즉시 부하 시, 임플란트 디자인이
주위 골의 응력 분포에 미치는 영향:
3차원적 유한 요소 분석
연세대학교 대학원
치의학과
배정윤
즉시 부하 시, 임플란트 디자인이
주위 골의 응력 분포에 미치는 영향:
3차원적 유한 요소 분석
지도 한종현 교수
이 논문을 박사 학위논문으로 제출함
2009 년 7 월 일
연세대학교 대학원
치의학과
배정윤
감사의 글
논문을 마무리하는 시점에 와서 지나간 시간을 뒤돌아보며, 처음 시작할 때의 의욕과 열정이 얼마나 남아있나 생각해보면, 많이 부끄러워집니다. 그러나, 저의 주위에 많은 분들이 있었기에 여기까지 올 수 있었던 것 같습니다. 이 논문이 완성되는데 있어 부족한 저에게 처음부터 지금까지 끊임 없는 가르 침을 주시고, 격려를 보내주신 한종현 교수님께 진심으로 감사 드립니다. 그리고, 바쁘신 와중에도 귀중한 조언을 해 주시고, 논문의 심사를 해 주신 심 준성 교수님, 류인철 교수님, 허성주 교수님, 김선재 교수님께도 감사를 드립니다. 또한, 이 논문의 실험을 도와주시고, 많은 조언을 아끼지 않으신 전흥재 교수님 과 강경탁, 주민진 선생님에게도 마음 깊이 감사를 드립니다. 논문을 준비하는 동안 힘들 때마다 옆에서 많은 도움이 되어 준 분당 제생 병 원 치과 선생님들과 저의 지인들에게도 감사의 마음을 전합니다. 그리고, 제가 여기에 있게 해주신 사랑하는 아버지, 어머니, 항상 격려해주시는 오빠와 언니에게도 감사의 마음을 표합니다. 2009년 7월 배정윤 드림i
차 례
그림 및 표 차례 ··· ⅱ 국문 요약 ··· ⅴ I. 서론 ··· 1 II. 재료 및 방법 ··· 4 1. 유한 요소 모델링 ··· 4 2. 임플란트-골 계면 디자인 ··· 5 3. 경계, 하중 조건과 물질의 성질 ··· 5 III. 연구 결과 ··· 8 1. 지연 부하에서 임플란트 길이, 직경, 바디 형태에 따른 골 최대 응력 변화 ··· 10 2. 즉시 부하에서 임플란트 길이, 직경, 바디 형태에 따른 골 최대 응력과 변위 변화 ··· 15 IV. 총괄 및 고찰 ··· 21 V. 결론 ··· 28 참고 문헌 ··· 30 영문 요약 ··· 39ii
그림 차례
Fig.1. The 3-dimensional model including the crown, the implant. ··· 7 Fig.2. Schematic presentation of a) tapered type b) straight type dental implant.
··· 7 Fig.3. The distribution of cortical & trabecular bone stresses around a) delayed loaded (bonded) implants and b) immediately loaded (contact) implants ··· 8 Fig.4. The distribution of cortical & trabecular bone stresses around a) tapered, b) straight 4.3 X 8.5, 4.3 X 10 and 4.3 X 11.5 mm delayed loaded (bonded) implants. ··· 11 Fig.5. The distribution of cortical & trabecular bone stresses around a) tapered, b) straight 5.3 X 8.5, 5.3 X 10 and 5.3 X 11.5 mm delayed loaded (bonded) implants. ··· 12 Fig.6. The maximum von-Mises stress (EQV) of the bone among three implant length (8, 10, 11.5 mm) of diameter 4.3 mm and 5.3 mm delayed loaded (bonded) a) tapered and b) straight implants. ··· 13 Fig.7. The maximum von-Mises stress (EQV) of the bone among two implant diameter (4.3, 5.3mm) of length 8.5 mm, 10 mm, and 11.5 mm delayed loaded (bonded ) a) tapered and b) straight implants. ··· 13 Fig.8. The maximum von-Mises stress (EQV) of the bone among two implant body designs (tapered, straight form) of length 8.5 mm, 10 mm, and 11.5 mm delayed loaded (bonded ) a) diameter 4.3 mm and b) 5.3 mm implants. ··· 14
iii
Fig.9. The distribution of cortical & trabecular bone stresses around a) tapered, b) straight 4.3 X 8.5, 4.3 X 10 and 4.3 X 11.5 mm immediately loaded (contact) implants. ··· 17 Fig.10. The distribution of cortical & trabecular bone stresses around a) tapered, b) straight 5.3 x 8.5, 5.3 X 10 and 5.3 x 11.5 mm immediately loaded (contact) implants. ··· 18 Fig.11. The maximum von-Mises stress (EQV) of the bone among three implant length (8, 10, 11.5 mm) of diameter 4.3 mm and 5.3 mm immediately loaded (contact) a) tapered and b) straight implants. ··· 19 Fig.12. The maximum von-Mises stress (EQV) of the bone among two implant diameter (4.3, 5.3 mm) of length 8.5 mm, 10 mm, and 11.5 mm immediately loaded (contact) a) tapered and b) straight implants. ···· 19 Fig.13. The maximum von-Mises stress (EQV) of the bone among two implant body designs (tapered, straight form) of length 8.5 mm, 10 mm, and 11.5 mm immediately loaded (contact) a) diameter 4.3 mm and b) 5.3 mm implants. ··· 20
iv
표 차례
Table I. Mechanical properties of the materials. ··· 6 Table II. The maximum von-Mises stress (maximum equivalent stress or Max EQV stress) of the bone around different implant length, diameter and body design (tapered and straight) with bonded and contact interface condition. ··· 9 Table III. The maximum sliding distance of model of contact implant-bone interfaces. ··· 20
v 국문 요약
즉시 부하 시, 임플란트 디자인이
주위 골의 응력 분포에 미치는 영향: 3차원적 유한 요소 분석
