◈ 원 저 ◈
비만으로 인한 전립선암 발생의 영향연구
: 복부비만도 측정과 그 외 생활 요인
김명성
국립암센터 방사선과
Association of visceral fat obesity and other lifestyle factors with
prostate cancer
Myeong-Seong Kim
Department of Radiology, National Cancer Center
Abstract
최근 우리나라의 암 발생률은 꾸준히 증가추세에 있고 그 중에서도 전립선암은 갑상선암을 제외했을 때 남성에서 가장 높은 증가 추세를 보이고 있는 암이다. 전립선암은 그 동안 선진국에서 주로 발병하는 것으로 알려진 암 종이 지만 서구화된 식습관과 생활 행태 변화로 인하여 국내에서도 발생률이 증가하는 것으로 추정하고 있다. 따라서 국 내 환경에 맞는 내장 지방 분포와 같은 정확한 비만도 측정을 통해 우리나라에서 증가율 1위를 보이고 있는 전립선 암 발생의 원인 관계를 찾고자 한다. 본 연구는 환자와 정상군 비교를 하는 환자-대조군 연구이고 본 연구를 위하여 임상시험 윤리위원회 (IRB) 승인 을 받았다 (NCC2014-0124). 환자군은 2014년 8월 1일부터 2015년 1월 6일 까지 국립암센터를 방문하여 전립선암 을 진단받고 수술과 항암치료 그리고 방사선 치료를 시작하지 않은 초진을 대상으로 하였고, 정상군은 2009년 11월 부터 2014년 9월 30일까지 공단검진을 목적으로 국립암센터를 방문한 정상인을 대상으로 하였다. 전립선암 연구는 환자 총 52명에 평균 66세 (51 – 82세)이고 정상군은 총 50명에 평균 64세 (59 – 75세) 이다. 모든 연구 대상자들 의 생활 요인 평가를 위하여 암 가족력, 흡연, 음주 상태, 운동, 등을 추가적으로 설문 조사하였다. MRI 영상의 배 꼽 주위에서의 내장 지방과 피하지방을 전용 분석 컴퓨터를 활용하여 측정 하였다. 복부비만율은 환자군과 정상군에서뿐만 아니라 (p = 0.03), 전립선암 악성도와 (Gleasonscore; p = 0.001)도 통 계적 차이를 나타냈다. 하지만 BMI 결과와는 전립선암 발생과 악성도에서 무관함을 보인 것에 반해 허리둘레는 전 립선암의 발생에 영향을 미치는 결과를 나타났다. 한편 전립선암의 또 다른 악성도 지표인 PSA는 비만 측정치와의 상관성이 Gleason score와 보다 대체적으로 낮게 나타났다. 학력, 운동량, 흡연, 음주 상태와 같은 생활 특성에 따 른 전립선암 발생의 영향 관계는 뚜렷하지 않았다. 결론적으로 본 연구를 통해서 전립선암의 발생 위험도와 악성도 지표로 복부 비만도가 유용함을 나타냈고 간단한 신체 계측 지표 활용으로는 BMI보다 허리둘레 측정치가 더 암 발생의 연관성이 높음을 보였다.Ⅰ. INTRODUCTION
Prostate cancer is a very common form of cancer in men and the second leading cause of cancer deaths in men in the Western populations1).
In contrast, prostate can cerranks as the fifth
most common can cerin men but them
ostprevalent can cerin annual rate of change (11.4%) with in creasing steadily in men in South Korea(Korean National Cancer Information Center. 2014). This rising trend may be explained by not only age, family history of prostate cancer also lifestyle factors such as westernization (increased intake of animal derived food products and life
style changes such as lack of physical
activity)2-4). Therefore prostate cancers in
westernized countries have incidence rates that are 10~15 times those of non-westernized countries. Inaddition, immigrant’s studies have indicated that Asian American men living in the United States have much higher incidence rates (50 per 100,000 men-years) than do their native counties (10 to 20 per 100,000 men-years)(Hsing and Devesa. 2001; Hsing and Chokkalingam. 2006).
