서론
2000년대에 들어서면서 초음파기기의 발달로 2 mm이
상의 갑상선결절을 찾아낼 수 있게 되고, 초음파의 사용이
보편화되면서 갑상선결절과 갑상선암의 발견이 증가하게
되었다[1]. 또한 갑상선결절의 초음파 소견에 대한 자료가
축적되면서 초음파검사로 갑상선암의 위험도를 예측할 수
있게 되었다[2]. 그러나 악성의 위험도가 높은 초음파 소견
은 주로 갑상선유두암을 예측하는 소견들로서, 갑상선여포
암 혹은 여포변종 갑상선유두암은 특이적인 초음파 소견을
보이지 않으므로 초음파검사 만으로 갑상선암의 위험도를
정확하게 진단하는 데에는 한계가 있다.
초음파유도 하 미세침흡인세포검사(fine-needle aspi-
ration, FNA)는 갑상선결절을 진단하는 데 가장 정확하
초음파 소견과 미세침흡인결과가 일치하지 않는
갑상선결절
김 민 주1·이 가 희2 | 1서울대학교병원 헬스케어시스템 강남센터, 2서울특별시 보라매병원 내분비내과Thyroid nodules with discordant results of
ultrasonographic and fine-needle aspiration
findings
Min Joo Kim, MD1 · Ka Hee Yi, MD2
Department of Internal Medicine, 1Seoul National University Hospital Healthcare System Gangnam Center, Seoul, 2Seoul National University Boramae Medical Center, Seoul, Korea
Received: March 8, 2018 Accepted: March 22, 2018 Corresponding author: Ka Hee Yi
E-mail: khyi@snu.ac.kr © Korean Medical Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons. org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
As the detection of thyroid nodules increases, it is important to differentiate whether thyroid nodules are malignant or not. Ultrasonography-guided fine-needle aspiration cytology is the standard method to diagnose thyroid nodules. Ultrasonographic findings of thyroid nodules can predict the risk of malignancy, and fine-needle aspiration allows the examination of cytopathology of thyroid nodules. However, both are not perfect, with a certain degree of false negative or false positive results. Therefore, we can face thyroid nodules with discordant results of ultrasonographic and fine-needle aspiration findings. In the case of benign features on ultrasonography with malignant cytology, follicular thyroid cancer, follicular variant papillary thyroid cancer, cystic or degenerative changes of thyroid cancer, and thyroiditis are candidates for diagnosis. In contrast, for the nodules with ultrasonographic features of highly suspicious of malignancy but benign cytology, we can consider the possibility of thyroiditis, changes of benign nodule, and cystic changes of thyroid cancer. These various conditions may result in discordant results of ultrasonographic features and fine-needle aspiration cytology, which need special attention not to miss the diagnosis of malignant nodules.
고, 비용 대비 효율이 가장 큰 방법으로 확립되어 있다.
FNA검사로 수술 전 갑상선암의 위험도가 높은 갑상선
결절을 진단할 수 있게 됨으로써 이전 시대에 비해 양성
결절에 대한 갑상선 수술의 건수는 급감하게 되었다. 그
러나 갑상선초음파검사뿐 아니라 FNA검사도 완벽한 검
사는 아니어서 일정 비율 위음성 또는 위양성 결과를 보
인다[2,3]. 때문에 초음파검사에서 악성 위험도가 높은
소견을 보였는데 FNA결과가 양성으로 나오거나 반대
로 초음파 소견은 양성의 소견을 보였는데 세포검사에
서 악성의 가능성이 높은 결과가 나오는 경우를 임상에
서 접하게 된다[4]. 이런 경우 어떤 질환의 가능성이 있
는지, 정확한 진단을 위해 어떻게 접근해야 하는지 살펴
보고자 한다.
