* Department of Dentistry, St. Mary’s Hospital, The Catholic University of Korea
** Department of Orthodontics, The Institute of Oral Health & Science, Samsung Medical Center, SungKyunKwan University School of Medicine
Abstract
The advent of implants has dramatically changed our view of the complete denture, single tooth replacement, and full-mouth fixed restoration. However, no surveys have been conducted regarding patient satisfaction with dental implant treatment in the distal extension missing areas. This study examined patient satisfaction with implant- supported fixed prostheses and conventional removable partial dentures (RPDs) in the distal extension missing areas.
Forty-two subjects with implant-supported fixed prostheses and 37 subjects with conventional RPDs were identified and included in the study. Patients rated their overall satisfaction and other features of their prostheses (comfort, esthetics, chewing ability, speech, stability, oral hygiene, treatment experience, treatment fee, treatment period and visit frequency, and self-confidence) on 100 mm visual analogue scales(VAS) over 2 months after delivery. Subjects in both groups were asked of a questionnaire consisting of 41 items focused on various clinical factors related to treatment outcome, such as oral function and patient satisfaction.
Within the limitations of this study, the following results were drawn:
1. The implant group had a better overall satisfaction than the conventional RPD but there were no significant differences. The implant group had a significantly higher scores on comfort, esthetics, speech, stability, treatment experience, and self-confidence. The conventional RPD group had a better overall satisfaction than the implant in oral hygiene, treatment fee, treatment period and visit frequency, but no statistically significant differences were observed in oral hygiene, and treatment period and visit frequency.
2. In function period, the implant group had a higher satisfaction than the conventional RPD except for the period from 1 year to 2 year but in more than 2 years only, a statistically better satisfaction (Ρ=0.027).
3. In all missing areas, the implant group had a higher satisfaction than the conventional RPD, but in the mandible of Kennedy class 1 only, a statistically better satisfaction (Ρ=0.043).
4. The conventional RPD subjects who had experienced previous removable denture, had lower satisfaction and the implant subjects who had experienced previous removable denture, slightly higher satisfaction was found but notsignificantly different.
5. The variables that were of primary importance in the implant patient satisfaction were stability, treatment fee and self-confidence (Ρ<0.0001), and in the denture patient satisfaction, were comfort (Ρ<0.0001). In conclusion, the use of osseointegrated implants as abutments for fixed partial dentures can be a predictable restorative alternative for the distal extension missing areas.
K
Keeyy wwoorrddss:: satisfaction, implant, conventional removable partial denture, distal extension missing areas.
dentures in the distal extension missing areas
Ho Sang Lee*, Cheol Won Lee*, Young Ho Kim**
Introduction
M
ost dental clinicians have used removable prostheses for the restoration of the distal extension areas. Great majority of patients are satisfied with their removable partial dentures (RPDs). However, even if the RPDs are constructed according to all accepted criteria, some patients will still be dissatisfied (Burns et al, 1995). Common complaints associated with the distal extension RPDs are lack of stability, minimal retention, unesthetic appearance of clasps, and discomfort upon loading (Brudvik, 1999).The advent of endosseous implants has dramatically changed our view of the complete denture, single tooth replacement, and full-mouth fixed restoration. It is obvious that implants can make a major contribution to the success of RPD. Our successes in these areas, especially in the mandible, where chronic problems associated with loading the edentulous ridge have plagued the profession, have led to the consideration of obtaining implant support for RPD (Becker et al, 1999).
A report regarding the proceedings of the Toronto Symposium (1998) concluded that patient satisfaction outcome measures should be included in future implant success criteria, highlighting the importance of the patient perspective in clinical practice (Zarb &
Albrektsson, 1998). In most cases, no significant relationship was observed between patient opinions of their prostheses and clinical assessments.
Patient-based assessments of treatment outcomes have been reported for complete dentures (Garrett et al, 1996
; Nassif, 1978) Examples include the evaluation of
patient satisfaction with complete dentures and masticatory performance and patient assessment of the perceived benefit from using dental implants to improve support and retention of complete dentures (Humphris et al, 1995 ; Harle & Anderson, 1993).
No surveys have been conducted regarding patient satisfaction with dental implant treatment in the distal extension missing areas.
The purpose of this study is to compare the overall satisfaction of two types of treatments-implant- supported fixed prostheses and conventional removable partial dentures-in the distal extension missing areas and to compare (1) the satisfaction according to function period, (2) satisfaction according to missing areas, (3) satisfaction with the view of functional aspect, treatment experience, treatment fee, treatment period and visit frequency, and self-confidence, and (4) satisfaction along with previous removable denture experience. The influence of clinical variables, such as functional aspect, treatment experience, treatment fee, treatment period and visit frequency, and self- confidence on the overall satisfaction was also evaluated.
Materials & Methods
1. Study design
This study examined the satisfaction of patients treated with dental implants for the replacement in the distal extension areas and treatment- and patient-related factors. An instrument was developed in this project to
II
I
survey patients who had been treated with dental implants. This survey instrument (self-administrated questionnaire) and data abstracted from the corresponding patient dental records were utilized to assess patient satisfaction with dental implant treatment in the distal extension areas. Restoration with conventional removable partial denture(RPD) was used as a control.