Westernization cause of increased prostate cancer is unclear. However cancer statics and many cancer studies have shown that the increased incidence rate of prostate cancer associated with increased prevalence of obesity (Ahnmedin et al 2010; Ministry of Health and
Welfare. 2010; Korean National Cancer
Information Center. 2014).
Many prostate cancers studies have shown that obesity is associated with an increase in risk of prostate cancer in inconsistent findings (Qu et al 2013). However recent studies indicate that obesity is increased risk on prostate cancer also increase in risks of advanced prostate cancer (Calle and Kaaks 2004). A reason for such dispute outcomes could be the BMI and classical anthropometric measures such as simple weighting
used their study, and failure to characteristic the contribution of subcutaneous and visceral fat (Qu et al 2013). Especially in men with greater muscle, classical anthropometric measures are not good method for obesity study because of
imperfect reflect multicompartment body
composition (van der Kooy et al 1993; Weits et al 1998). Recent studies have been shown that visceral obesity increases the risk of prostate cancer (von Hafe et al 2004; Qu et al 2013). Therefore, allowing obtained cross sectional body image and can be quantifies measurement of visceral fat needed medical modality such as CT or MRI.
We hypothesized that usual fat diet intake effect on visceral fat and accumulation as measured by MRI could be associated with the incidence of prostate cancer. In addition, we conducted study association between risk factor for obesity such as physical activity, alcohol consumption and stress influence the obesity
II. Materials and Methods
2.1. Study design and Subjects
This study is a case control and case only study with prostate cancer patients who visited at the Korean National Cancer Center hospital from August 1st, 2014 to April 24st, 2015. Control group is normal healthy participants without cancer who visited Korean National Cancer Center hospital for the health examination service by national health insurance from September 1st, 2008 to September 30th, 2014. The target participants were set as newly diagnosed with prostate cancer and undiagnosed cancer person as control. To find more association between abdominal fat ratio and prostate cancer, in addition to collected more abdominal fat data. That is this study was collected data from all of
variables (abdominal fat ratio, and other factors) with prospective (n=55) and prospective data with retrospective related abdominal fat ratio (n=150). The prostate cancer patients were 150 male aged ranges from 48 to 85 years with a mean age of 66.2 ± 6.8 years old and that of the control participants were 150 male aged ranges from 52 to 75 years with a mean age of 61.4 ± 4.6 years old. Prostate cancer is diagnosed in very few men aged younger than 55 years and increase in
incidence rate with aging. Thus normal
participants are included after age 59 years in this study and there was no difference in age between two groups indicating that prostate cancer patients and normal participants were closely matched.
All cancer patients were only for a newly diagnosed cancer without any related to cancer treatment as take any chemotherapy, radiation therapy and surgery before the start of the study. All normal participants were not take any medications and excluded if they had a personal history of cancer.
2.2. Participants information
All patient’s profile information (height, weight, PSA, Gleason score) obtained from institutional electronic medical record (EMR). Each subject’s weight and height were gathered from the nurse’s information sheet that was recorded at each admission interview to calculate for the BMI. BMI (kg –2) was calculated as bodyweight in kilograms divided by height in meters squared. In addition to the patient’s prostate-specific antigen level (PSA) level obtained from blood sample report in EMR.
Other disease besides prostate cancer in
patients, 30 patients have nothing with
diagnosed, came down with 2 for tuber culosis, 13 for hypertensions, 6 for diabetes, and 1 for patient myocardial infarction.
PSA and Gleason score as histological factor contributed significantly to the prediction of pathological stage. The most common grading system on prostate cancer is the Gleason grading system based upon its microscopic appearance. It is used to help predicts prognosis and guide therapy together with Prostate-specific antigen level (PSA). This score range from 2 to 10 and higher scores indicate more aggressive and have a worse prognosis5). The evaluation of this grade is
determined by pathologists that tumor specimen from our institution the preoperative biopsy. And this grade is used for malignancy factor on prostate cancer according to obesity in this study also obtained from pathology report section in EMR.
2.3. Abdominal fat ratio
On prostate cancer patients, measurements of abdominal fat were using MRI due to base on MRI for initial work-up prostate cancer in this study hospital. The study was conducted on a 3.0 Tesla Achieva and Achieva TX MR system (Philips Medical Systems, Best, The Netherlands), using a SENSE-XL-Torso imaging coil placed around the lower abdomen.