갑상선결절 초음파 소견 분류
갑상선결절은 초음파검사로 위치, 크기, 내부 성상, 모양,
경계 등을 관찰하게 된다. 초음파에서 악성위험도가 높은
소견은 미세석회화, 침상 혹은 소엽성 경계, 비평행 방향
혹은 앞뒤로 긴 모양, 고형, 저에코 소견 등이다[5]. 한 가
지 초음파 소견만을 가지고 갑상선결절의 악성 위험도를 예
측하기 어렵기 때문에 여러 가지 초음파 소견을 종합하여
갑상선결절의 악성 위험도를 예측하는 분류체계가 개발되
었는데, 2014년 영국갑상선학회, 2015년 미국갑상선학회
[6], 2016년 미국임상내분비학회·미국내분비학회·미국
메디치내분비학회 등에서 초음파 분류체계를 제시하였다.
우리 나라에서도 2005년 대한영상의학회에서 실무그룹을
만들어 다기관연구를 수행하고 이를 바탕으로 2006년 초
음파 소견에 따른 갑상선결절의 진단에 대한 권고안을 발
표하였다[7]. 이후 2011년 대한갑상선영상의학회에서 권고
안을 출판한 데 이어, 2016년에는 대한갑상선영상의학회
와 대한영상의학회가 공동으로 Korean Thyroid Imaging
Reporting and Data System (K-TIRADS)을 발표하였다
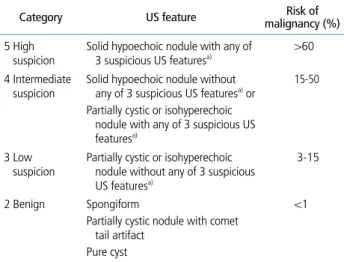
[2]. K-TIRADS에서는 갑상선결절의 성상과 에코, 악성결
절을 시사하는 소견(미세석회화, 비평행 방향, 침상 혹은 소
엽성 경계) 유무에 따라 K-TIRADS 2-5로 분류하고 있는
데 각각의 악성위험도는 Table 1과 같다[2]. K-TIRADS 2
나 3는 양성결절일 가능성이 높지만 K-TIRAD 5는 악성결
절일 가능성이 높다.
갑상선결절 FNA 결과 분류
FNA는 갑상선결절을 진단하는데 가장 정확하고 효과적
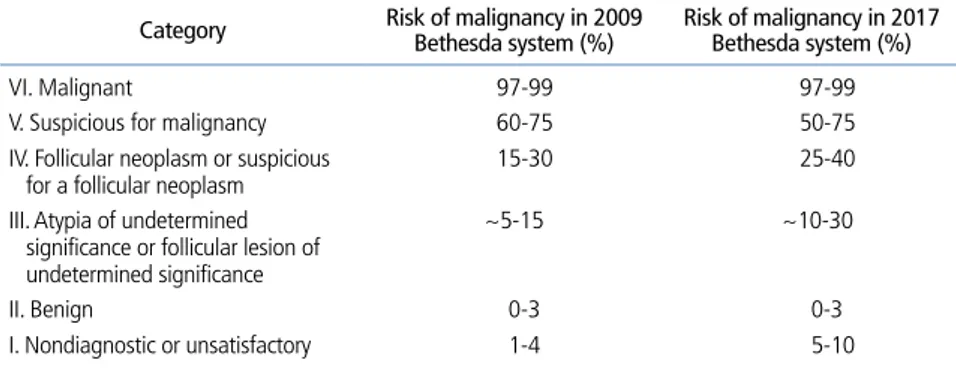
인 방법이다. FNA 결과는 2009년 발표된 The Bethesda
System for Reporting Thyroid Cytopathology (Bethesda
System)에 따라 보고되고 있다[8]. 세포검사 결과는 비진단
적, 양성, 비정형, 여포종양 혹은 여포종양 의심, 악성 의심,
악성 6가지로 분류하게 되고 각각의 악성 위험도는 Table 2
와 같다[8]. 이후 Bethesda System을 바탕으로 한 많은
연구들이 보고되었고[9], 이를 바탕으로 2017년 개정된
Bethesda System에서는 Table 2 [8]와 같이 악성 위험도
가 다소 조정되었다[3]. Bethesda 카테고리 II는 양성결절
일 가능성이 높지만 Bethesda 카테고리 V나 VI는 악성결절
일 가능성이 높다.