2. Subjects selection
Eligible patients were chosen at random from the files of the Department of Dentistry, Uijongbu St. Mary's hospital, Catholic University of Korea (USH) during the period from 1995 to 2004. Then they were verified by dental record documentation in order to meet the inclusion criteria. All patients had been treated with at least two dental implants-supported prostheses in the distal extension areas or tissue borne RPDs. Those patients whose definitive restoration was completed and in function at that time of subject recruitment (May to August, 2004) were included in this study. All prostheses were over two months old. All implants were fixed prostheses and all RPDs were retained with clasps.
3. Questionnaire and record abstraction The subjects for this study were recruited by telephone or periodic follow-up. A self-administrated structured questionnaire was developed to serve as the instrument for this survey. Treatment providers were not involved in collecting the data but one dental hygienist provided assistance. This questionnaire consists of 41 items that cover 12 domains : demographic characteristics, overall
satisfaction, comfort, esthetics, chewing ability, speech, stability, oral hygiene, treatment experience, treatment fee, treatment period and visit frequency, self- confidence. The patients were asked to response to visual analogue scales(VAS) with regard to 11 domains.
The VAS used (Fig.1) was a 100 mm horizontal line representing a spectrum of feeling between extremes identified by endphrases that served to provide patients with meaningful limits to their feelings (Wakabayashi et al, 1998). The left end of the line represented unsatisfactory, and the right end, satisfactory. Patients rated their assessment by placing a mark across the line at a point corresponding to their feelings at that time.
The distance of the mark from the left end limit was measured and identified as the VAS score. A low score represents an unsatisfactory feeling and a high score a satisfactory one. The scores of maxillary and mandibular prostheses were separately filled out if both arches were restored.
4. Dental record data abstraction Data abstraction from dental records was conducted blind to the questionnaire data by one dentist uninvolved. The abstraction included information regarding dental and medical history, demographic data, and details about the dental implant treatment itself (eg, type of implant placed and whether a grafting procedure was performed).
5. Statistical analysis
The primary analyses focused on the estimation of differences of overall satisfaction between treatment groups on VAS scores. Additional analyses explored the
association between overall satisfaction and clinically related factors.
Demographic differences between implant and RPD group were compared by Fisher's exact test in age and monthly income and Chi-square test in gender, marital status and education level. If there were demographic differences between two groups, adjustments made for age, gender, marital status, education level, and monthly income based on analysis of covariance (ANCOVA).
Satisfaction comparisons between treatment groups were performed using independent t-test and ANCOVA. Within group comparisons, the satisfaction of treatment according to function period and missing areas was compared by one-way analysis of variance (ANOVA). Significance was accepted at 5% and expressed as P values and 95% confidence intervals for the difference in mean VAS scores within and between groups. Ratings of overall satisfaction on the VAS were used as the dependent variable, while VAS ratings of level of comfort, esthetics, chewing ability, speech, stability, oral hygiene, treatment experience, treatment fee, treatment period and visit frequency, self- confidence were the independent variables. Univariate regression analyses were performed to evaluate the individual effect of each independent variable on the overall satisfaction ratings. In addition, multiple
regression analyses were conducted to estimate the combined effect of all the explanatory variables factors on subject ratings of overall satisfaction. The software used in the statistics analysis was SAS version 8.1 (SAS, Cary, NC. USA) for windows.
Results
1. A total of 87 subjects responded to the questionnaires. Three subjects failed to complete all questions, two subjects treated with severe complications after bone graft in the implant group and three subjects did not wear their RPDs. They were excluded. Therefore, a total of 79 subjects were evaluated.
The mean age was 49.5 years (SD 14.0) in the implant group and 62.2 years (SD 8.8) in the conventional RPD (Table 1). Forty-five percent of the implant group was men and 55% was women. In the conventional RPD, 38% was men and 62% was women. Eighty-three percent of the implant group and 81% of the conventional RPD were currently married. In education level, 34% of the implant group and 3% of the
III
Fig. 1. Example of a 100 mm long visual analogue scale with its English translation. The VAS score is equal to the distance in mm from left extremity.
Are you satisfied with overall treatment result?
Unsatisfactory very satisfactory
conventional RPD had college education. Thirty-eight percent of the implant group and 14% of the conventional RPD had monthly income above 3,000,000 won ( ). There were statistically significant differences between two groups in age (P=0.0004) and education level (P=0.0003).
2. Satisfaction comparisons between groups
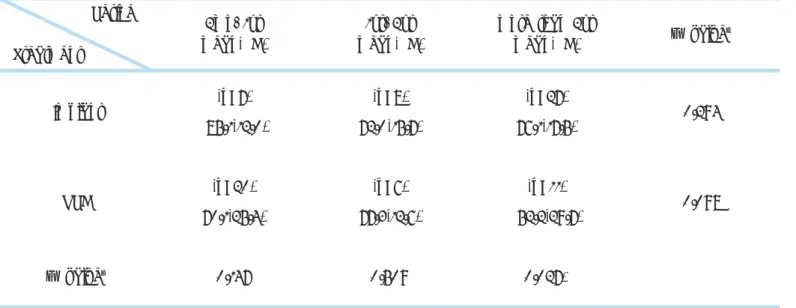
The implant group had a better overall satisfaction than the conventional RPD but was not significantly
different (Table 2). The implant group had a higher VAS scores on comfort, esthetics, chewing ability, speech, stability, treatment experience, and self- confidence. The conventional RPD group had a better overall satisfaction in oral hygiene, treatment fee, treatment period and visit frequency. However, no statistically significant differences were observed in chewing ability, oral hygiene, and treatment period and visit frequency.