Anthropometric measures of abdominal adiposity, including A, P and AP, were measured from the T2-weighted axial localisation images from MRI for 200 patients (Figure 1).21 A and P were measured as the fat thickness between the skin and the anterior abdominal musculature or posterior musculature. All measurements were performed at the midline, which was identified at the umbilicus level and at one cut immediately to the left and right of the midline in a blinded manner by a single person. These measurements were then averaged for the final measurement. The SAT value was calculated with the formula SAT=A+P. The degree of visceral obesity was defined as the percentage of VAT (VAT%), which
was calculated according to the formula VAT%=[(AP-SAT)/AP]x100 4).
2.4. Analysis
All means and distributions of demographic and characteristics were examined using the t-tests and chi-square tests. Multiple regression analysis was conducted to determine which of the many variables on prostate cancer after using the normal transformed variables. Among the relevant variables, odds ratios and 95% confidence intervals (CIs) were analyzed by entered logistic regression. Statistical analysis was performed using SPSS statistics v. 20 (SPSS Inc., Chicago, IL, USA), and p values < 0.05 were considered statistically significant.
III. Results
3.1. Comparison of characteristic and
distribution in case control study
Table 1show the detail of demographic
characteristics in this study.
General characteristics of sum daily intake of nutrients estimated by FFQ are presented in Table III-2. There were no statistically significant differences (t-test) between cases and controls in most of sum daily intake of nutrients that is total energy (p = 0.11), vegetable protein (p = 0.96), vegetable lipid (p = 0.38), animal protein (p = 0.10), glucose (p = 0.55), and dietary fiber (p = 0.31). However compared with controls, cases had a higher abdominal fat ratio (51.6% ± 7.9 for case, 49.4% ± 8.1 for control; p = 0.04) and animal lipid intakes (28.29 ± 24.1 for case, 18.41 ± 10.5; p = 0.01) with statistical significant
difference. However adjusted for total
consumption, animal lipid was changed into moderate differenced (p = 0.07) and dietary fiber
was changed into increased statistically significant difference in case and control (p = 0.02).
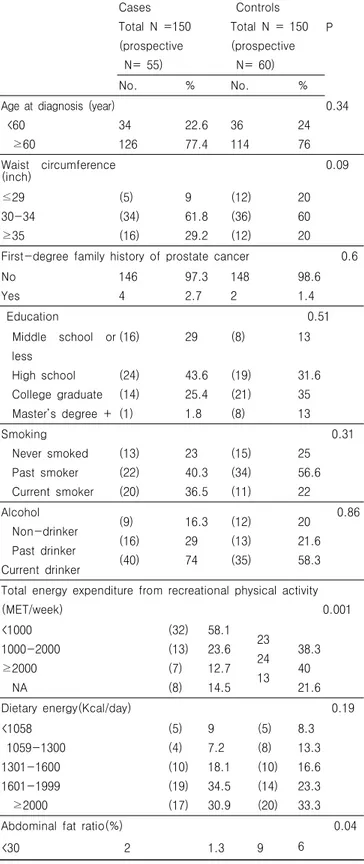
Table 1. Demographic characteristics of study participants
P value in case-control : Chi square tests
Cases Total N =150 (prospective N= 55) Controls Total N = 150 (prospective N= 60) P No. % No. %
Age at diagnosis (year) <60 ≥60 34 126 22.6 77.4 36 114 24 76 0.34 Waist circumference (inch) 0.09 ≤29 30-34 ≥35 (5) (34) (16) 9 61.8 29.2 (12) (36) (12) 20 60 20
First-degree family history of prostate cancer 0.6 No Yes 146 4 97.3 2.7 148 2 98.6 1.4 Education 0.51 Middle school or less High school College graduate Master’s degree + (16) (24) (14) (1) 29 43.6 25.4 1.8 (8) (19) (21) (8) 13 31.6 35 13 Smoking Never smoked Past smoker Current smoker (13) (22) (20) 23 40.3 36.5 (15) (34) (11) 25 56.6 22 0.31 Alcohol Non-drinker Past drinker Current drinker (9) (16) (40) 16.3 29 74 (12) (13) (35) 20 21.6 58.3 0.86
Total energy expenditure from recreational physical activity (MET/week) 0.001 <1000 1000-2000 ≥2000 NA (32) (13) (7) (8) 58.1 23.6 12.7 14.5 23 24 13 38.3 40 21.6 Dietary energy(Kcal/day) 0.19 <1058 1059-1300 1301-1600 1601-1999 ≥2000 (5) (4) (10) (19) (17) 9 7.2 18.1 34.5 30.9 (5) (8) (10) (14) (20) 8.3 13.3 16.6 23.3 33.3 Abdominal fat ratio(%) 0.04
There were no correlation between total calories intake and all of anthropometric measurements (waist circumference, BMI, abdominal fat ratio).