최근에는 임플란트를 식립한 후 보철물을 장착하기까지 소요하는 치유 기간을 점차 줄이고 있는 추세이며, 심지어는 치유 기간 없이 바로 기능 부하를 가하는 즉시 부하 치료도 많이 시행하는 추세이다. 이러한 즉시 부하의 성공에 가장 중요한 요소는 임플란트의 초기 안정성이며, 즉시 부하 결과에 영향을 주는 요인들 중 임플란트 디자인 요인들의 변화에 의해서 교합압을 적용할 때 골에서 지지하는 표면적을 늘일 수 있어, 발생하는 응력을 감소시킬 수 있다. 임플란트의 즉시 부하에서 이들의 영향은 최근에 연구하기 시작했으며, 지연 부하 시와 비교해서 다른 영향을 미칠 수 있을 것이다. 이번 연구의 목적은 임플란트의 즉시 부하 상황을 유한 요소 방법으로 재현하고, 임플란트 주위 골의 응력 분포에 대한 임플란트의 디자인의 영향을 분석하여, 즉시 부하 시술을 위한 적절한 임플란트 선택에 도움을 주기 위함이다. 실험 방법은 유한 요소 분석 방법을 선택했으며, 임플란트로 지지하는 하악 제 1 소구치 치관을 3차원적 모델로 재현하였다. Tapered, straight 형의, 4.3 mm의 직경과 8, 10, 11.5 mm의 길이를 가진 임플란트들과 5.3mm의 직경과 8, 10, 11.5 mm의 길이를 가진 임플란트들을 즉시 부하와 지연 부하 상황에 놓이게 하여, 등가 응력을 분석했다. 임플란트의 즉시 부하 시 임플란트 디자인이 주위 골의 응력 분포에 미치는 영향을 연구한 결과는 다음과 같다.vi 1. 지연 부하와 비교해서 즉시 부하에서는 응력이 임플란트 경부 피질골 뿐만 아니라, 임플란트-골 계면을 따라 임플란트 근단까지 해면골에도 광범위하게 분포하며, 최대 등가 응력도 더 높게 나타났다. 2. 지연 부하에서는 tapered 형 직경 4.3 mm 의 임플란트 모델이 10 mm 에서 11.5 mm 로 길이가 증가할 때 최대 응력이 다소 증가하는 양상을 보인 것을 제외하고는, 임플란트의 길이가 길어질수록 최대 응력이 감소했다. 또한 임플란트 직경이 커지면 최대 응력이 감소했으며, tapered 형 임플란트가 straight 형 임플란트보다 최대 응력이 더 높았다. 3. 즉시 부하에서는 tapered 형의 임플란트에서는, 같은 직경일 때 길이가 8.5 mm 에서 10 mm 로 증가 시에는 최대 응력이 감소하나, 10 mm 에서 11.5 mm 로 증가 시에는 최대 응력이 증가했으며, 같은 길이일 때는 직경이 증가할수록 최대 응력이 감소했다. 바디 형태에서는 4.3 X 8.5 mm 의 임플란트 모델을 제외하고, tapered 형 임플란트가 straight 형 임플란트보다 최대 응력이 더 낮게 나타났다. 즉시 부하 시 임플란트-골 계면의 최대 변위 거리는 허용되는 미세동요도인 50 μm 이하의 값을 나타냄으로써, 골형성을 방해하지 않는 것으로 보인다. 4. 지연 부하에서는 길이, 직경, 바디 형태들의 변화에 따른 최대 응력에 대한 영향이 비교적 규칙적인 양상을 보였으나, 즉시 부하에서는 이들의 영향이 다양하게 나타나는 모습을 보여주었다. 즉 지연 부하에서의 디자인 변수들의 영향과 일치하지 않을 수 있다는 것을 보여주었다. --- 핵심되는 말: 즉시 부하, 유한 요소 분석, 치과 임플란트, 길이, 직경, 디자인, 응력
- 1 -
I. 서 론
임플란트를 Brånemark이 처음 임상에 도입했을 때, 성공적인 골유착을 위해서는 임플란트를 치은 하방에 위치시킨 후 부하를 가하지 않는 3-6개월의 치유 기간이 필요하다고 제시했다. 1-2 그러나, 최근 임플란트를 식립한 후 보철물을 장착하기까지 소요하는 치유 기간을 점차 줄이고 있는 추세이며, 심지어는 치유 기간 없이 바로 기능 부하를 가하는 즉시 부하에 대한 연구도 보고되고 있다. 3-6 즉시 임플란트 부하란 임플란트를 식립한 후 즉시 또는 몇 시간 후 부하를 가하는 것으로 정의 할 수 있다. 7 최근에 Wang 등 8 은 즉시 부하의 정의를 임플란트를 식립한 후 적어도 48시간 내에, 임플란트 지지 수복물에 교합력을 가하는 것으로 제안했다. 이러한 즉시 부하는 환자에게 내원 기간 단축, 빠른 저작 기능과 심미성의 회복 등으로 편안함을 제공해 주지만, 임플란트의 미세동요로 인한 더 높은 실패율, 최종 결과 예측의 불확실성 등을 포함하는 많은 위험성을 가지고 있다. 7 초기 즉 1970년대의 임플란트의 즉시 부하는 섬유 피막화, 동요, 최종적으로 임플란트의 소실로 이어졌다. 9-12 최근 10년 동안 환자의 조심스런 선택, 교합과 보철물 설계의 적절한 계획, 임플란트 재료와 표면, 디자인의 개선으로 성공률이 높아짐에 따라 즉시 부하 치료는 점차 확대되어 가고 있는 추세이다. 7 통계상으로도 96% 이상의 성공률을 보고하고 있고, 골흡수에서도 지연 부하와 즉시 부하 간에 큰 차이를 보이지 않고 있다. 14-19 이와 같이 다수의 임상 연구는 진행되었으나, 즉시 부하 프로토콜에 대한- 2 - 연구와 즉시 부하의 근거가 될만한 임상 연구는 부족한 형편이다. 13 이러한 즉시 부하의 성공에 가장 중요한 요소는 임플란트의 초기 안정성으로서, 골유착을 위해서는 기간이 아니라, 교합압을 전달할 때 골과 임플란트 계면 사이에 발생되는 미세동요가 대략 50-150 μm 정도의, 수용 가능한 역치 이하에 존재하도록 하는 것이 필요하다. 이를 위해서 Gapski 등 20 은 즉시 부하 결과에 영향을 주는 요인들을 수술 시 초기 임플란트 안정성, 환자의 골량과 골질, 임플란트 디자인, 교합과 보철물 디자인 등 이라고 했다. 이중에서 임플란트 디자인 요인으로는 임플란트 길이, 직경, 바디 형태 등이 있으며, 이들을 적절하게 선택함에 의해 교합압을 작용할 때 골에서 지지하는 표면적을 늘일 수 있어 발생하는 응력을 감소시킬 수 있다. 21 바디 형태 중 현재 가장 대표적인 디자인으로는 tapered 형과 straight 형이 있다. 이런 디자인 요인들은 지연 부하에서도 폭넓게 연구하여 왔으며, 이들의 변화에 의해 임플란트 치료의 성공률을 높일 수 있다는 것을 발견했다. 22-25 그러나, 임플란트의 즉시 부하에서 이들의 영향은 최근에 연구하기 시작했으며, 또한 지연 부하 시와 비교해서 다른 영향을 미칠 수도 있을 것이다. 26-28 즉시 부하에 영향을 주는 변수들과 골에서 발생하는 응력과의 상관 관계를 좀더 상세하게 밝히기 위한 연구 방법 중의 하나가 유한 요소 분석법이다. 유한 요소 분석은 지난 2세기 동안 임플란트 주위 골의 응력의 예측을 위한 유용한 방법으로 이용해왔으며, 29 즉시 부하 상황을 유한 요소 방법으로 재현한 연구도 몇몇 논문에서 볼 수 있다. 30-33 Riger 등 31과 Palomar 등 32 은 완전한 골 유착 전에는 임플란트-골 계면에서 전면적인 활주 운동이 일어난다고 생각했으므로, frictionless interface(마찰이
- 3 - 없는 계면)으로 재현했다. 그러나, Mellal 등 33 은 치유 기간 동안 특정한 순간을 대표하는 마찰 계수를 임플란트-골 계면에서 추정할 수 있으므로, 골 유착 전 계면을 임플란트와 골 사이의 작은 변위를 허락하는 마찰 계면으로, 비선형 frictional contact(마찰 접촉) 요소를 사용하여 재현했다. 이번 연구에서는 즉시 부하 시 임플란트-골 계면을 후자와 같이 재현하였다. 이번 연구의 목적은 임플란트의 즉시 부하 상황을 유한 요소 방법으로 재현하고, 임플란트 주위 골의 응력 분포에 대한 임플란트의 디자인의 영향을 분석하여, 즉시 부하 시술을 위한 적절한 임플란트 선택에 도움을 주기 위함이다.
- 4 -
II. 재료 및 방법
1.
유한 요소 모델링
실험 단계는 Pro/Engineer Wildfire 2.0으로 모델링하고, Hypermesh 8.0 (Altair Co., USA)으로 preprocessing, postprocessing 한 후, ABAQUS 6.6 (HKS, Inc.)으로 해석하였다.
임플란트로 지지하는 하악 제 1 소구치 치관을 3차원적 모델로 재현하였다. 치관은 castable abutment (warantec, Seoul, Korea)로 제작한 시멘트 유지형 금관이며, 지대주의 높이는 5 mm로 하였다. 임플란트 주위의 골은, Lekholm와 Zarb 34 의 분류 중 type 2 골을 참고로 해서, 2mm 두께의 피질골 하방에 조밀한 해면골로 구성된 하악골로 3차원적으로 형성했다 (Fig.1). 골의 높이는 23.4mm 직경은 16mm로 하였다.
임플란트는 tapered, straight 형의 내부 연결형의 임플란트 (Oneplant, warantec, Seoul, Korea)를 모델로 하였다 (Fig.2). 4.3 mm의 직경과 8, 10, 11.5 mm의 길이를 가진 임플란트들과 5.3mm의 직경과 8, 10, 11.5 mm의 길이를 가진 임플란트들을 즉시 부하와 지연 부하 상황에 놓이게 했다.
요소는 C3D10m (A 10-node modified quadratic tetrahedron), C3D4 (A 4-node linear tetrahedron)를 사용하였다. 요소 크기는 임플란트는 0.5, 골은 0.4로 하였다.
- 5 -
2.