In function period (Table 3), the implant group had a higher satisfaction than the conventional RPD except
Table 1. Demographic characteristics of study subjects Variable
Age†
≤35 36-45 46-55 56-65 65 Gender‡
male female Marital status‡
married other§
Education level‡
≤middle school high school
≥college Monthly income†
2,000,000
2,000,000-3,000,000 3,000,000-4,000,000
≥ 4,000,000
Implant (n=42) no(%) 7(16.7) 9(21.4) 8(19.1) 13(31.0)
5(11.9)
19(45.2) 23(54.8)
35(83.3) 7(16.7)
11(26.8) 16(39.0) 14(34.2)
18(45.0) 7(17.5) 8(20.0)
7(17.5)
RPD (n=37) no(%)
0(0) 0(0) 10(27.0) 17(46.0) 10(27.0)
14(37.8) 23(62.2)
30(81.1) 7(18.9)
24(64.9) 12(32.4) 1(2.7)
21(58.3) 10(27.8) 2(5.6) 3(8.3)
Ρ value
0.0004*
0.506
0.794
0.0003*
0.126
*Ρvalue was statistically significant (P<0.05)
†Fisher's exact test, ‡Chi-square test Single, divorced, or widowed.
Table 2. Satisfaction (VAS scores) in implant and RPD groups
Variable
Overall satisfaction† Comfort‡
Esthetics‡ Chewing ability‡ Speech‡
Stability‡ Oral hygiene‡
Treatment experience‡ Treatment fee‡
Treatment period and visit frequency‡ Self-confidence‡
Implant (n=42) mean(SD) 76.0(21.0) 78.8(13.1) 84.8(12.6) 77.6(19.1) 94.2(6.6) 89.4(22.7) 79.4(22.6) 83.8(14.7) 44.2(30.5) 49.4(30.0) 85.6(13.6)
RPD (n=37) mean(SD)
71.9(25.0) 68.7(17.1) 76.8(20.0) 70.4(23.3) 83.1(18.3) 75.7(21.9) 79.7(28.5) 72.2(13.0) 59.2(28.5) 54.8(26.1) 76.6(19.6)
Ρ value
0.452 0.004*
0.039*
0.132 0.001*
0.008*
0.949 0.0004*
0.028*
0.399 0.023*
*Ρvalue was statistically significant (P<0.05)
†Based on analysis of covariance (ANCOVA); adjustments made for age, gender, marital status, education level, monthly income
‡Independent t-test
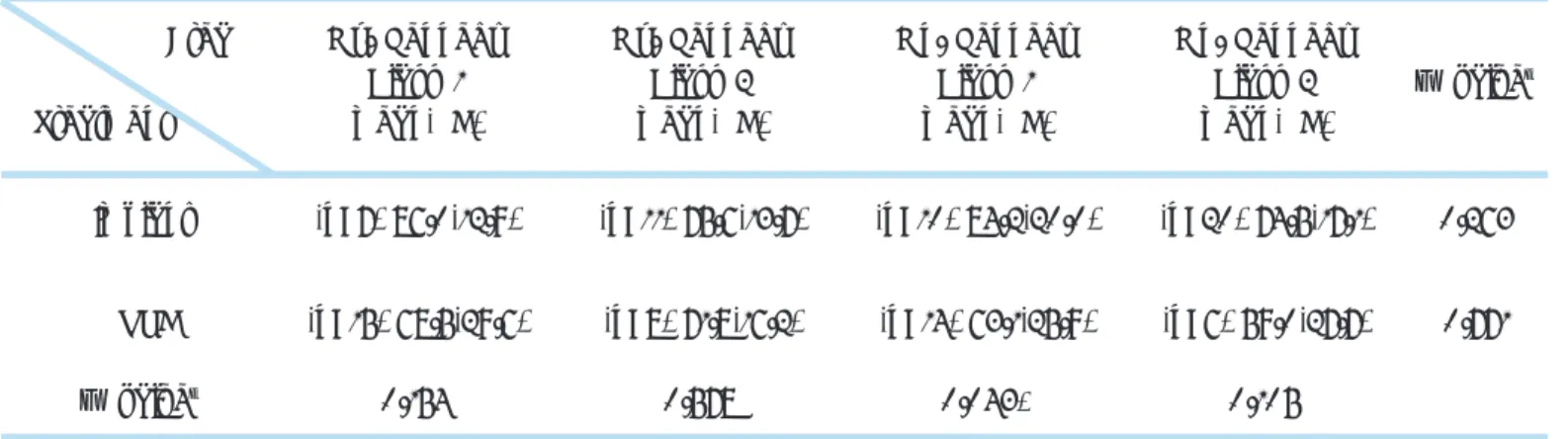
Table 3. Satisfaction (VAS scores) according to function period
*Ρvalue was statistically significant (P<0.05)
†Independent t-test, ‡one-way analysis of variance (ANOVA)
Period Treatment
Implant
RPD
Ρ value†
(n=7) 85.1(12.0)
(n=20) 70.1(25.4)
0.147
(n=8) 72.0(15.7)
(n=6) 77.3(12.6)
0.509
(n=27) 76.1(17.5)
(n=11) 52.2(29.7)
0.027*
0.294
0.098 2mo-1yr
mean(SD)
1yr-2yr mean(SD)
more than 2yr
mean(SD) Ρ value‡
for the period from 1 year to 2 year, but in more than 2 years only, a significantly better satisfaction (P=0.027).
