급성심근경색증으로
5
0
0
전체 글
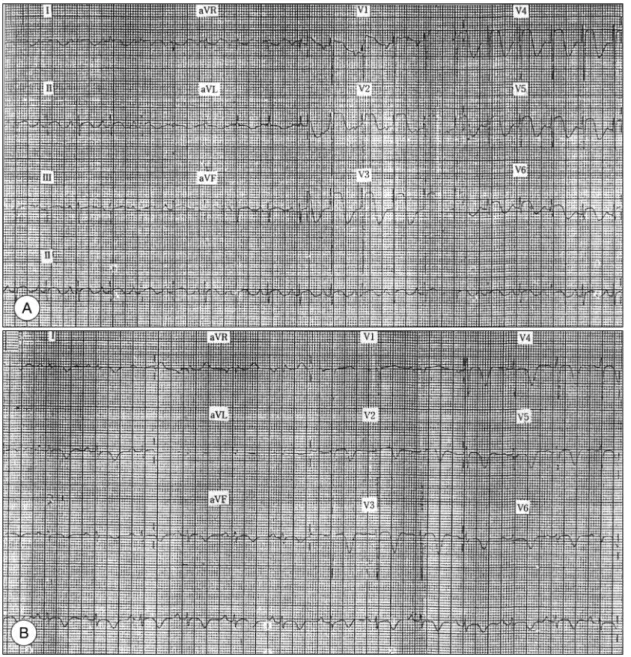
(2) 로 상승되어 있었으며, 심초음파도에서 전벽, 심첨부. 콜라민을 분비하는 갈색세포종을 생각할 수 있었다. 입. 및 심중격부에 국소벽 운동장애(RWMA)를 보였다. 급. 원 3일째 시행한 심초음파도에서는 심첨부에 혈전이. 성 심근경색증 의심하에 관동맥 스텐팅 목적으로 관동. 관찰되어었고 심첨부외의 국소벽 운동장애(RWMA)는. 맥조영술을 실시하였으나 정상 관동맥 소견을 보였다. 소실되었다(Fig. 3).. (Fig. 2). 급성 심근경색증의 병인을 찾던 중, 평소 갑. 검사실 소견:공복시 혈당은 133 mg/dL였으며, 소. 작스럽게 발생하는 심계항진과 발한을 경험하였던 기. 변 검사에서 당은 3+로 검출되었다. 갈색세포종을 의. 왕력이 있었고, 안저검사에서 Keith-Wagner class Ⅲ. 심하고 검사한 혈액 및 소변내 카테콜라민 및 대사산물. 의 고혈압성 망막증과 심초음파도에서 대칭성의 심근. 의 농도는 상승되어 있었다(Table 1).. 비대를 보이고 있어 이차성 고혈압의 원인으로서 카테. 방사선학적 소견:복부 MRI를 시행한 결과 주위로. Fig. 1. Serial electrocardiograms evolution of extensive anterior wall myocardial infarction. (A) At the first admission, (B) After theraphy of α-blocker during 3 weeks.. 307.
(3) Fig. 2. Coronary angiogram revealed normal coronary arteries. Table 1. Catecholamine and it's metabolites level At admission. Postop. Normal. Serum catecholamine (Epi, NE). 505.9 / 5257.9. 66.9 / 223.7. 0-120/100-410 pg/ml. 24hr urine catecholamine. 158.2 / 133.8. 15.8 / 24.88. 0- 40 / 0-80 μg/day. 24hr urine VMA 24hr urine metanephrine. 28.35 4455. 8. 4.87 108. 2-10 mg/day 52-341 μg/day. Fig. 3. Follow-up echocardiogram revealed a thrombus in the left ventricualr lumen at the 3rd hospital day.. 의 침습은 보이지 않는 6×6×5 cm 크기의 부신내 종 괴가 발견되었다(Fig. 4). 131-MIBG(metaiodoben-. Fig. 4. Abdominal MRI shows a round, well-demarcated mass with irregular central necrosis.. zylguanethidine) 스캔에서 부신외 전이는 없는 것으 로 확인되었고, 다발성내분비종양에 대한 검사로 갑상. 괴를 제거하였다. 절단면은 회갈색을 띄며 중심부에 출. 선 초음파를 시행하였으나 정상이었다.. 혈소견을 동반하였고, 현미경 소견에서는 섬유혈관성. 수술 및 병리소견:우측 늑골하 절개후 후복강내에. 조직들로 둘러싸인 주(chief)세포들의 덩어리와 혈관조. 서 4×4 cm 크기의 적갈색의 피막에 잘 싸여있는 종. 직의 증식이 관찰되었다. 종양세포들의 핵은 다양한 모. 308. Korean Circulation J 1999;29(3):306-310.