Table 1. Malignant risk of thyroid nodules according to Korean Thyroid
Imaging Reporting and Data System
Category US feature malignancy (%)Risk of 5 High
suspicion Solid hypoechoic nodule with any of 3 suspicious US featuresa) >60 4 Intermediate
suspicion Solid hypoechoic nodule without any of 3 suspicious US featuresa) or Partially cystic or isohyperechoic nodule with any of 3 suspicious US
featuresa)
15-50
3 Low
suspicion Partially cystic or isohyperechoic nodule without any of 3 suspicious US featuresa)
3-15
2 Benign Spongiform
Partially cystic nodule with comet tail artifact
Pure cyst
<1
Reproduced from Shin JH, et al. Korean J Radiol 2016;17:370-395, according to the Creative Commons license [2].
US, ultrasonography.
a)Microcalcification, nonparallel orientation (taller-than-wide),
초음파 소견과 FNA 결과의 불일치
초음파와 FNA가 악성결절을 감별진단하는데 많은 도움을
주기는 하지만, 두 검사 모두 완벽한 검사는 아니므로 위양성
과 위음성이 발생할 수 있기 때문에 임상에서 초음파와 FNA
결과가 일치하지 않는 경우가 발생할 수 있다. 이전 연구결과
에서 초음파와 FNA 결과가 일치하지 않는 경우가 4-10%로
보고되고 있다[4,10,11]. 여러 가지 경우
가 있을 수 있겠으나 본 논문에서는 초
음파에서 양성 소견이나 FNA에서 악성
이 의심되는 경우와 초음파에서 악성위
험도가 높은 소견이나 FNA에서 양성인
경우를 중심으로 살펴보고자 한다.
초음파에서 양성 소견이나
FNA에서 악성 소견인 경우
FNA에서 Bethesda 카테고리 V 악성
의심 또는 VI 악성인 경우 악성 위험도
가 50-99%이기 때문에 갑상선절제술
이 권고된다[5,6]. 그러나 FNA에서 악
성 의심이거나 악성이더라도 초음파 소
견이 양성결절을 시사하는 경우에는 많
게는 75%에서 양성결절일 수 있으므로
주의를 요한다[12]. 초음파에서 양성 소
견을 보였는데 FNA에서 악성 또는 악
성 의심으로 나올 수 있는 경우는 다음
과 같다(Figure 1A,1B).
1. 갑상선여포암
갑상선여포암은 갑상선유두암에 이어
두 번째로 흔한 암이지만, 우리나라에서
는 10% 미만으로 보고된다[13]. 갑상선
여포암과 갑상선여포선종은 초음파 소
견이나 FNA로 구분이 되지 않는다. 갑
상선여포암의 경우 FNA 결과 대부분 여포종양 혹은 여포종
양 의심으로 보고되지만 때로는 악성 의심이나 비정형으로
보고되는 경우도 있다. 갑상선여포암의 경우 상당수가 초음
파에서 양성 소견을 보인다[14]. 초음파에서 갑상선여포암의
경우 갑상선여포선종에 비해 저에코, 석회화 등의 악성 소견
을 많이 보인다는 보고도 있지만[15] 뚜렷한 차이를 보이지
않는다는 보고도 있다[14].
Table 2. Malignant risk of thyroid nodules according to the Bethesda System Thyroid Cytopathology
Category Risk of malignancy in 2009 Bethesda system (%) Risk of malignancy in 2017 Bethesda system (%) VI. Malignant 97-99 97-99 V. Suspicious for malignancy 60-75 50-75 IV. Follicular neoplasm or suspicious
for a follicular neoplasm 15-30 25-40 III. Atypia of undetermined
significance or follicular lesion of undetermined significance
~5-15 ~10-30
II. Benign 0-3 0-3 I. Nondiagnostic or unsatisfactory 1-4 5-10
Adapted from Cibas ES, et al. Am J Clin Pathol 2009;132:658-665 [8].