In all missing areas (Table 4), the implant group had a higher satisfaction than the conventional RPD, but in the mandible of Kennedy class 1 only, a significantly better satisfaction (P=0.043).
3. Satisfaction comparisons within group
Both Subjects who had received implants or conventional RPD had no significantly different
satisfaction according to function period and missing areas (Table 3 ; Table 4). Conventional RPD subjects who had experienced previous removable denture, had lower satisfaction and for the implant subjects who had experienced previous removable denture, slightly higher satisfaction was found but not significantly different (Table 5).
4. The univariate regression analyses in the implant group (Table 6) indicate that all factors had a significant effect on patient ratings of general satisfaction (P<0.05), Table 4. Satisfaction (VAS scores) according to missing areas
Area Treatment
Mx. Kennedy Class 1 mean(SD)
Mx. Kennedy Class 2 mean(SD)
Mn. Kennedy Class 1 mean(SD)
Mn. Kennedy Class 2 mean(SD)
Ρ value‡
Implant (n=7) 86.0(12.9) (n=11) 75.6(13.7) (n=10) 84.2(20.0) (n=20) 74.5(17.1) 0.263
RPD (n=15) 68.5(29.6) (n=8) 71.8(16.2) (n=14) 63.1(25.9) (n=6) 59.0(27.7) 0.771
Ρ value‡ 0.154 0.578 0.043* 0.105
*Ρ value was statistically significant (P<0.05)
†Independent t-test, ‡one-way analysis of variance (ANOVA)
Denture experience Treatment
Yes mean(SD)
No
mean(SD) Ρ value‡
Implant (n=16)
78.8(16.5)
(n=26)
75.6(16.8) 0.558
RPD (n=17)
56.9(28.5)
(n=20)
73.6(22.4) 0.054
*one-way analysis of variance (ANOVA)
Table 5. Satisfaction according to previous removable denture experience
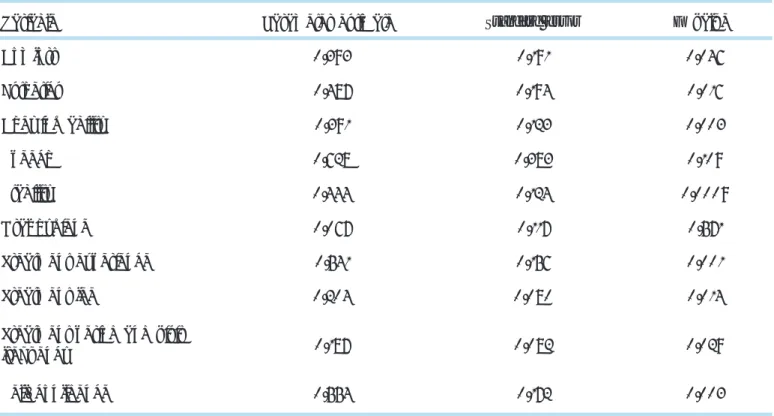
except for speech, oral hygiene. However, in the final model (Table 7), multiple regression methods show that this effect was not observed and patient ratings of stability, treatment fee and self-confidence were significant predictors of implant satisfaction (R- square=0.449, P<0.0001).
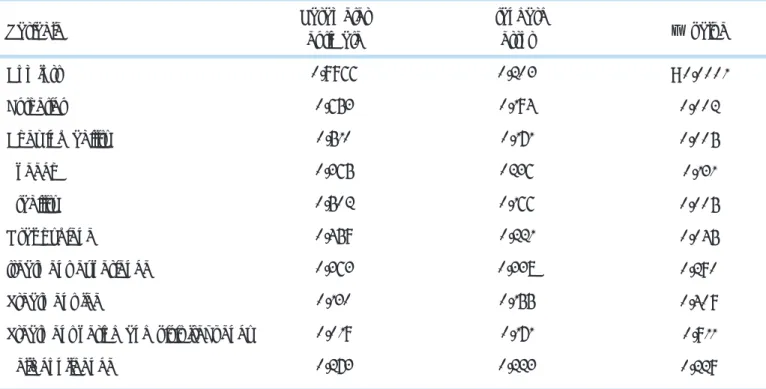
For the conventional RPD group, the univariate regression analyses (Table 8) indicate that factors of comfort, esthetics, chewing ability, stability, and oral hygiene had a significant effect on patient ratings of general satisfaction (P<0.05). However, in the final model (Table 9), multiple regression analyses show that Table 6. Univariate regression analysis in implant group
Variable Parameter estimate Standard error Ρ value
Comfort 0.393 0.191 0.046
Esthetics 0.487 0.194 0.016
Chewing ability 0.391 0.123 0.003
Speech 0.628 0.383 0.109
Stability 0.444 0.124 0.0009
Oral hygiene 0.067 0.117 0.571
Treatment experience 0.541 0.156 0.001
Treatment fee 0.204 0.080 0.014
Treatment period and visit
frequency 0.187 0.082 0.029
Self-confidence 0.554 0.172 0.003
Table 7. Multiple regression analysis in implant group
R-square=0.449, (Ρ<0.0001)
Variable Parameter estimate Standard error Ρ value 95% CI
Stability 0.307 0.115 0.012 0.080-0.533
Treatment fee 0.152 0.068 0.031 0.019-0.286
Self-confidence 0.471 0.150 0.003 0.178-0.765
comfort only was significant predictor (R- square=0.394, P<0.0001). Addition of any other variables failed to improve the final model.