Abdominal total fat was highest positive
correlation with all of anthropometric
measurements p < 0.001), exclude abdominal fat ratio (r = 0.43). As shown Table 2, correlation with BMI, waist circumference correlate, visceral fat, and abdominal total fat were high positive relation with statistical significant (p < 0.001). Also similar results of correlation analysis show in prostate cancer patients. For correlation in detail is shown in Table 2 and 3.
Table 2. Pearson correlation coefficients with anthropometric measurements and daily total calories in all of subjects
TC (log kcal) WC FR VF TF TC(log kcal) . 0.21 0.09 0.15 0.18 WC *0.21 . **0.26 ***0.62 ***0.71 FR 0.09 **0.26 . ***0.73 ***0.43 VF 0.15 ***0.62 ***0.73 . ***0.91 TF 0.18 ***0.71 ***0.43 ***0.91 .
TC: Total calories; WC: Waist circumference; FR: Abdominal fat ratio; VF: Visceral fat; TF: Total fat
*: p < 0.05 ***: p < 0.001
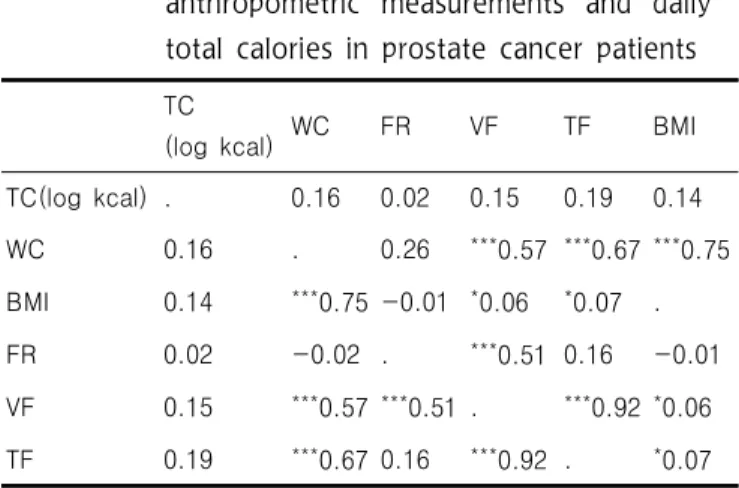
Table 3. Pearson correlation coefficients with anthropometric measurements and daily total calories in prostate cancer patients
TC
(log kcal) WC FR VF TF BMI
TC(log kcal) . 0.16 0.02 0.15 0.19 0.14 WC 0.16 . 0.26 ***0.57 ***0.67 ***0.75 BMI 0.14 ***0.75 -0.01 *0.06 *0.07 . FR 0.02 -0.02 . ***0.51 0.16 -0.01 VF 0.15 ***0.57 ***0.51 . ***0.92 *0.06 TF 0.19 ***0.67 0.16 ***0.92 . *0.07
TC: Total calories; WC: Waist circumference; FR: Abdominal fat ratio; VF: Visceral fat; TF: Total fat
*: p < 0.05 ***: p < 0.001
3.2. Association with predict clinical stage
in prostate cancer patients
Subjects were categorized as divided into two groups by histological grade score (< 7(3+4), ≥ 7(4+3)), to know difference in intake of nutrients on prostate cancer risk depending on Gleason score. Abdominal fat ratio was statistical significant difference in low and high prostate cancer malignant (p = 0.05).