임플란트-골 계면 디자인
임플란트의 즉시 부하와 지연 부하의 상황은 골과 임플란트 사이 계면에서의 서로 다른 상황을 추정해서 재현했다. 즉 즉시 부하시의 골-임플란트 계면은 임플란트와 골 사이 마찰이 있는 마찰 접촉 상황으로, 지연 부하시의 계면은 임플란트와 골이 완전히 고정된 결합으로 재현했다. 전자의 구조는 비선형 마찰 접촉 요소를 사용하여 재현하였으며, 임플란트와 골 사이의 약간의 변위를 허용한다. 33 골-임플란트 간 마찰계수는 0.3 으로 추정하였다. 35,363.
경계, 하중 조건과 물질의 성질
골조직 주위로 움직임이 전혀 발생하지 않는다고 가정하여, 골의 바깥쪽 가장 자리를 완전 구속하였고, 하중은 치관의 장축 방향으로 110N의 수직 부하를 가했다. 37 유한 요소 분석 결과는 von-Mises stress(등가 응력)으로 계산하였으며, 상대적인 비교의 편리성을 도모하기 위해 계산된 등가 응력을 특정한 값으로 선정하여 색상으로 표시하였다. 등가 응력은 연성 물질에 대한 항복 기준을 평가하기 위한 것으로, 2차원 또는 3차원에서의 스트레스들을 결합함에 의해 계산되며, 유한 요소 분석 결과는 전형적으로 등가 응력으로 나타낸다. 그리고, 즉시 부하 시 임플란트-골 계면에서의 최대 변위 거리도 해석하였다. 본 연구에 사용된 임플란트, 피질골, 해면골, 금관은 등방성, 동질성, 선형 탄성 재료로 가정하였다. 상대적인 기계적 성질은 물질에 따라 달라지며, 유한 요소 분석으로 실험한 기존의 논문과 제조회사 자료에 기초를 두고 결정하었다. 13- 6 -
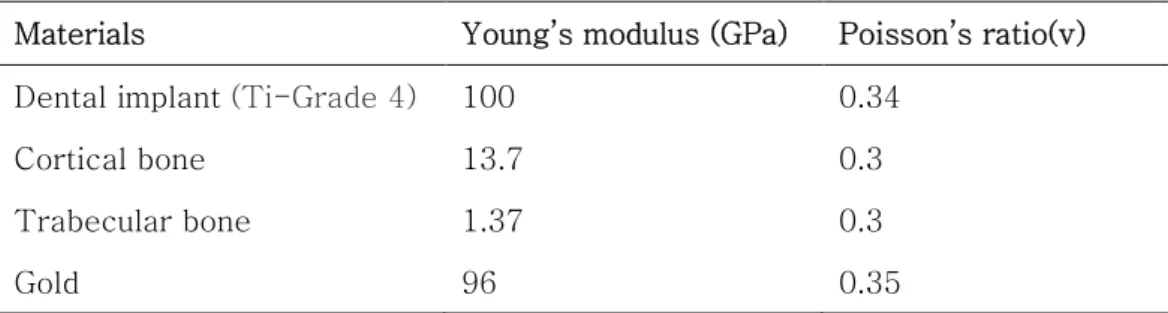
구조적 분석에서 요구되는 물리적 성질은 Young’s modulus와 Poisson’s ratio이었다 (Table I).
Table I. Mechanical properties of the materials.
Materials Young’s modulus (GPa) Poisson’s ratio(v) Dental implant (Ti-Grade 4) 100 0.34
Cortical bone 13.7 0.3
Trabecular bone 1.37 0.3
- 7 -
Fig.1. The 3-dimensional model including the crown, the implant.
a) b)
Fig.2. Schematic presentation of a) tapered type and b) straight type dental implant.
- 8 -
III. 연구 결과
골의 응력 분포 형상을 보면, 지연 부하에 비해 즉시 부하 시 응력이 임플란트 경부 피질골뿐만 아니라 해면골에서 임플란트-골 계면을 따라 임플란트 근단까지 더 광범위하게 분포하는 것을 보여준다 (Fig.3). 또한 최대 등가 응력은 지연 부하에 비해 즉시 부하에서 더 높으며, 지연 부하 시는 해면골보다 피질골에서 더 높으며, 즉시 부하에서도 tapered 형 4.3 X 10 mm, 4.3 X 11.5 mm, straight 형 4.3 X 8.5 mm 임플란트 모델들을 제외하고는 피 질골에서 더 높았다 (Table II). a) b)Fig.3. The distribution of cortical & trabecular bone stresses around a) delayed loaded (bonded) implants and b) immediately loaded (contact) implants
- 9 -
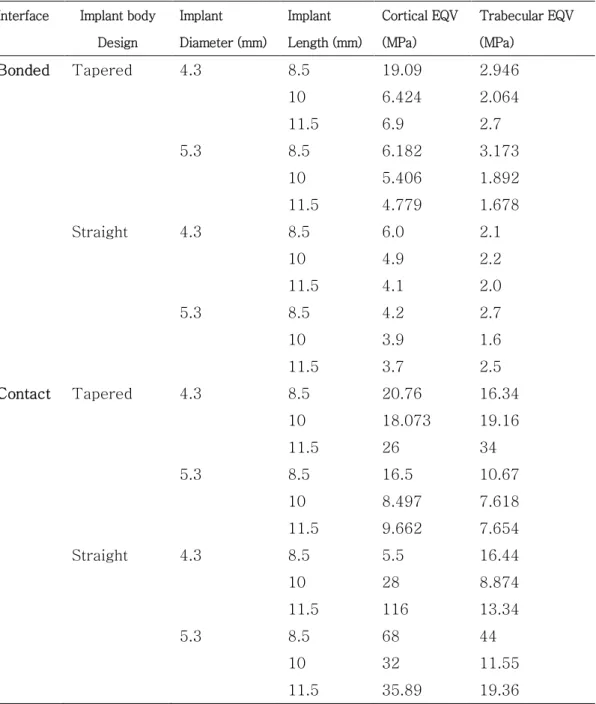
Table II. The maximum von-Mises stress (maximum equivalent stress or Max EQV stress) of the bone around different implant length, diameter and body design (tapered and straight) with bonded and contact interface condition.
Interface Implant body Design Implant Diameter (mm) Implant Length (mm) Cortical EQV (MPa) Trabecular EQV (MPa) Bonded Tapered 4.3 8.5 19.09 2.946 10 6.424 2.064 11.5 6.9 2.7 5.3 8.5 6.182 3.173 10 5.406 1.892 11.5 4.779 1.678 Straight 4.3 8.5 6.0 2.1 10 4.9 2.2 11.5 4.1 2.0 5.3 8.5 4.2 2.7 10 3.9 1.6 11.5 3.7 2.5 Contact Tapered 4.3 8.5 20.76 16.34 10 18.073 19.16 11.5 26 34 5.3 8.5 16.5 10.67 10 8.497 7.618 11.5 9.662 7.654 Straight 4.3 8.5 5.5 16.44 10 28 8.874 11.5 116 13.34 5.3 8.5 68 44 10 32 11.55 11.5 35.89 19.36
- 10 -
1.
지연 부하에서 임플란트 길이, 직경, 바디 형태에 따른 골 최대
응력 변화
지연 부하에서는 tapered 형 4.3 X 8.5 mm 임플란트 모델이 다른 모델보다 더 높은 최대 등가 응력을 보였다. 반면 straight 형 5.3 X 11.5 mm 임플란트 모델이 다른 모델보다 더 낮은 최대 등가 응력을 보였다 (Fig.6). 지연 부하에서는 tapered 형 직경 4.3 mm의 임플란트 모델들은 길이가 8.5 mm에서 10 mm로 증가 시에는 최대 응력이 감소하나, 10 mm에서 11.5 mm로 증 가 시 7.4% 증가한 것을 제외하고는, 같은 직경과 바디 형태일 때 길이가 길어질 수록 최대 응력이 감소하였다 (Fig.6). 특히 Tapered 형 직경 4.3 mm의 임플란트에서 길이가 8.5 mm에서 10 mm로 증가 시 최대 응력이 66.3%만큼 감소했다. 한편 같은 바디 형태와 길이를 가진 임플란트 모델들에서는 직경이 커지면 최 대 응력이 감소하였다 (Fig.7). 그리고, 같은 직경과 길이를 가진 임플란트 모델들 에서는 tapered 형이 straight 형보다 최대 응력 값이 더 높았다 (Fig.8).- 11 - a)
4.3 X 8.5 4.3 x 10 4.3 X 11.5 b)
4.3 X 8.5 4.3 X 10 4.3 X 11.5
Fig.4. The distribution of cortical & trabecular bone stresses around a) tapered, b) straight 4.3 X 8.5, 4.3 X 10 and 4.3 X 11.5 mm delayed loaded (bonded) implants.
