(real-time PCR)은 특정 유 전자의 증폭산물에 결합된 형광물질의 방출을 실시간으 로 분석하여 측정하는 방법으로 정량화 할 수 있고 중합효 소연쇄반응법 이후 전기영동과 같은 추가적인 과정이 필요 하지 않기 때문에 오염의 위험성을 낮출 수 있다. 또한 기 존 중합효소연쇄반응법에 비해 검사 시간을 단축할 수 있 으며 특이도를 높일 수 있는 다양한 장점을 가지고 있다13. 결핵균과 NTM을 동시에 진단할 수 있는 결핵균/비결핵 성항산균 실시간 중합효소연쇄반응법(TB/NTM real-time PCR)이 최근에 개발되고 상용화되면서 호흡기 검체에서 결 핵균의 검출률을 높이고 조기에 결핵균과 NTM을 감별할 수 있을 것으로 기대하고 있으며 그 유용성에 대한 보고가 국내에서도 발표되고 있다14-17. 본 연구는 객담 및 기관지세 척액과 같은 호흡기 검체에서 결핵균과 NTM 검출에 TB/NTM real-time PCR의 유용성을 알아보기 위한 것이다.
대상 및 방법
1. 대상 환자
2009년 1월부터 6월까지 객담 및 기관지세척액에서 TB/NTM real-time PCR을 시행하고 배양에서 결핵균 또 는 NTM이 동정된 80명(남자 54명, 여자 26명; 평균 나이 61.7세)을 대상으로 총 87예의 검체(객담 37예, 기관지세 척액 50예)를 후향적으로 분석하였다. 호흡기 검체에서 항산균 도말검사는 음성이면서 TB/NTM real-time PCR이
양성인 경우와 도말검사는 양성이면서 TB/NTM real-time PCR이 음성인 경우, 항산균 도말검사와 TB/NTM real- time PCR이 모두 음성 또는 양성인 경우를 조사하였다.
기존의 TB-PCR법과 비교하기 위해 2008년 3월부터 8월까 지 TB-PCR을 시행하고 객담 및 기관지세척액에서 결핵균 또는 NTM이 배양된 59명(남자 39명, 여자 20명; 평균나이 61.3세) 환자의 63예 검체(객담 19예, 기관지세척액 44예) 를 대상으로 후향적으로 같은 방법으로 분석하였다.
2. 검체의 처리와 항산균 도말 및 배양검사
검체와 동량의 4% NaOH를 섞고 실온에서 15분간 두었 다가 인산완충용액(0.067 M, pH 6.8) 2∼3배를 첨가하여 다시 섞어주었다. 검체를 4oC에서 4,000 rpm으로 20분간 원심분리한 후 침전물을 회수하여 검사를 시행하였다. 항 산균 도말은 Ziehl-Neelsen 염색법을 이용하여 미국질병 예방통제국의 기준에 따라 판독하였고3, 배양은 3% Oga- wa 한천 배지에 접종하고 37oC에서 최대 8주까지 배양하 였다. 배양 후 집락이 보이면 SD bioline TB Ag MPT64 Rapid (Standard Diagnostic Inc., Seoul, Korea)를 이용한 면역크로마토그래피 방법으로 결핵균과 NTM을 일차적으 로 구별하였다.
3. TB/NTM real-time PCR 방법
Real-QTM MTB&NTM Kit (Biosewoom Inc., Seoul, Korea)를 이용하여 제조사의 지침에 따라 시행하였다. 전 처리한 검체 1 mL을 원심분리하여 상층액을 제거한 다음 인산완충용액과 멸균된 증류수를 순서대로 첨가하여 각 각 원심분리를 한 다음 침전물을 얻었다. DNA 추출은 침 전물에 extraction buffer를 섞고, 56oC에서 약 15분간 보 관하고 간헐적으로 혼합한 뒤, 100oC에서 8분간 가열한 다음 원심분리하여 상층액 2.5 μL를 얻었다. PCR은 튜브 에 2×PCR mixture를 12.5 μL을 넣고, MTB와 NTM, Internal control (IC) primer/probe 혼합액을 넣은 다음 추출한 검체 DNA 2.5 μL를 첨가하고, Roter-GeneTM 3000/6000 (QIAGEN GmbH, Hilden, Germany)을 이용 하여 50oC 2분, 95oC 10분의 변성 단계 후 95oC 15초, 67oC 45초 동안 40주기로 시행하였다. 결과는 각각의 채 널에서 파장을 확인하여 CT 값을 구하고 35 미만인 경우 에 양성으로 판독하였다. MTB와 NTM을 구별하는 방법 은 MTB signal은 나오지 않고 mycobacterai genus-spe- cific signal만 나오는 경우에 NTM으로 추정하였다.
