55 https://jes-online.org
Minimally invasive video assisted thyroid and parathyroid surgery (MIVAT/MIVAP) has become a common approach worldwide and is being performed for malignant thyroid nodules and bilateral neck exploration for parathyroid as well (1). It is a central gasless approach as compared to the endoscopic approach proposed by Gagner (2) and other approaches described using CO2 insufflation, external retraction, lateral access as proposed by Henry et al. (3). The advantages of MIVAT/MIVAP are smaller incision, early post-operative recovery and lesser pain leading to better patient satisfaction. Other advantages arise due to the use of magnifying endoscope enabling an easier identification of the recurrent laryngeal nerves (RLNs), external branch of superior laryngeal nerves and parathyroids (4). We here describe a modified single port MIVAT/MIVAP technique using tubular retractor system.
The authors modified the gasless minimally invasive video assisted thyroid and parathyroid surgery technique.
Pre-operative preparation: pre-operative preparation and evaluation is same as for conventional surgery.
Surgical technique: patient is placed in supine position with neck in slight extension.
Painting and draping are done in such a way as to allow conversion to conventional surgery. Operating room set up and instruments are similar to those required for advanced laparoscopic procedures, including ultrasonic energy devices and high-definition camera system. A 1.5 cm transverse incision is made 2 cm above the sternal notch or over a skin crease if present. Subplatysmal flaps are created, and midline of strap muscle opened in case of thyroid surgery. Strap muscles are separated from the visceral surface of gland, followed by lateral dissection and separation from medial border of sternocleidomastoid and carotid artery is identified. At this point a tubular retractor which has self-retaining endoscope port is inserted to maintain the operative space. A 30-degree endoscope, 5 mm in diameter, is then fixed over the tubular retractor. Endoscopic surgical instruments including atraumatic spatulas, a spatula shaped aspirator, ear-nose-throat forceps and scissors are inserted, and procedure is then conducted endoscopically. Inferior thyroid vein is ligated using ultrasonic device and isthmusectomy is the next step which helps in providing traction while dissecting the lobe. The RLN and inferior parathyroid gland (PG) are identified using blunt dissecting forceps. After this, lobe is pulled down and rotated medially which helps in visualizing J Endocr Surg. 2021 Jun;21(2):55-58
https://doi.org/10.16956/jes.2021.21.2.55 pISSN 2508-8149·eISSN 2508-8459
Short Communication
Received: May 20, 2021 Revised: Jun 8, 2021 Accepted: Jun 8, 2021 Correspondence to Sanjay Kumar Yadav
Department of Surgery, NSCB Medical College, Tilwara Road, Doctors Colony, Medical College Colony, Jabalpur 482003, India.
E-mail: [email protected]
Copyright © 2021. Korean Association of Thyroid and Endocrine Surgeons; KATES This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://
creativecommons.org/licenses/by-nc/4.0/).
ORCID iDs Sanjay Kumar Yadav
https://orcid.org/0000-0002-0682-4970 Chandan Kumar Jha
https://orcid.org/0000-0003-0968-3269 Goonj Johri
https://orcid.org/0000-0002-3699-7338 Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Conceptualization: Sanjay Kumar Yadav, Chandan Kumar Jha; Data curation: Sanjay Kumar Yadav; Formal analysis: Sanjay Kumar Yadav, Goonj Johri; Investigation: Sanjay Kumar Yadav; Methodology: Sanjay Kumar Yadav; Project administration: Sanjay Kumar Yadav; Resources: Sanjay Kumar Yadav;
Supervision: Sanjay Kumar Yadav; Validation:
Sanjay Kumar Yadav; Visualization: Sanjay
Sanjay Kumar Yadav 1, Chandan Kumar Jha 2, Goonj Johri 3
1Department of Surgery, NSCB Medical College, Jabalpur, India
2Department of Surgery, All India Institute of Medical Sciences, Patna, India
3Department of Surgery, All India Institute of Medical Sciences, Raebareli, India
A Modified Single Port Minimally
Invasive Video Assisted Thyroid and
Parathyroid Surgery Technique Using
Tubular Retractor System
Kumar Yadav; Writing - original draft: Sanjay Kumar Yadav; Writing - review & editing:
Sanjay Kumar Yadav, Chandan Kumar Jha, Goonj Johri.
superior pole. The superior PG and external branch of the superior laryngeal nerve are identified and secured, and lobe is dissected off the trachea by dividing Berry's ligament.