- 12 - a)
5.3 X 8.5 5.3 X 10 5.3 X 11.5 b)
5.3 X 8.5 5.3 X10 5.3 X 11.5
Fig.5. The distribution of cortical & trabecular bone stresses around a) tapered, b) straight 5.3 X 8.5, 5.3 X 10 and 5.3 X 11.5 mm delayed loaded (bonded) implants.
- 13 - 0 5 10 15 20 8.5 10 11.5 Implant Length E Q V (M P a ) 4.3 5.3 a) b)
Fig.6. The maximum von-Mises stress (EQV) of the bone among three implant length (8, 10, 11.5 mm) of diameter 4.3 mm and 5.3 mm delayed loaded (bonded) a) tapered and b) straight implants.
0 5 10 15 20 4.3 5.3 Implant Diameter E Q V (M P a ) 8.5 10 11.5 a) b)
Fig.7. The maximum von-Mises stress (EQV) of the bone among two implant diameter (4.3, 5.3 mm) of length 8.5 mm, 10 mm, and 11.5 mm delayed loaded (bonded ) a) tapered and b) straight implants.
0 5 10 15 20 8.5 10 11.5 Implant Length E Q V (M P a ) 4.3 5.3 0 5 10 15 20 4.3 5.3 Implant Diameter E Q V (M P a ) 8.5 10 11.5
- 14 - 0 5 10 15 20 Tapered Straight Implant Designs E Q V (M P a ) 8.5 10 11.5 a) b)
Fig.8. The maximum von-Mises stress(EQV) of the bone among two implant body designs (tapered, straight form) of length 8.5 mm, 10 mm, and 11.5 mm delayed loaded (bonded ) a) diameter 4.3mm and b) 5.3mm implants.
0 5 10 15 20 Tapered Straight Implant Designs E Q V (M P a ) 8.5 10 11.5
- 15 -
2.
즉시 부하에서 임플란트 길이, 직경, 바디 형태에 따른 골 최대
응력과 변위 변화
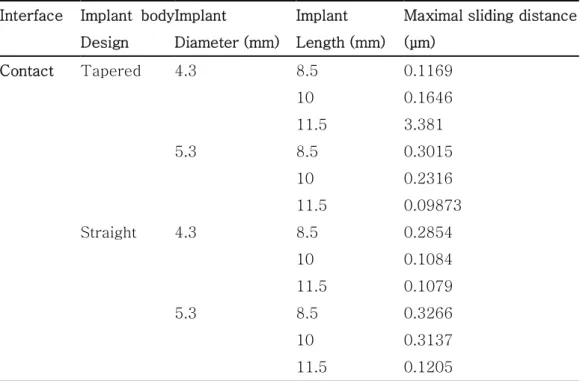
즉시 부하에서는 straight 형 4.3 X 11.5 mm 모델이 다른 모델보다 더 높은 최 대 등가 응력을 보였다. 반면 tapered 형 5.3 X 10 mm 모델이 다른 모델보다 더 낮은 최대 등가 응력을 보였다 (Fig.11). Straight 형 직경 4.3 mm 임플란트 모델들을 제외하고는, 같은 직경과 같은 바 디 형태일 때 8.5 mm에서 10 mm로 증가 시에는 최대 응력이 감소하나, 10 mm 에서 11.5 mm로 증가 시에는 최대 응력이 증가하였으며, 10 mm의 길이일 때, 가 장 낮은 최대 응력을 보였다. 따라서 tapered 형의 임플란트에서는 같은 직경일 때 길이가 8.5 mm에서 10 mm로 증가 시에는 최대 응력이 감소하나, 10 mm에서 11.5 mm로 증가 시에는 최대 응력이 증가하였다 (Fig.11). 즉 tapered 형 직경 5.3 mm 임플란트 모델들에서 길이가 8.5 mm에서 10 mm 로 증가 시 최대 응력이 48.5%만큼 감소했으며, straight 형 직경 5.3 mm 임플란 트 모델에서는 최대 응력이 53%만큼 감소했다. 반면 tapered 형 직경 4.3 mm 임플란트 모델에서 길이가 10 mm에서 11.5 mm로 증가 시 최대 응력이 77.5%만 큼 증가했다. 그러나, straight 형 직경 4.3 mm 임플란트 모델들에서는 길이가 길어질수록 최 대 응력이 증가하였다. 8.5 mm에서 10 mm 로 증가 시엔 70%, 특히 10 mm 에서 11.5 mm 증가 시엔 314% 증가했다 (Fig.11). Straight 형 길이 8.5, 10 mm 임플란트 모델들을 제외하고는, 같은 바디 형태 와 길이를 가진 임플란트 모델들에서는 직경이 증가할수록 최대 응력이 감소했다- 16 - (Fig.12). Straight 형 길이 8.5, 10 mm 임플란트 모델들에서는 직경이 4.3 mm에서 5.3 mm로 증가 시 최대 응력이 각각 313%, 14% 증가했다. 4.3 X 8.5 mm의 임플란트 모델을 제외하고, 같은 직경과 길이일 때, tapered 형 이 straight 형보다 최대 응력이 더 낮았다 (Fig.13). 한편, 즉시 부하 시 임플란트-골 계면의 최대 변위 거리는, tapered 형 4.3 X 11.5 mm 모델이 다른 모델보다 더 높은 값을 보인 반면 tapered 형 5.3 X 11.5 mm 모델이 다른 모델보다 더 낮은 값을 보였다 (Table III). Tapered 형 직경 4.3 mm 임플란트 모델들을 제외하고는, 같은 직경과 같은 바디 형태를 가진 임플란트 모델들에서는 길이가 증가 시에 최대 변위 거리가 감소했다. Tapered 형의 길이 11.5 mm 임플란트 모델들을 제외하고는 같은 바디 형태와 길 이를 가진 임플란트 모델들에서는 직경이 감소할수록 최대 변위 거리가 감소했다. 4.3 X 10 mm, 4.3 X 11.5 mm의 임플란트 모델을 제외하고, 같은 직경과 길이일 때, tapered 형이 straight 형보다 최대 변위 거리가 더 낮았다 (Table III).
- 17 - a)
4.3 X 8.5 4.3 X 10 4.3 X 11.5
b)
4.3 X 8.5 4.3 X 10 4.3 X 11.5
Fig.9. The distribution of cortical & trabecular bone stresses around a) tapered, b) straight 4.3 X 8.5, 4.3 X 10 and 4.3 X 11.5 mm immediately loaded (contact) implants.
- 18 - a)
5.3 X 8.5 5.3 X 10 5.3 X 11.5
b)
5.3 X 8.5 5.3 X 10 5.3 X 11.5
Fig.10. The distribution of cortical & trabecular bone stresses around
a) tapered, b) straight 5.3 x 8.5, 5.3 X 10 and 5.3 x 11.5 mm immediately loaded (contact) implants.
- 19 - a) b)
Fig.11. The maximum von-Mises stress (EQV) of the bone among three implant length (8, 10, 11.5 mm) of diameter 4.3 mm and 5.3 mm immediately loaded (contact) a) tapered and b) straight implants.
a) b)
Fig.12. The maximum von-Mises stress (EQV) of the bone among two implant diameter (4.3, 5.3 mm) of length 8.5 mm, 10 mm, and 11.5 mm immediately loaded (contact) a) tapered and b) straight implants.