Table 1. Detection rate of MTB and NTM in TB/NTM re- al-time PCR
Culture result
PCR positive for PCR negative (%) Total MTB (%) NTM (%)
M. tuberculosis 58
AFB stain (-) 22 (71) - 9 (29) 31 AFB stain (+) 25 (92.6) - 2 (7.4) 27
NTM 29
AFB stain (-) - 2 (11.1) 16 (88.9) 18 AFB stain (+) - 8 (72.7) 3 (27.3) 11 MTB: Mycobacterium tuberculosis ; NTM: nontuberculous myco- bacterium; AFB: acid fast bacilli; PCR: polymerase chain re- action.
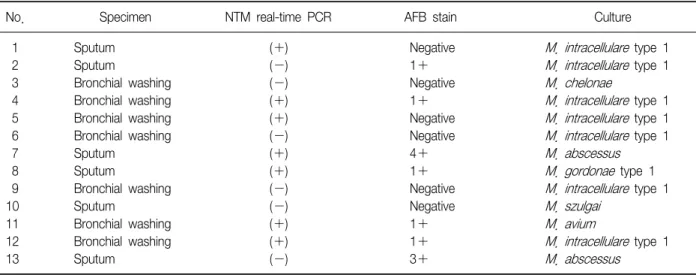
Table 2. Results of cases of cultured NTM
No. Specimen NTM real-time PCR AFB stain Culture
1 Sputum (+) Negative M. intracellulare type 1
2 Sputum (-) 1+ M. intracellulare type 1
3 Bronchial washing (-) Negative M. chelonae
4 Bronchial washing (+) 1+ M. intracellulare type 1
5 Bronchial washing (+) Negative M. intracellulare type 1
6 Bronchial washing (-) Negative M. intracellulare type 1
7 Sputum (+) 4+ M. abscessus
8 Sputum (+) 1+ M. gordonae type 1
9 Bronchial washing (-) Negative M. intracellulare type 1
10 Sputum (-) Negative M. szulgai
11 Bronchial washing (+) 1+ M. avium
12 Bronchial washing (+) 1+ M. intracellulare type 1
13 Sputum (-) 3+ M. abscessus
NTM: nontuberculous mycobacterium; AFB: acid fast bacilli; PCR: polymerase chain reaction.
4. TB-PCR 방법
ABSOLUTETM MTB II PCR Kit (Biosewoom Inc.)를 이용하여 제조사의 지침에 따라 시행하였다. 전처리와 DNA 추출은 real-time PCR과 동일한 방법으로 실시하였 다. PCR은 튜브에 1차 PCR 혼합물를 15 μL, 1차 PCR 효소를 0.5 μL 넣고 추출한 검체 DNA 4.5 μL를 첨가하 였다. Roter-GeneTM 3000/6000을 이용하여 95oC 5분의 변 성 단계 후 94oC 30초, 68oC 30초, 72oC 30초의 PCR 주기 로 35회 한 후 72oC 5분 동안 시행하였다. 1차 PCR이 끝 난 후 튜브에 2차 PCR 혼합물을 18 μL, 1 차 PCR 효소 0.5 μL와 1차 산물 1.5 μL를 첨가한 다음 Roter-GeneTM
3000/6000을 이용하여 95oC 5분의 변성 단계 후 94oC 30 초, 65oC 30초, 72oC 30초의 PCR 주기로 25회 한 후 72oC 5분 동안 시행하였다. PCR 반응 후 반응물 7 μL를 2%
아가로스 젤에 전기영동하여 PCR 산물의 크기를 확인하 였다. 230 bp와 473 bp가 나오거나 혹은 230 bp 밴드만 나올 경우 결핵균으로 판정하였다.
5. 통계 처리
SPSS version 12.0 (SPSS Inc., Chicago, IL, USA) 프로 그램을 이용하였다. 검사간의 민감도 비교는 교차분석을 통하여 chi-sqaure test를 시행하였으며, p값이 0.05 이하 인 경우 의미 있는 것으로 판단하였다.