For parathyroid surgery we prefer lateral approach and hence midline is not divided.
Working space is created under direct vision and tubular retractor is fixed between sternocleidomastoid and lateral surface of thyroid lobe. This exposes the thyro-tracheal groove. Endoscopic magnification allows for easier identification of the adenoma, RLN and inferior thyroid artery. Once the adenoma is visualized, gentle and precise manipulation is done to not the damage the capsule. Adenoma is mobilized until the hylus of the gland is reached, vessels ligation is performed by ultrasonic device. Finally, the adenoma is removed and retrieved through the skin incision.
We describe 2 representative cases (1 focused parathyroidectomy and 1 hemithyroidectomy) using this technique.
Case 1: a 40-year lady presented with history of bony pain and recurrent renal calculi for 4 years. On evaluation biochemical diagnosis of primary hyperparathyroidism was made.
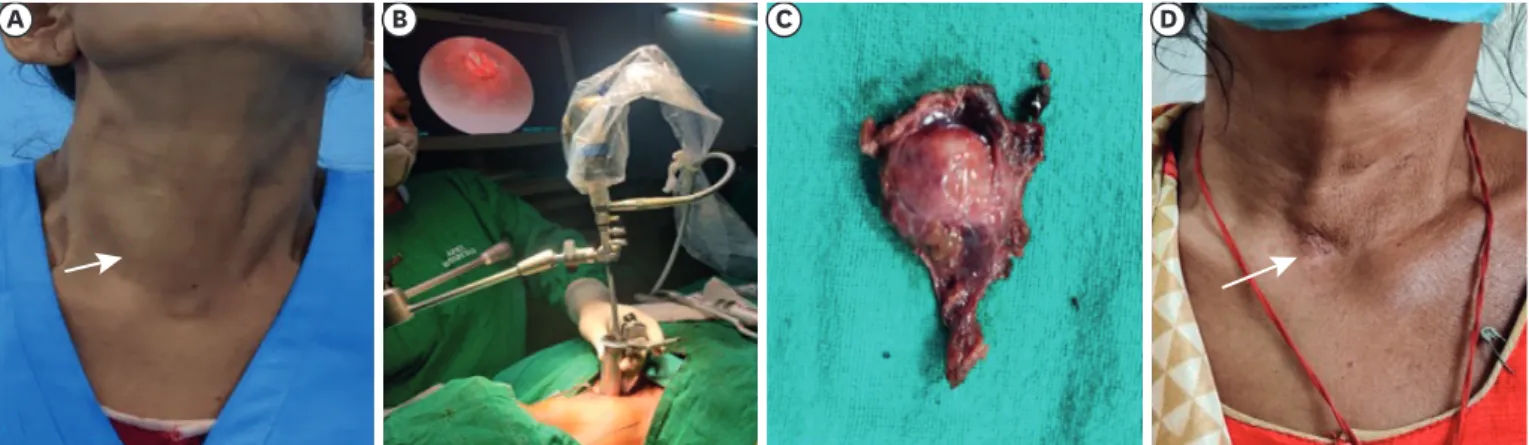
Functional imaging with SestaMIBI scan was suggestive of right superior parathyroid adenoma and anatomical imaging with ultrasonography was concordant with it. She underwent modified MIVAP using tubular retractor in October 2020 (Fig. 1A) and right superior focused parathyroidectomy was performed (Fig. 1B and C). Operative time was 40 minutes. Post- operatively patient had usual course and discharged on day 2. She did not develop any transient or permanent RLN injury, seroma, or haematoma. After 3 months follow-up her calcium and parathormone levels are normal and she is satisfied with her scar (Fig. 1D).