Discussion
Dental implants have demonstrated high success rates, as judged by clinicians, based on biologic and esthetic criteria. However, the importance of evaluating the
implant treatment from the patient standpoint so as to assess their acceptance of the treatment outcome has not been adequately recognized in the literatures, even though it has been suggested that implant success criteria should include the level of patient acceptance of the treatment (Zarb & Albrektsson, 1998).
The purpose of this study was to compare the overall satisfaction of implant-supported fixed prostheses with conventional removable partial denture(RPD) in the distal extension missing areas. For most categories, the improvement in the implant group was greater, as
IV
Table 8. Univariate regression analysis in RPD group
Variable
Comfort Esthetics Chewing ability Speech
Stability Oral hygiene
treatment experience Treatment fee
Treatment period and visit frequency Self-confidence
Parameter estimate
0.9966 0.653 0.510 0.365 0.502 0.459 0.363 0.130 0.019 0.273
Standard error 0.203 0.194 0.171 0236 0.166 0.221 0.338 0.155 0.171 0.223
Ρ value
< 0.0001 0.002 0.005 0.131 0.005 0.045 0.290 0.409 0.911 0.229
Table 9. Multiple regression analysis in RPD group
R-square=0.394, (Ρ<0.0001)
Variable Parameter estimate Standard error Ρ value 95% CI
Comfort 0.966 0.203 < 0.0001 0.569-1.357
illustrated by the higher satisfaction scores given by this group for most variables. General satisfaction was slightly higher in the group with implant-supported fixed partial dentures, who also gave significantly higher ratings for comfort, esthetics, speech, stability, treatment experience, and self-confidence, compared to that of conventional dentures. No patient-based assessments after treatment with implant-supported fixed prostheses in the distal extension areas have been reported but this result is in agreement with previous similar studies. For example, patient reponses to mandibular implant overdentures have been reported (Pera et al, 1998 ; Kapur et al, 1999). Randomized clinical trials have been shown that mandibular two- implant overdentures provide significant improvement in stability and retention in patients with severe problems adapting to conventional dentures and in medically compromised patients. Boerrigter et al (1995) reported that 1 year after treatment, there were significantly fewer functional complaints from subjects wearing mandibular two-implant overdentures than from those wearing conventional dentures.
The use of fixed prostheses supported by implants rather than conventional removable prostheses to restore the missing areas offers the advantage of less bulk, a more normal contour, improvement in chewing ability, comfort, and a more profound effect upon patient acceptance
(Jepson et al, 2003). The main reason why patients choose implant treatments rather than conventional dentures was due to reluctance to removable dentures as demonstrated by objective questions that were asked in this survey. Hence, a fixed prosthesis would be the
treatment of choice because it is more stable than any other removable appliance (DeBoer, 1993).
The implant subjects appeared dissatisfied with both the cost and the time it took to complete their treatment compared to conventional dentures. This results were consistent with objective questions that were asked. The first two of patient dissatisfaction associated with implant treatments were time and cost. However, time was not significant, while cost approached significance (P=0.028) (Table 2). These findings may suggest that patients do not find dental implant treatment inexpensive, but patients who proceed with this procedure are more often those who can afford it, making other personal considerations more important in their overall satisfaction (Levi et al, 2003).
Oral hygiene was considered somewhat more difficult to perform in the implant group than conventional denture. The diameter of the implant pillar platform does not comply with the diameter of the superstructure in molar regions, which results in an overhanging design (Yi et al, 2001). Other previous study showed that a mandibular long-bar overdenture was much easier to clean than a fixed bridge (de Grandmont et al, 1994), and patients find that oral hygiene is easier to manage with removable appliances (Beumer et al, 1993 ; DeBoer, 1993 ; Zarb & Schmitt, 1996).
Chewing ability was rated better with implant than with conventional denture but was not statistically significant. However, the differences between the prostheses were strongly dependent on the type of food.
Rice was the easiest to chew, and the difference between the prostheses was small. It was greater for carrot and nuts and difficulties in chewing become most
evident when tough and hard foods are being chewed (Geertman et al, 1996).
Speech problems are probably more strongly associated with maxillary prostheses since speech is influenced by factors such as maxillary anterior tooth form, position, and palatal coverage (Petrovic, 1985 ; Sones, 1989).