결 과
TB/NTM real-time PCR을 시행한 검체에서 결핵균과 NTM이 배양된 경우는 각각 58예, 29예이었다. 결핵균이 배양된 58예 중에서 47예(81%)가 TB real-time PCR 양성 이었고, NTM이 배양된 29예 중에서 NTM real-time PCR 이 양성인 경우는 10예(34.4%)이었다. 도말음성이고 결핵 균이 배양된 31예에서 TB real-time PCR 양성은 22예 (71%), 음성은 9예(29%)이었으며, 도말양성 27예 중에서 TB real-time PCR 양성은 25예(92.6%), 음성은 2예(7.4%) 이었다(Table 1). NTM이 배양된 29예 중에서 도말음성은 18예이었고 이 중 NTM real-time PCR 양성은 2예(11.1%), 음성은 16예(88.9%)이었고, 도말양성 11예 중에서 NTM
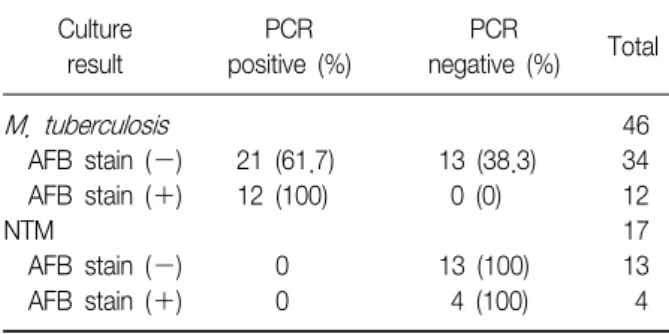
Table 3. Detection rate of MTB and NTM in TB-PCR
Culture
result
PCR positive (%)
PCR
negative (%) Total
M. tuberculosis 46
AFB stain (-) 21 (61.7) 13 (38.3) 34 AFB stain (+) 12 (100) 0 (0) 12
NTM 17
AFB stain (-) 0 13 (100) 13
AFB stain (+) 0 4 (100) 4
MTB: Mycobacterium tuberculosis ; NTM: nontuberculous myco- bacterium; AFB: acid fast stain; PCR: polymerase chain reaction.
real-time PCR 양성은 8예(72.7%), 음성은 3예(27.3%)이 었다(Table 1). NTM이 배양된 29예 중에서 균동정을 의 뢰하여 확인한 예는 Table 2와 같다.
TB-PCR 검사를 시행한 검체에서 결핵균이 배양된 경우 는 46예이었고 도말검사 음성은 34예, 양성은 12예이었 다. 도말음성인 34예 중에서 TB-PCR 양성은 21예 (61.7%), 음성은 13예(38.3%)이었고 도말양성인 12예는 TB-PCR이 모두 양성이었다. NTM이 배양된 17예는 TB- PCR이 모두 음성이었고, 항산균 도말검사가 양성으로 나 와 NTM으로 간주한 경우는 4예이었고(Table 3)
Myco- bacterium abscessus
가 2예,M. gordonae
과M. intra- cellular
e가 각각 1예이었다.고 찰
폐결핵과 NTM에 의한 폐질환은 임상증상이나 방사선 소견으로 감별하기 쉽지 않기 때문에 실제 임상에서는 항 산균 도말검사가 양성으로 나와 폐결핵으로 치료하다가 배양에서 NTM이 동정되어 약제를 변경하거나 중단하는 경우를 흔히 보게 된다18. 항산균 배양 양성의 검체에서 NTM의 검출률은 점점 증가하는 추세인데8,9, 본 연구에서 도 배양 양성 검체에서는 30% (46/150예)이었고, 도말양 성의 경우에는 24.4% (12/49예)를 차지하였다. 이런 점으 로 볼 때 항산균 도말이 양성이 나와도 NTM의 가능성을 항상 염두에 두어야 하며 적절한 치료와 방침을 결정하기 위해 조기 감별이 중요하다고 할 수 있다. 현재 임상에서 는 항산균 도말검사가 양성이면서 TB-PCR이 음성이면 NTM으로 간주하고 임상 결정에 유용한 것으로 보고되고
있지만10,11, 최근 상용화된 TB/NTM real-time PCR 검사는
호흡기 검체에서 결핵균과 NTM을 직접 감별하고 검출률
도 올릴 수 있을 것으로 기대된다.
본 연구의 결과로 보면 TB/NTM real-time PCR 검사는 도말음성 보다는 도말양성 검체에서 결핵균과 NTM을 감 별하는데 더 유용할 것으로 생각된다. NTM이 배양된 검 체에서 도말양성의 경우 real-time PCR 양성률은 72.7%
(8/11예)이었지만, 도말음성의 경우는 11.1% (2/18예)로 도말양성 검체에 비해 상대적으로 매우 낮은 양성률을 보 였다. Chang 등17의 보고에서도 도말음성 검체 8예 중에 서 1예에서만 NTM real-time PCR이 양성으로 나왔고, Kim 등15은 6예의 도말음성 검체에서 3예가 NTM re- al-time PCR 양성으로 보고하고 있다. 본 연구와 국내의 연구결과를 보면 도말음성 검체에서 NTM에 대한 re- al-time PCR의 민감도는 낮은 것으로 생각된다.