56 https://jes-online.org https://doi.org/10.16956/jes.2021.21.2.55
Modified Gaseless Central Access Minimally Invasive Parathyroid Surgery
A B
C D
Rt RLN
Rt sup parathyroid
Rt inf parathyroid
Fig. 1. (A) Set up for parathyroidectomy using tubular retractor, (B) intra-operative endoscopic view showing right superior parathyroid adenoma, (C) excised adenoma (D) neck scar at 3 months follow-up.
Rt = right; RLN = recurrent laryngeal nerve.
Case 2: a 63-year lady presented with right side thyroid nodule for 6 years. Triple assessment (serum thyroid stimulating hormone, ultrasonography of neck and fine needle aspiration cytology) established the diagnosis of benign euthyroid right solitary thyroid nodule. She underwent modified MIVAT using tubular retractor in February 2021 (Fig. 2). Post-operative course was uneventful, and she did not develop any transient or permanent RLN injury, seroma, or haematoma. She was discharged on first post-operative day. After 3 months follow-up, she is satisfied with her scar.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was taken from patient.
Surgical management of thyroid and parathyroid lesions is guided by patient's choice and tumour factors. Recently remote access approaches have gained popularity globally as they leave no scar over neck. However, several factors limit their widespread dissemination such as technical difficulty, long learning curve and invasiveness (5). Whereas MIVAT/MIVAP is a safe and effective procedure in selected cases (5). Another advantage is that bilateral neck exploration can be performed easily with this approach as compared to remote access approaches where it is technically more difficult.
Our modification of using tubular retractor makes MIVAP ergonomically easier. In Miccoli's approach (1) 3 surgeons are needed to perform the video assisted procedure. The surgeon holds a spatula for dissection. The first assistant holds the endoscope and a spatula-aspirator.
The second assistant holds the small retractors. Use of tubular retractor obviates the need of third assistant. The superior ergonomics, a similitude to conventional surgery and excellent cosmesis are major advantages.
There are few limitations as well. Thyroid surgery was technically challenging using tubular retractor and hence we did not repeat it on any other patient. We prefer transoral endoscopic approach for thyroid nodules up to 4 cm. Other limitation is considerable learning curve required for surgeons not well versed with endoscopic thyroid surgery. We are routinely performing remote access thyroid surgeries and hence for us it was easier.
57 https://jes-online.org https://doi.org/10.16956/jes.2021.21.2.55
Modified Gaseless Central Access Minimally Invasive Parathyroid Surgery
A B C D
Fig. 2. (A) Right benign euthyroid solitary thyroid nodule, (B) set up for hemithyroidectomy using tubular retractor, (C) excised nodule, (D) scar mark at 3 months follow-up.
In conclusion, this modified MIVAP technique using tubular retractor is safe, feasible and requires less surgeons.
REFERENCES
1. Miccoli P, Pinchera A, Cecchini G, Conte M, Bendinelli C, Vignali E, et al. Minimally invasive, video- assisted parathyroid surgery for primary hyperparathyroidism. J Endocrinol Invest 1997;20:429-30.
PUBMED | CROSSREF
2. Gagner M. Endoscopic subtotal parathyroidectomy in patients with primary hyperparathyroidism. Br J Surg 1996;83:875.
PUBMED | CROSSREF
3. Henry JF, Raffaelli M, Iacobone M, Volot F. Video-assisted parathyroidectomy via the lateral approach vs conventional surgery in the treatment of sporadic primary hyperparathyroidism: results of a case-control study. Surg Endosc 2001;15:1116-9.
PUBMED | CROSSREF
4. Scerrino G, Melfa G, Raspanti C, Rotolo G, Salamone G, Licari L, et al. Minimally invasive video-assisted thyroidectomy: analysis of complications from a systematic review. Surg Innov 2019;26:381-7.
PUBMED | CROSSREF
5. Dionigi G. Evidence-based review series on endoscopic thyroidectomy: real progress and future trends.
World J Surg 2009;33:365-6.
PUBMED | CROSSREF
58 https://jes-online.org https://doi.org/10.16956/jes.2021.21.2.55
Modified Gaseless Central Access Minimally Invasive Parathyroid Surgery