(4) A. B. Fig. 5. (A) Rounded nests of chief cells circumscribed by fibrovascular network. The vascular proliferation is particularly prominent in this example. Large polygonal tumor cells have nuclear pleomorphism and eosinophilic granular cytoplasm (H&E stain, 400×). (B) Immunohistochemical pattern of pheochromocytoma. Chief cells are positive for chromogranin (400×).. 양을 띄며 핵내에 가성 봉입체(pseudoinclusion)을 가. 경우에서도 3주간 α-차단제를 사용였음에도 T파의. 지고 있고, 세포질은 호산성의 과립상을 띄었다. 면역염. 역위는 남아 있었고(Fig. 1B), 수술후에도 지속되었다.. 색에서 종양세포들은 chromogranin과 synaptophysin. 갈색세포종에서 이러한 심전도상의 변화가 나타나는. 에 양성을 보였고, 지지세포들은 S-100에 양성이었다. 병인에 대한 연구가 있었다. 1983년 McGolnigle 등15). (Fig. 5).. 은 흉통이나 심근경색증을 경험한 환자에서 보이는. 수술 후 경과:수술후 갈색세포종이 확진되었고, 혈. ST 분절의 상승을 관상동맥의 연축에 의한다고 제시. 압 상승 및 심계항진은 호전되었으며 내당능 장애 및. 하였고, 1986년 Goldbaum 등7)이 이형 협심증 환자에. 뇨당 검출은 정상화되어 현재 외래 추적 관찰 중이다.. 서 임상적으로 관찰한 바에 의하면 α교감신경 자극과 β교감신경 차단이 갈색세포종 환자들과 같은 감수성. 고. 찰. 있는 환자에서 관상동맥의 연축을 유발하거나 촉진한 다고 제시하고 있다. 그러나, 카테콜라민과 관상동맥의. 갈색세포종에서 분비되는 카테콜라민과 관련된 심전. 연축과의 관계는 아직 정확히 이해되지 않고 있다.. 도의 변화들과 협심증, 심근경색증, 심근증 및 심부전. 임상적으로 갈색세포종 환자는 반수 이상에서 지속. 증 등의 심혈관계 증상들에 대한 여러 보고들이 있었지. 적인 고혈압을 보이지만 주기적인 혈압변동 및 고혈압. 만, 갈색세포종과 관련된 급성심근경색증의 실제 빈도. 의 돌연발작을 보이기도 하고, 10%정도에서는 정상 혈. 및 병인에 대해 정확히 알려진 바는 없다.1-9). 압을 보이기 때문에 주의를 해야 한다.16) 한편 지속적. 본 환자는 심전도에서 특징적으로 V1에서 V6에 이 르는 흉부유도에 ST 분절의 상승을 보이고 있었는데, 문헌들을 볼 때 갈색세포종 환자의 75%정도에서 심전 10). 도의 이상을 보인다고 하였다.. 으로 상승된 카테콜라민에 의해 탈감작상태가 되면 기 립성 저혈압이 오기도 한다. 그리고, 본 증례에서는 평소 고혈압을 진단받지 못했. 주로 T파의 역위와. 지만 초음파에서 대칭성의 좌심실 비대가 저명하였는. 좌심실 비대 및 동성빈맥을 보이며, 방실전도의 변동으. 데, 1986년 Clarence 등17)이 갈색세포종을 가진 26명. 로 P-R간격이 짧아지거나 QRS간격이 좁아진다고 하. 의 환자를 대상으로 한 연구보고에 따르면 갈색세포종. 였고, 심근이 손상되게 되면 ST분절의 변화 및 전반적. 환자에서 가장 흔한 심초음파에서의 특징은 정상 또는. 인 T파의 역위을 볼수 있다고도 하였다.7)11-14) 이러한. 증가된 심실 수축력을 보이는 정상 좌심실이었다. 좌심. 심전도의 변화는 종양을 제거하거나 약물로 차단했을. 실 비대를 보이는 경우는 대부분 대칭적으로 심실벽이. 때 사라지지만, 고혈압이 오랫동안 있었던 경우는 심전. 두꺼워져있으며, 이들도 심실기능은 정상이거나 약간. 도 변화가 지속될 수도 있다고 하였다.11-13) 본 증례의. 감소되어 있었고, 최근 발생한 하측벽의 심근경색증 환 309.