Between the period of 1 year less and 2 years more, there was a trend of decrease of satisfaction irrespective of type of treatments. This time-dependent changes may result from late complications such as screw-loosening, material fracture, frequent denture adjustment like relining or repair. Otherwise, a steady decline in the number of people who continued to wear their RPDs with the passage of time. Nonwearing and dissatisfaction are intimately linked (Nakazawa, 1977 ; Wetherell & Smales, 1980). Weinstein et al (1988) indicated that the longer the patients used RPDs, the more their neuromuscular control of the appliance may develop, and their speaking ability improve. Also, the patients may have more realistic expectations for their speaking ability based on their past experience with dentures.
The fact that removable dentures were partially supported by the mucosa could be the main reason for lower ratings for comfort, chewing ability, stability. It has also been suggested that the much lower levels of satisfaction that characterize conventional mandibular dentures are probably due almost entirely to the poor bearing properties of the soft tissues (Boerrigter et al, 1995 ; Burns et al, 1995). This is in agreement with that patients with Kennedy class 1 who have mandibular bilateral edentulous molar areas revealed significant differences between implant and dentures. It has been
proposed that the level of comfort is related to the degree of bone resorption under the denture (Humphris et al, 1995).
According to Frank et al (1998 ; 2000), the patients who had experience with previous RPDs were more satisfied than the patients with their first ever RPDs. Contrary to Frank, this study reported less overall satisfaction in those who have had prior experience with RPDs. The presence of past experience includes both positive and negative results. Thus, past experience alone may not be highly predictive of future satisfaction. Changes in the oral conditions, expectations, or in the patient-dentist relationship could result in an unsatisfactory outcome even in those with a positive past dental history. In those who were dissatisfied with a previous RPD, it is not always possible to determine the true cause of failure and whether it can be avoided in the future.
Clinicians must be careful in interpreting the association between past experience and patient satisfaction. It was also thought that patients with a lower economic status might be less satisfied than their expectation of RPDs and patients with a greater number of missing teeth in the mandible might have more uncomfortable RPDs in comparison with previous fewer missing teeth (Knezovic et al, 2003).
The influence of the patient age, gender, the socioeconomic status, marital status on the patient satisfaction has already been studied in several other papers, so this study had a focus on clinical variables such as function and psychological factor. The three variables that were of primary importance in the implant patient satisfaction were stability, treatment fee, and self-confidence (Table 7). The former represents
function and the latter two reflects upon psychological aspect. On the other hand, the variables that were of primary importance in the denture patient satisfaction was comfort (Table 9). This reflects upon function. This results provide in patient satisfaction of the removable dentures, function is more important than psychological factor. For some patients, the satisfaction with their RPDs relates primarily to the comfort and ability to masticate (Kay, 1993). The esthetics and retention also seem to be important (Hakestam et al, 1997).
The reliability of VAS has been discussed in several dental papers. In assessing the within-subject comparisons of implant-supported mandibular prostheses, de Grandmont et al (1994) used both VAS and a category scale, and reported that the two scales gave similar results. Lamb and Ellis (1995 ; 1996) claimed that the VAS scale is the most efficient method for measuring patient-assessed denture security. A ceiling or floor effect can reduce sensitivity and lead to an underestimation of the real difference between groups. Ceiling and floor effects are less of a problem with VAS than with other instruments such as category scales where the subject has a limited choice of numbers or words (Duncan et al, 1989). A conflicting view exists in the study by Magnusson et al (1995) that a behavior rating scale with six-point verbal categories was superior to the other scales including VAS, in respect of precision and sensitivity to pain and discomfort in patients with temporomandibular disorder. The verbal scales, however, are generally believed to have some disadvantages. Relatively large divisions are insensitive to graduations in patient feelings and the meaning of the sentence excessively
influences their responses.
There are several limitations to this study. The study design was retrospective and relied on subject memory and may have introduced an associated bias.
Retrospective study is less likely to consistently follow every factor for every patient. This study is quite likely to record major adverse events (Steven, 2003). Another weakness of this study is that data collected through the self-administrated questionnaire might be misinterpretated by the subjects about the questions.
Third, because the sample size was small (n=79), variables that were not shown to be statistically significant may have demonstrated significance with a larger sample size. Finally, the selected patients were all treated at the USH.
Additional studies should be carried out to further evaluate the importance of the type of opposing dentition, number and location of remaining teeth, periodontal health, and previous medical history.
In summary, our results showed that in the distal extension missing areas, patients with implant- supported prostheses had no significantly better overall satisfaction than the conventional removable partial dentures. But the implant group had a significantly higher VAS scores on comfort, esthetics, speech, stability, treatment experience, and self-confidence.
Hence, the use of osseointegrated implants as abutments for fixed partial dentures can be a predictable restorative alternative for the distal extension missing areas.
References
1. Awad MA, Lund JP, Dufresne E, Feine JS. Comparing the efficacy of mandibular implant-retained overdentures and conventional dentures among middle-aged edentulous patients : satisfaction and functional assessment. Int J Prosthodont 2003 ; 16 : 117-122.
2. Becker W, Becker BE, Alsuwyed A, Al-Mubarak S. Long-term evaluation of 282 implants in maxillary and mandibular molar positions : a prospective study. J Periodontol 1999 ; 70 : 896-901.