TB/NTM real-time PCR 검사는 본 연구에서 결핵균을 진단하는 데도 높은 민감도를 보였다. 도말양성 검체에서 TB real-time PCR은 92.6% (25/27예)의 양성률을 보였고 도말음성 검체에서도 71% (22/31예)의 양성률을 보였는 데 이것은 TB-PCR 검사를 시행한 도말음성 검체에서의 양성률 61.7% (13/21예) 보다 높은 것이다(p<0.05). Kim 등15의 보고에서도 본 연구와 비슷한 70% 정도의 양성률을 보였다. 본 연구의 결과로 보면 결핵균 검출에 대한 re- al-time PCR 민감도도 기존의 TB-PCR 만큼 우수할 것으로 생각되지만 두 검사 간의 민감도를 비교하기 위해서는 동 일한 검체를 이용한 검사가 필요할 것으로 생각된다.
본 연구에서 사용한 ABSOLUTETM MTB II PCR 키트는 nested PCR 방법으로 1차 PCR 산물의 특정한 부위를 2차 PCR로 다시 증폭하여 전기영동에 의해 균의 유무를 확인 하는 방법으로 기존의 PCR법에 비해 오염의 위험도는 높 지만 민감도를 향상시킨 검사법이다. 객담이나 기관지세 척액과 같은 호흡기 검체에서 도말음성인 경우에 결핵 진 단을 위한 TB-PCR 검사의 민감도는 연구자마다 차이가 있지만 약 40∼60% 정도로 보고되고 있으며19-21, 국내의 연구22도 비슷한 민감도를 보고하고 있고 본 연구에서는 검체 수가 충분하지 않지만 약 60% 정도로 비교적 높은 양성률을 보였다.
일반적으로 도말양성이지만 TB-PCR이 음성인 경우에 NTM을 의심할 수 있고 임상적으로 유용한 것으로 보고되 고 있는데10-12, 본 연구에서도 도말양성이지만 TB-PCR이 음성으로 나온 4예에서 모두 NTM이 배양되었고, 도말음 성이지만 전기영동에서 결핵균과는 다른 양상을 보여 NTM으로 보고된 경우가 3예가 있었다. 결과에는 기술되 지는 않았지만 TB-PCR이 양성으로 나와 결핵으로 간주하
였으나 배양에서는
Mycobacterium
spp.로 나온 경우가 1예가 있었으며 이것은 PCR에서 MTB와 NTM 밴드가 동 시에 나오는 경우에 MTB로 판정을 내리게 되므로 배양에 서는 NTM이 배양될 수 있을 것으로 생각된다.본 연구에서는 도말 양성인 검체에서 TB real-time PCR 이 음성인 경우가 27예 중에서 2예로 위음성률이 7.4%로 나왔으며, Chang 등17의 보고에서도 1예에서 위음성을 보 고하였지만 Kim 등15의 연구에서는 82예의 도말양성 검체 모두가 real-time PCR이 양성으로 나온 것으로 보고하고 있다. TB-PCR에서는 위음성으로 나온 경우는 본 연구에 서 관찰되지 않았는데 결핵균에 대한 real-time PCR과 TB-PCR의 민감도와 특이도는 Jung 등16의 보고에 의하면 각각 86∼93% 정도로 비슷한 수준을 보이는 것으로 보고 하고 있다.
결론적으로 TB/NTM real-time PCR은 항산균 도말양성 의 호흡기 검체에서 결핵균과 NTM을 감별하는데 유용하 며, 결핵균의 검출에도 기존 TB-PCR만큼 우수한 것으로 판단된다.
참 고 문 헌
1. Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC.
Consensus statement. Global burden of tuberculosis:
estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA 1999;282:677-86.
2. Kim HJ. Current situation of tuberculosis and its control in Korea. J Korean Med Assoc 2006;49:762-72.
3. Diagnostic Standards and Classification of Tuberculosis in Adults and Children. This official statement of the American Thoracic Society and the Centers for Disease Control and Prevention was adopted by the ATS Board of Directors, July 1999. This statement was endorsed by the Council of the Infectious Disease Society of America, September 1999. Am J Respir Crit Care Med 2000;161:1376-95.