Figure 1. Thyroid nodules with discordant results of ultrasonography and fine-needle aspiration (FNA). (A,B)
Thyroid nodule showed low suspicion features (Korean Thyroid Imaging Reporting and Data System 3) in ul-trasonography, but FNA cytology (×400) was malignant (Bethesda category VI). The final pathology was follicular variant papillary thyroid carcinoma. (C,D) Thyroid nodule showed intermediate suspicion features (Korean Thyroid Imaging Reporting and Data System 4) in ultrasonography, but FNA cytology (×400) was benign (Bethesda category II).
A
C
B
2. 여포변종 갑상선유두암
여포변종 갑상선유두암은 갑상선유두암의 아형 중의 하나
로 우리나라에서는 10% 미만으로 보고되는데[16], 세포핵
은 갑상선유두암과 비슷하나 자라는 형태는 갑상선여포암
과 비슷하다. 여포변종 갑상선유두암의 초음파 소견은 갑상
선여포암의 경우와 마찬가지로 양성 소견을 보이는 경우가
많다[17].
3. 갑상선암의 낭성 변화나 퇴행성 변화
일부 갑상선암에서는 낭성 변화나 퇴행성 변화가 일어나,
초음파에서 양성 소견으로 판독될 수 있다[18].
4. 갑상선염
갑상선염이 있는 경우 FNA에서 위양성이 보다 많이 발생
한다[19]. 염증으로 인해 모양이 변형된 세포들이 갑상선암
세포로 오인될 수 있다[20].
5. 반복된 FNA
FNA를 시행하고 나면 출혈, 육아, 섬유화, 경색, 흉터 등
이 발생하게 되고 이러한 변화들 때문에 세포검사 결과가
위양성으로 보고될 수도 있다[21]. 초음파에서 양성 소견
을 보였으나 FNA에서 악성으로 나온 경우 한 번 더 FNA를
시행하거나 중심침생검을 시행하는 것이 좋다[22]. 중심침
생검은 갑상선결절을 진단하는데 있어 FNA만큼 정확한 검
사방법이기는 하나 갑상선결절의 진단에서 일차적인 검사
방법은 아니다. 현재는 FNA에서 비진단적 또는 비정형으
로 나온 경우에 주로 사용되고 갑상선암 이외의 암이 의심
되는 경우 등 선택적인 경우에도 권고되고 있다[23]. FNA
와 초음파 소견이 일치하지 않는 경우 FNA를 다시 시행하
는 것보다 우월하다는 근거는 부족하지만[24] 중심침생검
의 경우 보다 많은 조직을 얻을 수 있고 결절의 피막과 같
은 조직구조를 볼 수 있으며 면역화학염색을 할 수 있다는
장점이 있다.
BRAF나 RAS 유전자 돌연변이 검사 등의 분자표지자검
사가 도움이 될 수 있다[25]. Bethesda 카테고리 V 악성
의심의 경우에 BRAF 검사는 갑상선유두암 진단에 민감도
36-46%, 특이도 88-100%의 성적을 보였다[26,27]. 여러
가지 분자표지자들을 같이 검사할 경우 민감도와 특이도는
더욱 높아진다[26,28].
초음파에서 악성 소견이나 FNA에서 양성
소견인 경우
FNA에서 Bethesda 카테고리 II 양성인 경우 악성 위험도
가 3% 미만이다. 그러나 초음파검사에서 악성 위험도가 높
은 소견을 보이는데 FNA에서 양성인 경우[10], 악성 위험도
는 6-20%로 다소 높아진다[11,29]. 초음파에서 악성 위험
도가 높은 소견인데 FNA에서 양성 소견인 경우는 다음과 같
다(Figure 1C,1D).