0 20 40 60 80 100 120 8.5 10 11.5 Implant length E Q V (M P a ) 4.3 5.3 0 20 40 60 80 100 120 8.5 10 11.5 Implant length E Q V (M P a ) 4.3 5.3 0 20 40 60 80 100 120 4.3 5.3 Implant Diameter E Q V (M P a ) 8.5 10 11.5 0 20 40 60 80 100 120 4.3 5.3 Implant Diameter E Q V (M P a ) 8.5 10 11.5
- 20 - 0 20 40 60 80 100 120 Tapered Straight Implant Designs E Q V (M P a ) 8.5 10 11.5 a) b)
Fig. 13. The maximum von-Mises stress (EQV) of the bone among two implant body designs (tapered, straight form) of length 8.5mm, 10mm, and 11.5mm immediately loaded (contact) a) diameter 4.3mm and b) 5.3mm implants.
Table III. The maximum sliding distance of model of contact implant-bone interfaces.
Interface Implant body Design
Implant Diameter (mm)
Implant Length (mm)
Maximal sliding distance (μm) Contact Tapered 4.3 8.5 0.1169 10 0.1646 11.5 3.381 5.3 8.5 0.3015 10 0.2316 11.5 0.09873 Straight 4.3 8.5 0.2854 10 0.1084 11.5 0.1079 5.3 8.5 0.3266 10 0.3137 11.5 0.1205 0 20 40 60 80 100 120 Tapered Straight Implant Designs E Q V (M P a ) 8.5 10 11.5
- 21 -
IV. 총괄 및 고찰
지연 부하에서는 이전의 연구 결과와 같이, 본 연구에서도 부하 시 응력이 주로 임플란트 경부 피질골에 집중되어 분포했다. 38 그러나, 지연 부하 시와 비교해서 즉시 부하에서는 응력이 피질골 뿐만 아니라, 임플란트-골 계면을 따라 임플란트 근단까지 해면골에도 광범위하게 분포했다. 또한, 최대 응력도 즉시 부하에서 더 높게 나타났다. 이것은 전의 실험 결과들 28, 39 과 일치한다. 이같이 지연 부하에 비해 더 높은 골 응력이 발생하는 즉시 부하의 성공을 위해서는 적절한 임플란트의 선택을 통하여 골 응력을 줄이는 것이 필요할 것이다. 따라서 본 연구는 즉시 부하 시술을 위한 적절한 임플란트 선택에 도움을 주기 위해, 즉시 부하 상황에서 골 응력 분포에 대한 임플란트 디자인의 영향을 유한 요소 분석을 이용하여 연구했다. 즉시 부하 시 임플란트-골 계면은 임플란트의 식립 즉시 골이 직접적으로 임플란트 표면과 접촉하여, ‘일차 골 접촉’을 이루며, 시간이 지남에 따라 골조직이 리모델링되어, 이 부위도 새로운 골로 대체되어, ‘이차 골 형성’이 일어난다. 40 Berglundh 등 41에 의하면 개에서 임플란트를 식립 후 두 시간 후의 ground section을 보면, 임플란트가 골과 밀접하게 접촉하고 있으며, 초기에 빈 wound chamber 는 육아 조직과 혈병으로 이루어져 있다. 즉시 부하 시의 임플란트-골 계면은 전 과정을 유한 요소 방법으로 재현하기 어려우므로, 이러한 식립 초기 같은 특정한 순간을 재현하여, 임프란트와 골 사이에 작은 변위를 허락하는 마찰 계면으로 재현하기로 했다. 이차 골형성이- 22 - 일어나면서부터는 지연 부하 시와 비슷한 상황에 놓이기 때문이다. 골-임플란트 접촉의 물리적 모델은 마찰이 없는 접촉, 마찰 접촉 등이 있으며, 가장 간단한 모델은 마찰이 없는 접촉이고, 마찰 접촉은 더 복잡한 재현을 하며, 비가역적이며, 경로-의존적이다. 42 이런 마찰 접촉 계면을 설명하는 면 대 면 모델이 정형외과에서 발달해왔으며, 치과 임플란트에도 동일하게 적용된다. 마찰 운동은 Elastic Coulomb 마찰 모델로 모델링되며, 42 금속과 골의 마찰 계수는 0.1-0.5 사이에 존재한다. 35 본 실험에서는 즉시 부하 상황을 재현하기 위한 임플란트-골 계면간의 마찰 계수를 임플란트 모델의 실제 값이 아닌, 기존의 연구들 35,36 에서 사용한 값을 이용하여, 마찰 접촉 모델로 재현했다. 0.3과 1사이에서 마찰 계수가 증가하더라도, 골 응력을 감소시키지는 않는다는 실험 결과가 있었다. 27, 28 지연 부하에서의 같은 바디 형태와 직경을 가진 임플란트의 길이의 변화에 따른 최대 등가 응력의 변화를 보면, tapered형 직경 4.3 mm의 임플란트 모델이 10 mm에서 11.5 mm로 길이 증가 시 최대 응력이 다소 증가하는 양상을 보인 것을 제외하고는, 전반적으로 같은 직경과 바디 형태일 때 길이가 길어질수록 최대 응력이 감소했다. 이것은 임플란트 길이가 길어질수록 골 응력이 감소한다는 전의 연구 결과들과 일치한다. 13, 22 임플란트의 증가된 길이는 초기 고정력과 임플란트-골 접촉 면적을 늘이므로 의미가 있다. 38 지연 부하에서의 직경에 대해 영향을 살펴보면, 같은 바디 형태와 길이를 가진 임플란트 모델들에서는 직경이 커지면 최대 응력이 감소했다. 이것은 기존의 연구 결과들 24, 25 과 일치하는 결과로서, 더 넓은 임플란트는 증가된 골 접촉부위
- 23 - 때문에 유사한 높이와 디자인을 가진 좁은 임플란트보다 더 큰 골 접촉부위를 가지므로, 38 더 호의적인 응력 분배가 이루어진다. 43또한, 임플란트에 가해지는 교합 하중의 대부분이 치조정에 가해지며, 이 치조정이 조기 골 소실이 일어나는 곳이므로, 초기 고정과 토크에 대한 최소 길이가 얻어졌다면 직경이 길이보다 더 중요하다. 38
바디 형태에 대해서는, Mailat, 43 Siegele and Soltesz, 44 Patra 등 45 의 연구 결과들과 같이 지연 부하에서 같은 길이와 직경을 가진 임플란트 모델들에서는 tapered 형 임플란트가 straight 형 임플란트보다 최대 응력이 더 높았다. Tapered 형 임플란트는 같은 길이, 너비, 나선 수의 평행형 나사 임플란트에 비해 전반적인 표면적이 더 적으며, 이 특징은 초기 고정을 감소시킬 수 있다. 21 한편, 즉시 부하에서 현재까지의 논문들을 고찰해보면, 직경 4 mm 이상, 길이 10 mm 이상의 tapered 형 나사 나선 디자인의 임플란트를 추천하고 있다. 7, 8, 46 즉시 부하 시 길이, 직경, 바디 형태에 따른 최대 등가 응력과 변위의 변화를 분석해 보았다. Straight 형 직경 4.3 mm 임플란트 모델들을 제외하고는, 같은 직경과 같은 바디 형태일 때 길이가 8.5 mm에서 10 mm로 증가 시에는 최대 응력이 감소하나, 10 mm에서 11.5 mm로 증가 시에는 최대 응력이 증가했으며, 길이가 10 mm 일 때, 가장 낮은 골 응력을 보였다. 전의 실험 결과들 13, 26, 28 은 길이가 길어질수록 골 응력이 감소한다고 보고했으므로, 이번 실험 결과와는 다르다. 임상 연구에서 Schnitman 등 47 은 길이가 10 mm 보다 짧은 경우 즉시 부하 임플란트에서 50%의 실패율을 보였다고 했다. 또 많은 논문들 48-50에서 즉시
- 24 - 부하에서는 길이 10 mm 이상의 임플란트를 식립할 것을 추천하고 있다. 그러나, straight형 직경 4.3 mm 임플란트 모델들에서는 길이가 길어질수록 최대 응력이 증가하였다. Straight 형의 직경 4.3 mm 임플란트에서는 길이를 증가시키는 것이 전혀 최대 응력 감소에 도움을 주지 않았다. 직경에 대한 결과를 보면, straight 형 길이 8.5, 10 mm 임플란트 모델들을 제외하고는, 같은 바디 형태와 길이를 가진 임플란트 모델들에서는 직경이 증가할수록 최대 응력이 감소했다. 이것은 지연 부하시의 실험 결과와 일치하는 모습을 보여주며, 다른 즉시 부하 상황의 유한 요소 분석 실험에서의 결과와도 일치한다. 26, 28 O¨stman 51은 더 넓은 임플란트는 협측과 구개측 치밀골에 더쉽게 삽입되어 골-금속 표면 접촉을 크게 한다고 했다. 그의 다른 연구에서도 narrow/regular 임플란트에 비해 wide 임플란트가 공진 주파수 분석에서 더 높은 초기 임플란트 안정성을 보였다. 또한, 단일 치관 수복물을 지지하는 wide body 임플란트의 즉시 하중에 대한 성공적인 연구 결과들이 발표되었다. 52-54 그러나, straight 형 길이 8.5, 10 mm 임플란트 모델들에서는 직경이 4.3 mm에서 5.3 mm로 증가 시, 최대 응력이 증가했다. 이것은 5mm보다 더 큰 직경의 임플란트는 골에서 더 큰 응력을 보여주므로, 즉시 부하 프로토콜에서 선택해서는 안 된다고 주장한 Georgiopoulas 등 13 의 결과와 일치한다. Degidi 등 55 는 임상 연구 결과 직경이 5.25 mm을 넘는 임플란트는 즉시 부하 시 위험성이 증가한다고 발표하였다. 즉 지연 부하와 달리 즉시 부하에서는 직경이 증가할 때 반드시 최대 응력이 감소하는 것은 아니었다.