4. Cousins DV, Wilton SD, Francis BR, Gow BL. Use of polymerase chain reaction for rapid diagnosis of tuberculosis. J Clin Microbiol 1992;30:255-8.
5. Park SS, Kwak KR, Hwang JY, Yun SM, Ryue CC, Chang CH, et al. Clinical utility of amplified mycobacte- rium tuberculosis direct test in the diagnosis of pulmo- nary tuberculosis. Tuberc Respir Dis 1999;47:747-56.
6. Balasingham SV, Davidsen T, Szpinda I, Frye SA, Tønjum T. Molecular diagnostics in tuberculosis: basis
and implications for therapy. Mol Diagn Ther 2009;13:
137-51.
7. Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA state- ment: diagnosis, treatment, and prevention of non- tuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007;175:367-416.
8. Lee JY, Choi HJ, Lee H, Joung EY, Huh JW, Oh YM, et al. Recovery rate and characteristics of nontuber- culous mycobacterial isolates in a university hospital in Korea. Tuberc Respir Dis 2005;58:385-91.
9. Koh WJ, Kwon OJ, Yu CM, Jeon KM, Suh GY, Chung MP, et al. Recovery rate of nontuberculous mycobac- teria from acid-fast-bacilli smear-positive sputum speci- mens. Tuberc Respir Dis 2003;54:22-32.
10. Lee JS, Ji HS, Hong SB, Oh YM, Lim CM, Lee SD, et al. Clinical utility of polymerase chain reaction for the differentiation of nontuberculous mycobacteria in pa- tients with acid-fast bacilli smear-positive specimens.
Tuberc Respir Dis 2005;58:452-8.
11. Yu CM, Koh WJ, Ryu YJ, Jeon K, Choi JC, Kang EH, et al. Usefulness of PCR test for M. tuberculosis for the differentiation of pulmonary tuberculosis and non- tuberculous mycobacterial lung disease in patients with smear-positive sputum. Tuberc Respir Dis 2004;57:
528-34.
12. Kim CS, Son HD, Park MR, Seo JY, Cho DI, Rheu NS.
Usefulness of PCR study in AFB smear negative patients on admission. Tuberc Respir Dis 1997;44:1001-10.
13. Lee MK. Real-time polymerase chain reaction (PCR) in microbiology. Infect Chemother 2004;36:105-13.
14. Lee SD, Lee HY, Kim HC, Kim SY. Mycobacterium tu- berculosis and nontuberculous mycobacteria by PCR assay. Korean J Clin Microbiol 2007;10:135-42.
15. Kim YJ, Park MY, Kim SY, Cho SA, Hwang SH, Kim HH, et al. Evaluation of the performances of AdvanSure TB/NTM real time PCR kit for detection of mycobacteria in respiratory specimens. Korean J Lab Med 2008;28:
34-8.
16. Jung CL, Kim MK, Seo DC, Lee MA. Clinical usefulness of real-time PCR and amplicor MTB PCR assays for di- agnosis of tuberculosis. Korean J Clin Microbiol 2008;
11:29-33.
17. Chang HE, Heo SR, Yoo KC, Song SH, Kim SH, Kim HB, et al. Detection of mycobacterium tuberculosis complex using real-time polymerase chain reaction.
Korean J Lab Med 2008;28:103-8.
18. Koh WJ, Kwon OJ. Diagnosis and treatment of non- tuberculous mycobacterial lung disease. Korean J Med
2008;74:120-31.
19. Wobeser WL, Krajden M, Conly J, Simpson H, Yim B, D'costa M, et al. Evaluation of Roche Amplicor PCR as- say for Mycobacterium tuberculosis. J Clin Microbiol 1996;34:134-9.
20. Bergmann JS, Woods GL. Clinical evaluation of the Roche AMPLICOR PCR Mycobacterium tuberculosis test for detection of M. tuberculosis in respiratory speci- mens. J Clin Microbiol 1996;34:1083-5.
21. Mo EK, Kyung TY, Kim DG, Park MJ, Lee MG, Hyun IG, et al. The clinical utility of polymerase chain re- action in the bronchoalveolar lavage fluid for the de- tection of mycobacteria. Tuberc Respir Dis 1998;45:
519-28.
22. Baek SH, Lee JM, Kang MJ, Son JW, Lee SJ, Kim DG, et al. How reliable is sputum PCR test in the diagnosis of pulmonary tuberculosis when sputum smear is neg- ative? Tuberc Respir Dis 2001;50:222-8.