1. 갑상선염
아급성 갑상선염이나 무통성 갑상선염 등에서 미만성 염
증 형태가 아니라 국소적 결절 형태처럼 보일 때가 있다. 이
런 경우 불규칙한 경계를 보이는 저에코 고형결절로 보이기
때문에 악성결절로 오인될 수 있다[30,31].
2. 양성결절의 변화
실제로는 양성결절인데 갑상선결절의 섬유화나 석회화
등으로 인해 초음파에서 악성 위험도가 높은 소견을 보
일 수 있다[32,33]. 결절이 오래되면 석회화가 생기는 경
우가 있는데 석회화는 악성을 시사하는 중요한 소견이다.
그러나 모든 석회화 소견이 악성을 시사하는 것은 아니다.
결절의 석회화는 1 mm 이하의 미세석회화와 1 mm를 초
과하는 거대석회화, 테두리석회화 등으로 나눌 수 있는
데, 미세석회화만이 악성결절에 특이적이다[2]. 실제 석
회화가 아니라 결절의 낭성 부분에 생긴 혜성꼬리허상
(comet-tail artifact)이 미세석회화로 오인되는 경우도
있다[2]. 또한 낭성결절이 시간이 지나면서 저절로 작아
지거나 치료 목적의 흡인 또는 에탄올절제술 이후에 크기
가 줄어들면서 악성 위험도가 높은 결절로 보이는 경우도
있다[34,35].
3. 갑상선암의 낭성 변화
일부 갑상선암에서는 낭성 변화가 일어난다. 낭성 부분에
대해 FNA를 시행할 경우 양성 또는 낭액만 흡인되어 비진단
적으로 나올 수 있다. 그러므로 낭성 부분이 있는 결절의 경
우 반드시 낭액을 흡인해 내고 난 후 고형 부분에서 FNA를 시
행해야 한다.
4. FNA 과정에서의 오류
갑상선암의 크기가 작거나 결절의 일부분에만 갑상선암
이 존재하는 경우 검체채취 과정에서 오류가 발생하기 쉽다
[36]. 검체채취 과정의 오류를 줄이기 위해서 촉진보다는 초
음파유도 하에 FNA를 시행하는 것이 권장된다[37]. FNA에
서 양성인 경우 즉각적인 추가 검사나 일상적인 치료는 권고
되지 않는다[5]. 그러나 FNA에서 양성이라도 초음파검사는
악성 위험도가 높은 소견을 보이는 경우 미국갑상선학회에
서는 1년 이내에 초음파 또는 초음파유도 하 FNA를 다시 시
행할 것을 권고하고 있다[6]. FNA보다 중심침생검이 도움이
되는 경우도 있다. 특히, 결절에 석회화가 있거나 퇴행성 변
화가 있는 경우 FNA를 반복하는 것 보다 중심침생검이 진
단에 더 도움이 될 수 있다[24,38]. 2번 이상의 FNA 또는 중
심침생검에서 양성으로 확인된 경우에는 악성 위험도가 거
의 0%이기 때문에 지속적으로 초음파 추적검사를 할 필요
는 없다[6].
결론
다양한 원인에 의해 초음파 소견과 FNA검사 결과가 일치
하지 않는 경우가 발생할 수 있다. 갑상선 양성결절이 악성
결절로 오인되면 환자가 불필요한 갑상선절제술을 받게 되
고, 갑상선 악성결절이 양성결절로 오인되면 암의 진단이 늦
어지고 치료가 지연된다. 따라서 갑상선결절을 진단할 때에
는 초음파와 FNA 소견을 같이 고려하여 판단하여야 하고
[39], 두 검사가 일치하지 않을 경우에는 위에 기술된 여러
가지 가능성을 고려하여 FNA 재검을 포함한 적절한 검사방
법을 통해 정확한 진단을 하도록 주의를 요한다.