- 25 - 바디 형태에서는 4.3 X 8.5 mm의 임플란트 모델을 제외하고, tapered 형 임플란트가 straight 형 임플란트보다 최대 응력 값이 더 낮게 나타남으로써, 지연 부하와 가장 대조적인 모습을 보여주었다. 임플란트 바디 형태는 지연 부하에서도 중요한 요인이지만, 즉시 부하에서 더 특별한 중요성을 가진다. 그 이유는 즉시 부하에서는 임플란트를 식립하자마자 최대의 안전성을 얻어야 하며, 교합력 적용 전에 골이 임플란트 바디의 요철 부위로 자라거나, 표면에 부착할 시간이 없기 때문이다. 21
Huang 등 23 은 tapered 형 임플란트는 square straight 디자인에 비해 피질골에서 응력을 방출시켜 망상골로 더 많이 응력을 이동시켜 피질골과 망상골에서 응력을 감소시킨다고 했다. Tapered 형 임플란트의 나선의 증가된 깊이는 골-임플란트 접촉 면적를 깊게 증가시켜서 이런 생역학적 효과에 기여했을 수도 있다. 피질골 부위에 응력이 집중되어 있는 지연 부하에 비해, 즉시 부하에서는 피질골뿐만 아니라 해면골에도 응력이 광범위하게 분포하며, 골 응력이 더 높으므로, 이러한 tapered 형의 임플란트가 straight 형 임플란트보다 더 낮은 최대 응력 값을 보일 수 있을 것이다. 즉시 부하에서는 tapered 형 임플란트가 straight 형보다 추천된다는 연구 결과들이 있다. 8, 21, 56, 57 O¨ stman 등 58 과 Glauser 등 59 은 부드러운 골질을 가진 부위에서 tapered 형 임플란트의 즉시 부하 시술시의 높은 생존율을 발표했다. Tapered 형의 임플란트의 성공은 골질, 수술기법과 관계 있으며, taper 각과 나선 깊이에 따라 다양한 결과를 가져올 수 있다.
- 26 - 거리에 대한 영향은 서로 일치하지는 않았지만, tapered형 4.3 X 11.5 mm 임플란트는, tapered 형 임플란트 중에서, 최대 변위 거리도 최대 응력과 같이 가장 높은 값을 보였다. 그러나, 모든 모델에서 최대 변위 거리는, 즉시 부하에서 허용되는 미세동요도인 50 μm 이하의 값을 나타냄으로써, 골형성을 방해하지 않는 것으로 보인다. 이렇게 지연 부하에서는 길이, 직경, 바디 형태들의 변화에 따른 최대 응력에 대한 영향이 비교적 규칙적인 양상을 보였으나, 즉시 부하에서는 이들의 영향이 다양하게 나타나는 모습을 보여주었다. 즉 지연 부하에서의 이들의 최대 응력에 대한 영향과 일치하지 않을 수 있다는 것을 보여주었다. 본 실험에서는 유한 요소 분석에 의해 변수들에 따른 최대 응력에 대한 영향의 전반적인 경향만 살펴보았다. 따라서, 앞으로 변수들의 최대 응력에 대한 영향과 변수들간의 영향을 분석하기 위한 통계적 결과 처리가 가능한 실험이 요구된다. 즉시 부하의 성공에는 여러 가지 요인들이 복합적으로 영향을 끼치기 때문에, 최대 응력의 감소가 임플란트 성공률과 반드시 일치하지 않을 수도 있다. 따라서, 근거가 될만한 임상 연구가 같이 동반되어야 할 것이다. 그 밖에 실험 조건에서 본 연구는 교합력으로 110N 크기의, 수직 부하만 재현해서, 모델에 정적 하중을 가했다. Morneburg와 Proshchel 37 등은 단일 임플란트의 평균 최대 교합력은 구치부에서 129N 정도라고 했으며, 그 밖의 연구 61 에서도 임플란트 지지 보철물에서 112.9N 정도라고 했으므로, 이에 근거해 교합력의 크기를 재현했다. 그리고, 사선 방향의 힘이나 측방력이 작용시 응력이 증가할 뿐만 아니라, 응력의 형태도 전단력 같이 골에 위험한 형태로 바뀌어, 골소실이나 골재성장에 손상을 가져오므로, 지연 부하에서뿐만 아니라, 완전한
- 27 - 골유착이 이루어지지 않은 조건을 가진 즉시 부하에서는 더욱이 작용되지 않아야 한다. 38 또한, 기존의 지연 부하 상황에서 이 같은 하중을 가하는 많은 실험을 하여, 이미 위와 같은 결과들을 얻었다. 따라서, 본 실험에서는 수직 방향 이외의 힘들을 재현하지 않았다. 그러나, 정적 하중 모델에 비해 동적 하중 모델에서 임플란트-골 계면에서 더 높은 최대 응력의 결과를 보여준다는 연구 결과 60도 있으며, 실제 구강 내 상황과 더 일치하므로, 즉시 부하의 동적 하중 모델에서의 유한 요소 분석에 대해서도 좀더 연구해 볼 필요가 있을 것이다.
- 28 -
V. 결 론
유한 요소 분석을 이용해, 임플란트의 즉시 부하 상황을 재현해서 임플란트 주위 골의 응력 분포에 대한 임플란트 디자인의 영향을 연구한 결과는 다음과 같다. 1. 지연 부하와 비교해서 즉시 부하에서는 응력이 피질골 뿐만 아니라, 임플란트-골 계면을 따라 임플란트 근단까지 해면임플란트-골에도 광범위하게 분포하며, 최대 등가 응력도 더 높게 나타났다. 2. 지연 부하에서는, tapered 형 직경 4.3 mm 의 임플란트 모델이 10 mm 에서 11.5 mm 로 길이가 증가 시 최대 응력이 다소 증가하는 양상을 보인 것을 제외하고는, 임플란트의 길이가 길어질수록 최대 응력이 감소했다. 또한 임플란트 직경이 커지면 최대 응력이 감소했으며, tapered 형 임플란트가 straight 형 임플란트보다 최대 응력이 더 높았다. 3. 즉시 부하에서, tapered 형의 임플란트는 길이가 8.5 mm 에서 10 mm 로 증가 시에는 최대 응력이 감소하나, 10 mm 에서 11.5 mm 로 증가 시에는 최대 응력이 증가했으며, 직경이 증가할수록 최대 응력이 감소했다. 바디 형태에서는 4.3 X 8.5 mm 의 임플란트 모델을 제외하고, tapered 형 임플란트가 straight 형 임플란트보다 최대 응력이 더 낮게 나타났다. 즉시 부하 시 임플란트-골 계면의 최대 변위 거리는 허용되는 미세동요도인 50 μm 이하의 값을 나타냄으로써, 골형성을 방해하지 않는 것으로 보인다.- 29 -
4. 지연 부하에서는 길이, 직경, 바디 형태들의 변화에 따른 최대 응력에 대한 영향이 비교적 규칙적인 양상을 보였으나, 즉시 부하에서는 이들의 영향이 다양하게 나타나는 모습을 보여주었다. 즉 지연 부하에서의 변수들의 영향과 일치하지 않을 수 있다는 것을 보여주었다.
