http://crossmark.crossref.org/dialog/?doi=10.14474/ptrs.2019.8.2.112&domain=pdf&date_stamp=2019-6-25
Received: 21 March, 2019 Revised: 7 May, 2019 Accepted: 21 May, 2019
Corresponding author: Sung-Hyoun Cho (ORCID https://orcid.org/0000-0002-5108-4342)
Department of Physical Therapy, Nambu University, 23 Cheomdanjungang-ro, Gwangsan-gu, Gwangju 62271, Republic of Korea Tel: 82-62-970-0232 Fax: 82-62-970-0492 E-mail: geriatricpt1@gmail.com
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2019 Korean Academy of Physical Therapy Rehabilitation Science
https://doi.org/10.14474/ptrs.2019.8.2.112 pISSN 2287-7576
eISSN 2287-7584
Phys Ther Rehabil Sci 2019, 8 (2), 112-123 www.jptrs.org
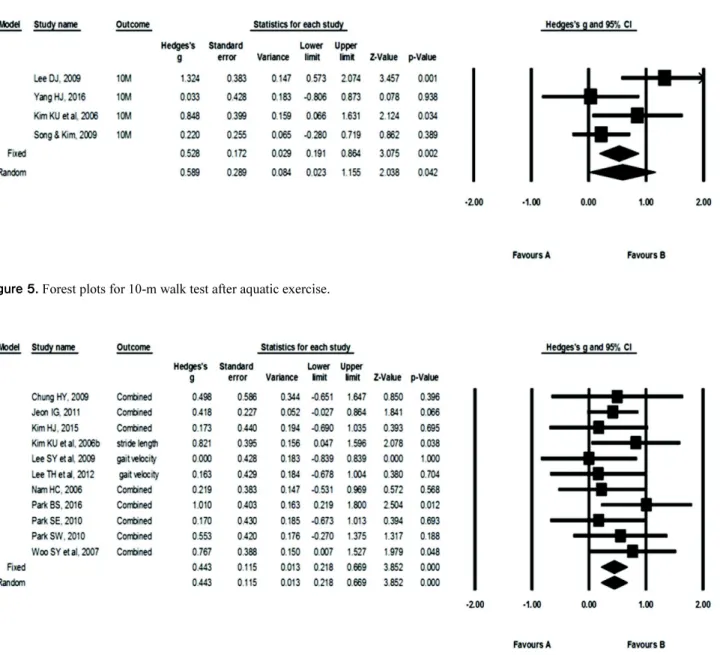
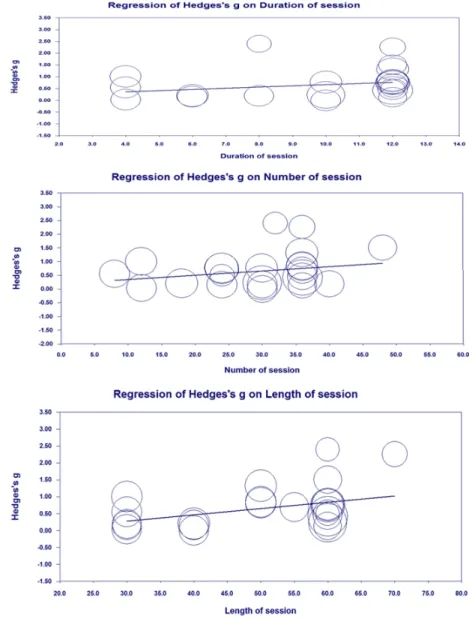
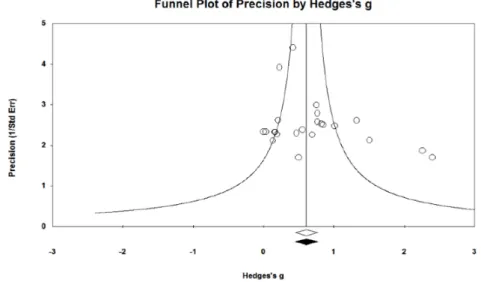
Effect of aquatic exercise on gait in persons with chronic stroke: a meta-analysis study in Korea
Dong-Jin Lee a , Sung-Hyoun Cho b
a
Department of Physical Therapy, Gwangju Health University, Gwangju, Republic of Korea
b