찾아보기말:
미세침흡인세포검사; 갑상선결절; 초음파ORCID
Min Joo Kim, http://orcid.org/0000-0002-9765-9340 Ka Hee Yi, http://orcid.org/0000-0002-1999-9841
REFERENCES
1. Ahn HS, Kim HJ, Welch HG. Korea’s thyroid-cancer “epidemic”: screening and overdiagnosis. N Engl J Med 2014;371:1765-1767.
2. Shin JH, Baek JH, Chung J, Ha EJ, Kim JH, Lee YH, Lim HK, Moon WJ, Na DG, Park JS, Choi YJ, Hahn SY, Jeon SJ, Jung SL, Kim DW, Kim EK, Kwak JY, Lee CY, Lee HJ, Lee JH, Lee JH, Lee KH, Park SW, Sung JY; Korean Society of Thyroid Radiology (KSThR) and Korean Society of Radiology. Ultrasonography diagnosis and imaging-based management of thyroid nodules: revised Korean Society of thyroid radio-logy consensus statement and recommendations. Korean J Radiol 2016;17:370-395.
3. Cibas ES, Ali SZ. The 2017 Bethesda system for reporting thyroid cytopathology. Thyroid 2017;27:1341-1346.
4. Lee YJ, Kim DW, Park YM, Park HK, Jung SJ, Kim DH, Lee SM, Oh M. Comparison of sonographic and cytological diagnoses of solid thyroid nodules: emphasis on the discor-dant cases. Diagn Cytopathol 2015;43:953-959.
5. Yi KH, Lee EK, Kang HC, Koh Y, Kim SW, Kim IJ, Na DG, Nam KH, Park SY, Park JW, Bae SK, Baek SK, Baek JH, Lee BJ, Chung KW, Jung YS, Cheon GJ, Kim WB, Chung JH, Rho YS. 2016 Revised Korean Thyroid Association management guidelines for patients with thyroid nodules and thyroid Cancer. Int J Thyroidol 2016;9:59-126.
6. Haugen BR, Alexander EK, Bible KC, Doherty GM, Man-del SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Associa-tion management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016;26:1-133. 7. Moon WJ, Na DG, Jung SL, Lee JH, Kim HS.
Recommen-dations for ultrasound-based management of thyroid nodules. Seoul: Korean Radiological Society; 2006.
8. Cibas ES, Ali SZ; NCI Thyroid FNA State of the Science Conference. The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol 2009;132:658-665.
9. Bongiovanni M, Spitale A, Faquin WC, Mazzucchelli L, Baloch ZW. The Bethesda system for reporting thyroid cytopathology: a meta-analysis. Acta Cytol 2012;56:333-339.
10. Hwang SH, Sung JM, Kim EK, Moon HJ, Kwak JY. Imaging-cytology correlation of thyroid nodules with initially benign cytology. Int J Endocrinol 2014;2014:491508.
11. Kwak JY, Koo H, Youk JH, Kim MJ, Moon HJ, Son EJ, Kim EK. Value of US correlation of a thyroid nodule with initially benign cytologic results. Radiology 2010;254:292-300. 12. Kwak JY, Kim EK, Kim MJ, Hong SW, Choi SH, Son EJ, Oh
KK, Park CS, Chung WY, Kim KW. The role of ultrasound in thyroid nodules with a cytology reading of “suspicious for papillary thyroid carcinoma". Thyroid 2008;18:517-522. 13. Cho BY, Choi HS, Park YJ, Lim JA, Ahn HY, Lee EK, Kim
KW, Yi KH, Chung JK, Youn YK, Cho NH, Park DJ, Koh CS. Changes in the clinicopathological characteristics and out-comes of thyroid cancer in Korea over the past four decades. Thyroid 2013;23:797-804.
14. Choi YJ, Yun JS, Kim DH. Clinical and ultrasound features of cytology diagnosed follicular neoplasm. Endocr J 2009;56: 383-389.