- 30 -
참고 문헌
1. P.I. Branemark, B.O. Hansson, R. Adell, U. Breine, J. Lindstrom and O. Hallen et al. Osseointegrated implants in the treatment of the edentulous jaw: experience from a 10-year period, Scand J Plast Reconstr Surg Suppl. 1977;11 :1–132.
2. P.I. Branemark, G. Zarb and T. Albrektsson, Tissue integrated prostheses: osseointegration in clinical dentistry, Quintessence, Chicago. 1985:11-77. 3. Chiapasco M. Early and immediate restoration and loading of implants in
completely edentulous patients. Int J Oral Maxillofac implants.2004;19 (Suppl.);6–91.
4. Ganeles J, Wismeijer D. Early and immediately restored and loaded dental implants for single-tooth and partial arch applications. Int J Oral Maxillofac Implants. 2004;19(Suppl):92–102
5. O¨ stman PO, Hellman M, Sennerby L. Direct implant loading in the edentulous maxilla using a bone density-adapted surgical protocol and primary implant stability criteria for inclusion. Clin Implant Dent Relat Res 2005;7 Suppl 1:S60–S69.
6. Romanos GE, Nentwig GH. Immediate versus delayed functional loading of implants in the posterior mandible: a 2-year prospective clinical study of 12 consecutive cases. Int J Periodontics Restorative Dent 2006;26:459–469 7. Avila G, Galindo P, Rios H, Wang HL. Immediate implant loading: current
- 31 -
8. Wang HL, Ormianer Z, Palti A, et al. Consensus Conference on Immediate Loading: The Single Tooth and Partial Edentulous Areas. Implant Dent. 2006;15:324-333.
9. Linkow LI. Endosseous blade-vent implants: a two-year report. J Prosthet Dent.1970;23:441-448.10.
10. Linkow LI, Donath K, Lemons JE. Retrieval analyses of a blade implant after 231 months of clinical function. Implant Dent.1992;1:37-43.
11. Linkow LI, Glassman PE, Asnis ST. Macroscopic and microscopic studies of endosteal bladevent implants (6 month dog study). Oral Implantol. 1973;3:281-309.
12. Brunski JB, Moccia AF, Jr, Pollack SR, et al. The influence of functional use of endosseous dental implants on the tissue-implant interface. I. Histological aspects J Dent Res. 1979;58:1953-1969.
13. Georgiopoulos B, Kalioras K, Provatidis C, Manda M, Koidis P. The effects of implant length and diameter prior to and after osseointegration: a 2-D finite element analysis. J Oral Implantol. 2007;33(5):243-56.
14. Horiuchi K, Uchida H, Yamamoto K, Sugimura M. Immediate loading of Brånemark system implants following placement in edentulous patients: a clinical report. Int J Oral Maxillofac Implants. 2000 Nov-Dec;15(6):824-30. 15. Tealdo T, Bevilacqua M, Pera F, Menini M, Ravera G, Drago C, Pera P.
Immediate function with fixed implant-supported maxillary dentures: a 12-month pilot study. J Prosthet Dent. 2008 May;99(5):351-60.
- 32 -
16. Nikellis I, Levi A, Nicolopoulos C. Immediate loading of 190 endosseous dental implants: a prospective observational study of 40 patient treatments with up to 2-year data. Int J Oral Maxillofac Implants. 2004 Jan-Feb;19(1):116-2.
17. Chiapasco M, Gatti C. Implant-retained mandibular overdentures with immediate loading: a 3- to 8-year prospective study on 328 implants. Clin Implant Dent Relat Res. 2003;5(1):29-38.
18. Romanos GE, Toh CG, Siar CH, Swaminathan D. Histologic and histomorphometric evaluation of peri-implant bone subjected to immediate loading: an experimental study with Macaca fascicularis. Int J Oral Maxillofac Implants. 2002 Jan-Feb;17(1):44-51.
19. Romanos GE, Toh CG, Siar CH, Wicht H, Yacoob H, Nentwig GH. Bone-implant interface around titanium Bone-implants under different loading conditions: a histomorphometrical analysis in the Macaca fascicularis monkey. J Periodontol. 2003 Oct;74(10):1483-90.
20. Gapski R, Wang HL, Mascarenhas P, et al. Critical review of immediate implant loading. Clinical Oral Implants Research. 2003;14:515-527.
21. Misch CE, Wang HL, Misch CM, Sharawy M, Lemons J, Judy KW. Rationale for the application of immediate load in implant dentistry: part II. Implant Dent. 2004 Dec;13(4):310-21.
22. Kong L, Sun Y, Hu K, Li D, Hou R, Yang J, Liu B. Bivariate evaluation of cylinder implant diameter and length: a three-dimensional finite element analysis. J Prosthodont. 2008 Jun;17(4):286-93. Epub 2008 Jan 15
- 33 -
23. Huang HL, Chang CH, Hsu JT, Fallgatter AM, Ko CC. Comparison of implant body designs and threaded designs of dental implants: a 3-dimensional finite element analysis. Int J Oral Maxillofac Implants. 2007 Jul-Aug;22(4):551-62.
24. Petrie CS, Williams JL. Comparative evaluation of implant designs: influence of diameter, length, and taper on strains in the alveolar crest. A three-dimensional finite-element analysis. Clin Oral Implants Res. 2005 Aug;16(4):486-94.
25. Himmlová L, Dostálová T, Kácovský A, Konvicková S. Influence of implant length and diameter on stress distribution: a finite element analysis.J Prosthet Dent. 2004 Jan;91(1):20-5.
26. Ding X, Liao SH, Zhu XH, Zhang XH, Zhang L.Effect of Diameter and Length on Stress Distribution of the Alveolar Crest around Immediate Loading Implants.Clin Implant Dent Relat Res. 2008 Sep 9.
27. Huang HL, Fuh LJ, Hsu JT, Tu MG, Shen YW, Wu CL.Effects of implant surface roughness and stiffness of grafted bone on an immediately loaded maxillary implant: a 3D numerical analysis.J Oral Rehabil. 2008 Apr;35(4):283-90.
28. Huang HL, Hsu JT, Fuh LJ, Tu MG, Ko CC, Shen YW. Bone stress and interfacial sliding analysis of implant designs on an immediately loaded maxillary implant: a non-linear finite element study.J Dent. 2008 Jun;36(6):409-17. Epub 2008 Apr 1.
- 34 -
29. Geng JP, Tan KB, Liu GR. Application of finite element analysis in implant dentistry: a review of the literature. J Prosthet Dent. 2001 Jun;85(6):585-98.
30. Winter W, Heckmann SM, Weber HP. A time-dependent healing function for immediate loaded implant. J Biomech. 2004 Dec;37(12):1861-7.
31. Rieger MR, Adams WK, Kinzel GL, Brose MO. Finite element analysis of bone-adapted and bone-bonded endosseous implants. J Prosthet Dent. 1989 Oct;62(4):436-4.
32. Pérez del Palomar A, Arruga A, Cegoñino J, Doblaré M. A finite element comparison between the mechanical behaviour of rigid and resilient oral implants with respect to immediate loading. Comput Methods Biomech Biomed Engin. 2005 Feb;8(1):45-57.
33. Mellal A, Wiskott HW, Botsis J, Scherrer SS, Belser UC. Stimulating effect of implant loading on surrounding bone. Comparison of three numerical models and validation by in vivo data. Clin Oral Implants Res. 2004 Apr;15(2):239-48.
34. Lekholm U, Zarb GA.Tissue-integrated Prostheses: Osseointegration in clinical dentistry.1985;199-209.
35. Rancourt D, Shirazi-Adl A, Drouin G, Paiement G. Friction properties of the interface between porous-surfaced metals and tibial cancellous bone. J Biomed Mater Res. 1990 Nov;24(11):1503-19.
