http://crossmark.crossref.org/dialog/?doi=10.14474/ptrs.2020.9.1.25&domain=pdf&date_stamp=2020-03-25
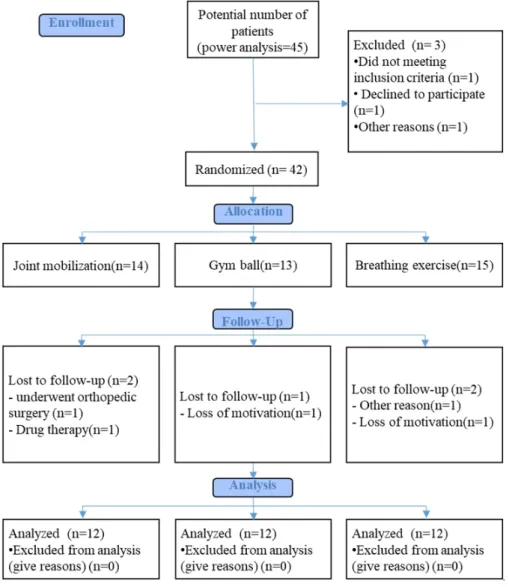
Comparison of the effects of joint mobilization, gym ball exercises, and breathing exercises on breathing pattern disorders and joint position sense in persons with chronic low back pain
11
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
수치

+3

관련 문서
The purpose of this study is to analyze the effects of sports marketing strategy fit on organizational attitude and organizational citizenship behavior
The purpose of this study was to investigate the impact of social capital and positive psychology capital on the will of start-up according to experience
The purpose and necessity of this study was to investigate the effect of the 8-week GX complex exercise program on the stress index, blood lipid and APG
The purpose of this study was to investigate how the BOSU Ball exercise, which can develop core muscles in middle-aged women, affects body composition and
The purpose of this study was to examine the parents' perceptions on the current status, effects and satisfaction of personal assistant service for students
The purpose of this study was to provide primary material in discussing methods to activate the treatment effects of diabetes and reduce the rate of
The torque analysis was performed acting on the joint of robot by modeling the kinematics and dynamics of the robot.. Load torque of the joint
The purpose and necessity of this study was to investigate the effects of lactic acid fatigue and body oxidation through myofascial relaxation exercise using small tools