15. Lee SH, Baek JS, Lee JY, Lim JA, Cho SY, Lee TH, Ku YH, Kim HI, Kim MJ. Predictive factors of malignancy in thyroid nodules with a cytological diagnosis of follicular neoplasm. Endocr Pathol 2013;24:177-183.
16. Hong AR, Lim JA, Kim TH, Choi HS, Yoo WS, Min HS, Won JK, Lee KE, Jung KC, Park DJ, Park YJ. The Frequency and Clinical Implications of the BRAF(V600E) Mutation in papillary thyroid cancer patients in Korea over the past two decades. Endocrinol Metab (Seoul) 2014;29:505-513. 17. Kim DS, Kim JH, Na DG, Park SH, Kim E, Chang KH,
Sohn CH, Choi YH. Sonographic features of follicular variant papillary thyroid carcinomas in comparison with conventional papillary thyroid carcinomas. J Ultrasound Med 2009;28:1685-1692.
18. Yang J, Schnadig V, Logrono R, Wasserman PG. Fine-needle aspiration of thyroid nodules: a study of 4703 patients with histologic and clinical correlations. Cancer 2007;111:306-315. 19. Kapan M, Onder A, Girgin S, Ulger BV, Firat U, Uslukaya O,
Oguz A. The reliability of fine-needle aspiration biopsy in terms of malignancy in patients with Hashimoto thyroiditis. Int Surg 2015;100:249-253.
20. Yi KI, Ahn S, Park DY, Lee JC, Lee BJ, Wang SG, Cha W. False-positive cytopathology results for papillary thyroid carcinoma: a trap for thyroid surgeons. Clin Otolaryngol 2017; 42:1153-1160.
21. Recavarren RA, Houser PM, Yang J. Potential pitfalls of needle tract effects on repeat thyroid fine-needle aspiration. Cancer Cytopathol 2013;121:155-161.
22. Trimboli P, Nasrollah N, Guidobaldi L, Taccogna S, Cicciarella Modica DD, Amendola S, Romanelli F, Lenzi A, Nigri G, Centanni M, Giovanella L, Valabrega S, Crescenzi A. The use of core needle biopsy as first-line in diagnosis of thyroid nodules reduces false negative and inconclusive data reported by fine-needle aspiration. World J Surg Oncol 2014;12:61.
23. Na DG, Kim DS, Kim SJ, Ryoo JW, Jung SL. Thyroid nodules with isolated macrocalcification: malignancy risk and diag-nostic efficacy of fine-needle aspiration and core needle biop-sy. Ultrasonography 2016;35:212-219.
24. Ha EJ, Baek JH, Lee JH, Song DE, Kim JK, Shong YK, Hong SJ. Sonographically suspicious thyroid nodules with initially benign cytologic results: the role of a core needle biopsy. Thyroid 2013;23:703-708.
25. Kim SY, Kim EK, Kwak JY, Moon HJ, Yoon JH. What to do with thyroid nodules showing benign cytology and BRAF(V600E) mutation? A study based on clinical and radiologic features using a highly sensitive analytic method. Surgery 2015;157:354-361.
26. Nikiforov YE, Ohori NP, Hodak SP, Carty SE, LeBeau SO, Ferris RL, Yip L, Seethala RR, Tublin ME, Stang MT, Coyne C, Johnson JT, Stewart AF, Nikiforova MN. Impact of mutational testing on the diagnosis and management of patients with cytologically indeterminate thyroid nodules: a prospective analysis of 1056 FNA samples. J Clin Endocrinol Metab 2011; 96:3390-3397.
27. Jara SM, Bhatnagar R, Guan H, Gocke CD, Ali SZ, Tufano RP. Utility of BRAF mutation detection in fine-needle aspiration biopsy samples read as “suspicious for papillary thyroid carcinoma”. Head Neck 2015;37:1788-1793.
28. Nikiforov YE, Steward DL, Robinson-Smith TM, Haugen BR, Klopper JP, Zhu Z, Fagin JA, Falciglia M, Weber K, Nikiforova MN. Molecular testing for mutations in improving the fine-needle aspiration diagnosis of thyroid nodules. J Clin Endocrinol Metab 2009;94:2092-2098.