- 35 -
36. Rubin PJ, Rakotomanana RL, Leyvraz PF, Zysset PK, Curnier A, Heegaard JH. Frictional interface micromotions and anisotropic stress distribution in a femoral total hip component. J Biomech. 1993 Jun;26(6):725-39.
37. Morneburg TR, Proschel PA. Measurement of masticatory forces and implant loads: a methodologic clinical study. Int J Prosthodont. 2002;15:20-27
38. Misch CE. Dental Evaluation: Factors of Stress.& Occlusal Considertations for Implant-Supported Prostheses. Contemporary Implant Dentistry, 2nd ed. St. Louis: Mosby;1999:119.&609
39. Van Oosterwyck H, Duyck J, Vander Sloten J, Van der Perre G, De Cooman M, Lievens S, Puers R, Naert I. The influence of bone mechanical properties and implant fixation upon bone loading around oral implants. Clin Oral Implants Res. 1998 Dec;9(6):407-18.
40. Cochran DL. The evidence for immediate loading of implants. J Evid Based Dent Pract. 2006 Jun;6(2):155-63.
41. Berglundh T, Abrahamsson I, Lang NP, Lindhe J. De novo alveolar bone formation adjacent to endosseous implants. Clin Oral Implants Res. 2003 Jun;14(3):251-62.
42. Viceconti M, Muccini R, Bernakiewicz M, Baleani M, Cristofolini L. Large-sliding contact elements accurately predict levels of bone-implant micromotion relevant to osseointegration. J Biomech. 2000 Dec;33(12):1611-8.
- 36 -
43. Mailath G, Stoiber B, Watzek G, Matejka M. Bone resorption at the entry of osseointegrated implants—a biomechanical phenomenon. Finite element study [in German]. Z Stomatol 1989;86:207-16.
44. Siegele D, Soltesz U. Numerical investigations of the influence of implant shape on stress distribution in the jaw bone. Int J Oral Maxillofac Implants 1989;4:333-40.
45. Patra AK, DePaolo JM, D’Souza KS, DeTolla D, Meenaghan MA. Guidelines for analysis and redesign of dental implants. Implant Dent 1998;7:355-68. 46. Attard NJ, Zarb GA. Immediate and early implant loading protocols: a
literature review of clinical studies. J Prosthet Dent 2005;94;242–258. 47. Schnitman PA, Wohrle PS, Rubenstein JE. Immediate fixed interim
prostheses supported by two-stage threaded implants: methodology and results. J Oral Implantol. 1990;16:96–105.
48. D.P. Tarnow, S. Emtiaz and A. Classi, Immediate loading of threaded implants at stage 1 surgery in edentulous arches: ten consecutive case reports with 1- to 5-year data, Int J Oral Maxillofac Implants. 1997;12:319–324.
49. I. Ericsson, H. Nilson, T. Lindh, K. Nilner and K. Randow, Immediate functional loading of Branemark single-tooth implants. An 18 months' clinical pilot follow-up study, Clin Oral Implants Res. 2000 Feb; 11(1):26– 33.
- 37 -
outcome in immediate loading? Int. J. Oral Maxillofac. Surg. 2007;36:1172-1176.
51. Ostman PO. Immediate/early loading of dental implants. Clinical documentation and presentation of a treatment concept. Periodontol 2000. 2008;47:90-112.
52. Calandriello R, Tomatis M, Vallone R, Rangert B, Gottlow J. Immediate occlusal loading of single lower molars using Brånemark System Wide-Platform TiUnite implants: an interim report of a prospective open-ended clinical multicenter study. Clin Implant Dent Relat Res. 2003;5 Suppl 1:74-80.
53. Cornelini R, Cangini F, Covani U, Barone A, Buser D. Immediate restoration of single-tooth implants in mandibular molar sites: a 12-month preliminary report. Int J Oral Maxillofac Implants. 2004 Nov-Dec;19(6):855-60.
54. Schincaglia GP, Marzola R, Giovanni GF, Chiara CS, Scotti R. Replacement of mandibular molars with single-unit restorations supported by wide-body implants: immediate versus delayed loading. A randomized controlled study. Int J Oral Maxillofac Implants. 2008 May-Jun;23(3):474-80.
55. Degidi M, Piatelli A. Immediate functional and non-functional loading of dental implants: a 2 to 60 month follow-upstudy of 646 titanium implants. J Periodontol. 2003 Feb;74(2):225-41.
- 38 -
56. Testori T, Smukler-Moncler S, Francetti L, et al. The immediate-loading of Osseotite implants. A clinical and histological assessment 4 months after being brought into function. Parodontie-Dentisterie Restauratrice. 2001;21:451–459.
57. Piatelli A, Corigliano M, Scarano A, et al. Bone reactions to early occlusal loading of two-stage titanium plasmasprayed implants: a pilot study in monkeys. Int J Perio Rest Dent. 1997;17:162–169.
58. Ostman PO, Hellman M, Albrektsson T, Sennerby L. Direct loading of Nobel Direct and Nobel Perfect one-piece implants: a 1-year prospective clinical and radiographic study. Clin Oral Implants Res. 2007 Aug;18(4):409-18.
59. Glauser R, Zembic A, Ruhstaller P, Windisch S. Five-year results of implants with an oxidized surface placed predominantly in soft quality bone and subjected to immediate occlusal loading. J Prosthet Dent. 2007 Jun;97(6 Suppl):S59-68.
60. Kayabasi O, Yüzbasioğlu E, Erzincanli F, Static, dynamic and fatigue behaviors of dental implant using finite element method. Advances in Engineering software 37(2006) 649-658.
61. Carr AB, Laney WR. Maximum occlusal force levels in patients with osseointegrated oral implant prostheses and patients with complete dentures. Int J OralMaxillofac Implants. 1987; 2: 101-108.
- 39 -
Abstract
The effect of implant designs on stress distribution
of the bone around immediate loading implants
: A 3-dimensional finite element analysis
Jung Yoon Bae
Department of Dentistry
The Graduate School, Yonsei University
(Directed by Professor Chong Hyun Han)
Until recently, the healing period from dental implant placement to the prosthesis delivery has become shorter and even immediate loading procedure become popular. Implant primary stability is the most important clinical factor influencing success of immediate loading. The surface area of implant support may be increased by modifications in implant designs, so the stress in the bone be decreased. But, the effect of implant designs in immediately loaded implants has recently been investigated and will affect different compared to in delayed loaded implants. The purpose of this study was to investigate the effect of implant designs on stress distribution of the bone around immediate loading implants by a 3-dimensional finite element analysis and to help to select proper implant for immediate loading treatment.
- 40 -
A 3-dimensional model of a single implant supported crown substituting a lower first premolar was simulated. The von-Mises stresses of the bone around different implant length (8, 10, 11.5 mm), diameter (4.3, 5.3 mm) and body design (tapered, straight) with delayed loaded and immediately loaded condition were analyzed.
The results were as followings;
1. Compared to the delayed loaded implants, in immediately loaded implants, the stresses were widely distributed in trabecular bone to the implant apex along implant-bone interfaces as well as in cortical bone surrounding the implant neck and the maximum von-Mises stresses were higher.
2. For the delayed loaded implants, except that increasing implant length from 10 mm to 11.5 mm resulted in the maximum stress increasing, in diameter 4.3 mm tapered implants, increasing implant length resulted in the maximum stress reduction. And increasing implant diameter decreased the maximum stress, tapered implants showed higher maximum stresses than straight implants.
3. For the immediately loaded implants, increasing implant length from 8.5 mm to 10 mm resulted in the maximum stress reduction, but increasing implant length from 10 mm to 11.5 mm resulted in the maximum stress increasing and increasing implant diameter resulted in the maximum stress reduction in tapered implants. Except for 4.3 X 8.5 mm implant, tapered implants showed
- 41 -
lower maximum stresses than straight implants. The maximum sliding distance of model of contact implant-bone interfaces was less than accepted micromotion value (50 μm), so did not disturb osseointegration.
4. For the delayed loaded implants, the effects of the implant length, diameter, and body design on maximum stresses showed relatively regular appearance, but
the effect of implant designs in immediately loaded implants showed various appearances, in other words, did not accord in delayed loaded implant
--- Key word : immediate loading, finite element analysis, dental implant, length,