3. Beumer J Ⅲ, Hamada MO, Lewis S. A prosthodontic overview. Int J Prosthodont 1993 ; 6 : 126-130.
4. Boerrigter EM, Geertman ME, van Oort RP, Bouma J, Raghoebar GM, van Waas MAJ. Patient satisfaction with implant-retained mandibular overdentures : a comparison with new complete dentures not retained by implants-a multicenter randomized clinical trial. Br J Oral Maxillofac Surg 1995 ; 33 : 282-288.
5. Brudvik JS. Advanced removable partial dentures. 1st ed. Chicago : Quintessence 1999 : 153.
6. Burns DR, Unger JW, Elswick RK Jr, Beck DA. Prospective clinical evaluation of mandibular implant overdentures : Part I. Retention, stability, and tissue response. J Prosthet Dent 1995 ; 73 : 354-363.
7. Burns DR, Unger JW, Elswick RK Jr, Giglio JA. Prospective clinical evaluation of mandibular implant overdentures : Part II. Patient satisfaction and preference. J Prosthet Dent 1995 ; 73 : 364-369.
8. DeBoer J. Edentulous implants : overdenture versus fixed. J Prosthet Dent 1993 ; 69 : 386-390.
9. De Grandmont P, Feine JS, Tache R, Boudrias P, Donohue WB, Tanguay R. Within-subject comparisons of implant-supported mandibular prostheses : psychometric evaluation. J Dent Res 1994 ; 73 : 1096-1104.
10. Duncan GH, Bushnell MC, Lavigne GJ. Comparison of verbal and visual analogue scales for measuring the intensity and unpleasantness of experimental pain. Pain 1989 ; 37 : 295-303.
11. Frank RP, Milgrom P, Leroux BG, Hawkins NR. Treatment outcomes with mandibular removable partial dentures : a population-based study of patient satisfaction. J Prosthet Dent 1998 ; 80 : 36-45.
12. Frank RP, Brudvic JS, Leroux B, Milgrom P, Hawkins N. Relationship between the standards or removable partial denture construction, clinical acceptibility, and patient satisfaction. J Prosthet Dent 2000 ; 83 : 521-527.
13. Garrett NR. Kapur KK, Perez P. Effects of improvements of poorly fitting dentures on patient satisfaction. J Prosthet Dent 1996 ; 76 : 403- 413.
14. Geertman ME, Boerrigter EM, van't Hof MA, van Waas MAJ, van Oort RP, Boering G. Two-center clinical trial of implant-retained mandibular overdentures versus complete dentures-chewing ability.
Community Dent Oral Epidemiol 1996 ; 24 : 79-84.
15. Hakestam U, Karlsson T, Soderfeldt B, Ryden O, Glantz P. Does the quality of advanced prosthetic dentistry determine patient satisfaction?
Acta Odontologica Scandinavica 1997 ; 55 : 365-371.
16. Harle TJ, Anderson JD. Patient satisfaction with implant-supported prostheses. Int J Prosthodont 1993 ; 6 : 153-162.
17. Humphris GM, Healey T, Howell RA, Cawood J. The psychological impact of implant-retained mandibular prostheses : a cross-sectional study. Int J Oral Maxillofac Implants 1995 ; 10 : 437-444.
18. Jepson N, Allen F, Moynihan P, Kelly P, Thomason M. Patient satisfaction following restoration of shortened mandibular dental arches in a randomized controlled trial. Int J Prosthodont 2003 ; 16 : 409-414.
19. Kapur KK, Garrett NR, Hamada MO. Randomized clinical trial comparing the efficacy of mandibular implant-supported overdentures and conventional dentures in diabetic patients : Part Ⅲ. Comparisons of patient satisfaction. J Prosthet Dent 1999 ; 82 : 416-427.
20. Kay EJ. Patients needs-more than meets the eye. Br Dent J 1993 ; 20 : 212-214.
21. Knezovic zlataric D, Celebic A, Valentic-peruzovic M, Jerolimov V. A survey of treatment outcomes with removable partial dentures. J Oral Rehabil 2003 ; 30 : 847-854.
22. Lamb DJ, Ellis B. Patient-assessed security changes when replacing mandibular complete dentures. Int J Prosthodont 1995 ; 8 : 135-142.
23. Lamb DJ, Ellis B. Comparisons of patient self-assessment of complete mandibular denture security. Int J Prosthodont 1996 ; 9 : 309-314.
24. Levi A, Psoter WJ, Agar JR, Reisine ST, Taylor TD. Patient self- reported satisfaction with maxillary anterior dental implant treatment.
Int J Oral Maxillofac Implants 2003 ; 18 : 113-120.
25. Magnusson T, List T, Helkimo M. Self-assessment of pain and discomfort in patients with temporomandibular disorders : a comparison of five different scales with respect to their precision and sensitivity as well as their capacity to register memory of pain and discomfort. J Oral Rehabil 1995 ; 22 : 549-556.
26. Nakazawa I. A clinical survey of removable partial dentures : analysis of follow-up examinations over a 16-year period. Bull Tokyo Med Dent Univ 1977 ; 24 : 125-137.