29. Nam SJ, Kwak JY, Moon HJ, Yoon JH, Kim EK, Koo JS. Large (≥3cm) thyroid nodules with benign cytology: Can Thyroid Imaging Reporting and Data System (TIRADS) help predict false-negative cytology? PLoS One 2017;12:e0186242. 30. Moon HJ, Kim EK, Kim MJ, Kwak JY. Lymphocytic
thy-roiditis on fine-needle aspiration biopsy of focal thyroid nodules: approach to management. AJR Am J Roentgenol 2009;193:W345-W349.
31. Hwang S, Shin DY, Kim EK, Yang WI, Byun JW, Lee SJ, Kim G, Im SJ, Lee EJ. Focal lymphocytic thyroiditis nodules share the features of papillary thyroid cancer on ultrasound. Yonsei Med J 2015;56:1338-1344.
32. Chung SR, Baek JH, Park HS, Choi YJ, Sung TY, Song DE, Kim TY, Lee JH. Ultrasound-pathology discordant nodules on core-needle biopsy: malignancy risk and management strategy. Thyroid 2017;27:707-713.
33. Kim DW. Benign lesions that mimic thyroid malignancy on ultrasound. Can Assoc Radiol J 2015;66:79-85.
34. Koo JH, Shin JH, Han BK, Ko EY, Kang SS. Cystic thyroid nodules after aspiration mimicking malignancy: sonographic characteristics. J Ultrasound Med 2010;29:1415-1421. 35. Park NH, Kim DW, Park HJ, Lee EJ, Park JS, Park SI, Bae JM,
malignancy during sonographic follow-up. J Clin Ultrasound 2011;39:441-446.
36. Ha EJ, Baek JH, Lee JH, Lee HY, Song DE, Kim JK, Shong YK, Hong SJ. A focal marked hypoechogenicity within an isoechoic thyroid nodule: is it a focal malignancy or not? Acta Radiol 2015;56:814-819.
37. Hatada T, Okada K, Ishii H, Ichii S, Utsunomiya J. Evaluation of ultrasound-guided fine-needle aspiration biopsy for thyroid nodules. Am J Surg 1998;175:133-136.
38. Ha EJ, Baek JH, Lee JH, Kim JK, Kim JK, Lim HK, Song DE, Sung TY, Kim TY, Kim WB, Shong YK. Core needle biopsy can minimise the non-diagnostic results and need for diagnostic surgery in patients with calcified thyroid nodules. Eur Radiol 2014;24:1403-1409.
39. Hong MJ, Na DG, Baek JH, Sung JY, Kim JH. Cytology-ultra-sonography risk-stratification scoring system based on fine-needle aspiration cytology and the Korean-thyroid imaging reporting and data system. Thyroid 2017;27:953-959.
Peer Reviewers’ Commentary
본 논문은 갑상선결절의 진단에서 상호보완적인 갑상선초음파 와 미세침흡인결과가 일치하지 않는 다양한 상황과 그 해결법 을 국내에서 제정된 갑상선결절 진료권고안을 기반으로 다양 한 논문을 검토하여 체계적으로 잘 기술하고 있다. 암을 시사 하는 초음파 소견들은 갑상선유두암에 근거하고 있어 여포조 직으로 구성된 여포암, 여포변종 갑상선유두암에서 오류가 발 생할 수 있음을 강조하였고, 염증성 질환, 그리고 양성결절의 석 회화 혹은 섬유화와 같은 이차적인 변화가 초음파에서 암으로 해석될 수 있음을 잘 설명하였다. 미세침흡인검사 재검, 중심바 늘생검, 그리고 분자표지자 검사 등 해결책에 대한 언급은 혼란 스러운 상황에 놓인 임상가들에게 실제적 도움을 주는 좋은 지 침이라 생각한다. [정리: 편집위원회]