(5) 자에서만 심실기능이 저하되어 있었다. 그리고, 심전도. 7) Goldbaum TS, Henochowicz S, Mustafa M. Pheochro-. 에서 좌심실비대를 보였을지라도 6명의 환자 가운데서 5명은 정상 초음파소견을 보였다. 또 심증상이 없거나. 8). 심장을 침범한 다른 임상적 증거가 없는 경우는 심초음 파에서 대개 정상이었다고 하였다. 갈색세포종은 고혈압 환자의 0.1% 미만에서 나타나 는 드문 질환으로서 이와 관련되어 급성 심근경색증이 발현되는 경우는 극히 적지만, 본 증례의 환자처럼 젊. 9) 10). 은 연령에 위험인자가 없으면서 급성 심근경색증이 발 생한 경우 카테콜라민을 분비하는 갈색세포종을 고려. 11). 해 볼 필요가 있다고 생각되어 보고하는 바이다.. 중심 단어:급성심근경색증・갈색세포증. REFERENCES. 12) 13). 1) Priest WM. Pheochromocytoma with fatal myocardial infarction in a man aged 22. Brit M J 1952;2:860.. 2) Roseman MD. Painless myocardial infarction: A review 3) 4) 5) 6). of the literature and analysis of 220 cases. Ann Int Med 1954;41:1-8. Bravo EL, Gifford RW. Pheochromocytoma: Diagnosis, localization and management. N Engl J Med 1984;311: 1298-1303. Northfield TC. Cardiac complications of pheochromocytomas. Br Heart J 1967;29:588-93. Boldt MH, Flexner M, Ortner AB. Pheochrocytoma associated with painless myocardial infarction. Ann Int Med 1957;46:1165-77. Mattman PE. Successful removal of a pheochromacytoma four weeks after acute myocardial infarction. Am J Cardiol 1961;8:426-30.. 310. 14). 15) 16). 17). mocytoma presenting with prinzmetal’s angina. Am J Med 1986;81:921-2. Serfas D, Shoback DM, Lorrell BH. Pheochromocytoma and hypertrophic cardiomyopathy: Apparent supression of symptoms and noradrenaline secretion by calciumchannel blokade. Lancet 1983;24:711-3. Sardesai SH, Marinde AJ, Sivathandon Y. Pheochromocytoma and catecholamine-induced cardiomyopathy presenting as heart failure. Br Heart J 1990;63:234-7. Surawicz B, Mangiardi ML. Electrocardiogram in endocrine and metabolic disorders. In Rios JG (eds): Clinical Electrocardiographic Correlations. Philadelphia FA Davis Co;1977. p.243. Sayer WJ, Moser M, Mattingly TW. Pheochrocytoma and the abnormal electrocardiogram Am Heart J 1954; 43:42-53. Cheng TO, Bashour TT. Striking electrocardiographic changes associated with pheochromacytoma. Chest 1976; 70:397-9. Strenson G, Swedbeg K. QRS amplitudes, QT intervals, and ECG abnormalities in pheochromocytoma patients before, during and after treatment. Acta Med Scand 1988; 224:231-5. Jung TH, Jang JK, Jung HS, Kim SK, An JW, Jang KH, et al. A case of pheochromocytoma with electrocardiographic change mimicking angina pectoris, and hypotensive crises. Korean J Med. 1993;45:801-7. McGonigle P, Webb SW, Adgoy AA. Pheochromocytoma: An unusual cause of chest pain. Br Med J 1983;286:1477-8. Braunwald E. Heart disease: A textbook of cardiovascular medicine. In: Williams GH, Lilly LS, Seely EW. The Heart in Endocrine and Nutritional Disorders. 5th ed. WB Saunders Co;1997. p1897-9. Shub C, Cueto-Garcia L, Sheps SG. E chocardiographic findings in pheochromocytoma. Am J cardiol 1986;57:971-5.. Korean Circulation J 1999;29(3):306-310.
(6)
수치

관련 문서
In addition, I compared Kim Ki-Su 'Arirang' music score and current middle school music textbooks 'Arirang' score, which were presented at the National
Seung Soo Jang Sung Gyun Shin Min Jae Lee Sang Soo Han Chan Ho Choi Sungkyum Kim Woo Sung Cho and Song Hyun Kim POSTECH Yeong Rok Kang Wol Soon Jo Soo Kyung Jeong and
Therefore, cTnT is a recommended biomarker for use in the detection of myocardial infarction (MI) and in acute coronary syndromes.[8] Indeed, several authors
Chang Goo Kang, Ah Hyun Park, Jang Ho Ha, Young Soo Kim, Joon-Ho Oh, Jeong Min Park, Soo Mee Kim, Seung-Jae Lee, Seung Hee Lee, and Han Soo Kim(KAERI). Fabrication
Approved clinical use of bone marrow stem cells for myocardial infarction treatment... Cardiac
Chang Je Park, Kwoen Ho Kang, Sang Ho Na, Young Hee Kim, Ho Jin Ryu, Geun Il Park, and Kee Chan Song (KAERI). Geun-Suk Choi and
IL Soon Hwang, Myung Hyun Kim, Han Gyu Joo, Kyung Woo Yi, Bong Yoo, Moo Hwan Kim, Seung Rok Oh, Yoon Jae Kim, Jong Gye Shin, Kwang Myung Lee, Jae Yong
컴퓨터 이용 설계 및 제작 Moon Ki, Jung..