27. Nassif J. A self-administered questionnaire-an aid in managing complete denture patients. J Prosthet Dent 1978 ; 40 : 363-366.
28. Pera P, Bassi F, Schierano G, Appendino, Preti G. Implant anchored complete mandibular denture : evaluation of masticatory efficiency, oral function and degree of satisfaction. J Oral Rehabil 1998 ; 25 : 462- 467.
29. Petrovic A. Speech sound distortions caused by changes in complete denture morphology. J Oral Rehabil 1985 ; 12 : 69-79.
30. Sones AD. Complications with osseointegrated implants. J Prosthet Dent 1989 ; 62 : 581-585.
31. Steven EE, Yong-geun Choi, Sreenivas K. Methods for comparing the results of different studies. Int J Oral Maxillofac Implants. 2003 ; 18 : 697-705.
32. Wakabayashi N, Yatabe MAI, Sato M, Nakamura K. The influence of some demographic and clinical variables on psychosomatic traits of patients requesting replacement removable partial dentures. J Oral Rehabil 1998 ; 25 : 507-512.
33. Weinstein M, Schuchman J, Lieberman J, Rosen P. Age and denture experience as determinants in patient denture satisfaction. J Prosthet Dent 1988 ; 59 : 327-329.
34. Wetherell JD, Smales RJ. Partial denture failures : a long-term clinical survey. J Dent 1980 ; 8 : 333-340.
35. Yi SW, Carlsson GE, Ericsson I, Kim CK. Patient evaluation of treatment with fixed implant-supported partial dentures. J Oral Rehabil 2001 ; 28 : 998-1002.
36. Zarb GA, Schmitt A. The edentulous predicament Ⅱ. The longitudinal effectiveness of implant-supported overdentures. J Am Dent Assoc 1996 ; 127 : 66-72.
37. Zarb GA, Albrektsson T. Consensus report : Towards optimized treatment outcomes for dental implants<editorial>. Int J Prosthodont 1998 ; 5 : 385-389.
reprint request to Young Ho Kim
Clinical Associate Professor
Department of Orthodontics, The Institute of Oral Health & Science, Samsung Medical Center, Sungkyunkwan University Medical College, Kangnam-Gu Irwon-Dong 50, Seoul, Korea
E-mail : [email protected]
국
국문문초초록록
임프란트의 출현은 총의치, 단일치의 수복, 전악 고정성 수복에 대한 우리의 생각을 극적으로 변화시켰다. 그러나 후방연장 결손부에서 치과 임프란트로 수복한 환자의 만족도에 관한 조사는 행해지지 않았다. 이 연구는 후방연장 결손부에서 임프란 트 지지 고정성 보철물로 수복한 환자와 일반적인 가철성 국소의치로 수복한 환자의 만족도를 조사하였다. 임프란트 지지 고 정성 보철물로 수복한 환자 42명과 일반적인 가철성 국소의치로 수복한 환자 37명을 검사하였다. 환자들은 최종 보철물 장착 후 2개월 이상 지난 다음, 100mm VAS 점수로 치료의 전반적인 만족도와 기타 보철물의 특징들(편안함, 심미성, 저작능력, 발음, 안정, 구강위생, 치료경험, 치료비, 치료기간과 내원빈도, 자신감)을 평가하였다. 두 군 모두, 구강기능, 환자의 만족도 와 같은 치료결과와 관련된 다양한 임상적 요소에 초점이 맞추어진 41개로 구성된 설문지에 답변을 하여 다음과 같은 결과를 얻었다.
1. 임프란트 군은 일반적인 가철성 국소의치 군보다 나은 전반적인 만족도를 보였으나 유의성있는 차이는 없었다. 임프란트 군은 편안함, 심미성, 발음, 안정, 치료경험, 자신감에서 국소의치 군보다 유의하게 높은 값을 보였다. 국소의치 군은 구강 위생, 치료비, 치료기간과 내원빈도에서 임프란트 군보다 높은 값을 보였으나, 구강위생과 치료기간과 내원빈도는 유의한 차이를 보이지 않았다.
2. 기능기간에서 임프란트 군은 1년에서 2년 사이의 기간을 제외하고 국소의치 군보다 높은 만족도를 보였으나, 2년 이상의 기간에서만 유의하게 높은 만족도를 보였다 (Ρ=0.027).
3. 모든 결손 부위에서 임프란트 군은 국소의치 군보다 높은 만족도를 보였으나, 하악의 케네디 분류 1급에서만 유의하게 높 은 만족도를 보였다(Ρ=0.043).
4. 이전의 가철성 의치 경험을 가진 국소의치 환자는 낮은 만족도를 보였고, 이전의 가철성 의치 경험을 가진 임프란트 환자 는 약간 높은 만족도를 보였으나 두 군 모두 유의한 차이는 없었다.
5. 임프란트 환자의 만족도에서 가장 중요한 변수는 안정, 치료비, 자신감이었으며 (P<0.0001), 국소의치 환자의 만족도에서 는 편안함이었다 (Ρ<0.0001).
결론적으로, 고정성 국소의치의 지대치로서 골유착 임프란트의 이용은 후방연장 결손부에서 예측 가능한 수복 대체법이라고 할 수 있다.