The results of linear regression model were presented in Table 4 and 5. Also there were no association between BMI or waist circumference and PSA or Gleason pathological score (Figure 2). Only abdominal fat was association with prostate cancer Gleason score(β = 0.19, p = 0.09).
A regression model show moderate relation between PSA level and aging (β=0.25, p = 0.01), but more weak relations between aging and Gleason score (β=0.05, p = 0.04) in cancer patients. 30-49 ≥50 79 69 52.6 46 75 66 50 44 Gleason score at diagnosis
2-6 7(3+4) 7(4+3) or 8-10 17 56 77 11.3 37.3 51.3 -PSA level at diagnosis, ng/ml
<4 4-9.9 10-19.9 ≥20 35 59 24 32 23.3 39.3 16 21.3
Table 4. The relationship between Gleason patho- logical score and anthropometric measure- ments (abdominal fat ratio, waist circum- ference, and BMI) or age in prostate cancer 95% CI β Low Upper p Fat ratio (%) 0.19 -0.753 5.606 0.09 Wais circumference 0.08 -0.065 0.122 0.54 BMI -0.03 -0.113 0.081 0.09 Age 0.05 -0.026 0.045 0.04
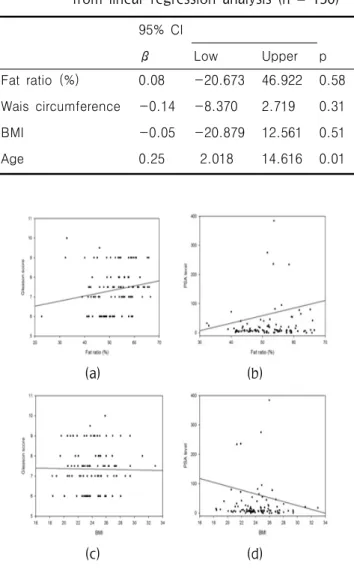
Table 5. The relation between PSA level and abdominal fat ratio, waist circumference, and BMI in prostate cancer patients result from linear regression analysis (n = 150)
95% CI β Low Upper p Fat ratio (%) 0.08 -20.673 46.922 0.58 Wais circumference -0.14 -8.370 2.719 0.31 BMI -0.05 -20.879 12.561 0.51 Age 0.25 2.018 14.616 0.01 (a) (b) (c) (d) (e) (f)
Figure 1. A simple scatter – regression graph on Gleason score of prostate cancer in prostate cancer patients (n = 150)
(a) and (b) correlation between abdominal fat ratio and prostate clinical stage. A positive relation show between Gleason pathological score and abdominal fat ratio (β = 0.19, p = 0.09), but weak positive depict relation between abdominal fat ratio and PSA level (β = 0.08, p = 0.58).
(c) and (d) correlation between BMI and prostate clinical stage. No association show between Gleason pathological score and BMI (β = -0.03, p= 0.09). (e) and correlation between waist circumference and prostate clinical stage. No association show between Gleason pathological score and waist circumference (β =-0.18, p=0.09).
3.3 Personality factors on prostate cancer
As shown in Table 6, lower education level and physical activity increase prostate cancer risk, but no meet with statistical significant (β = -0.17, p = 0.10; β = -0.10, p = 0.35). Waist circumference, smoking and drinking status also shows no association with prostate cancer risk.
To know risk factor on Gleason score of prostate cancer performed analysis multiple regression classified as predicting pathological stage (Gleason pathology score and PSA level) in prostate cancer patients. Life personality factor such as education level, physical activity, and stress level variables show difference statistical value with Gleason pathology score and PSA level. As shown Table 7 and 8, life style factors no association with Gleason score of prostate cancer. Physical activity was negative association with
prostate cancer risk (1030.3 ± 655.2 for case, 1,374 ± 832.8 for control; p= 0.02)(β = - 0.1, p = 0.35) in case control study, but showing positive association with Gleason score in prostate cancer patients (β = 0.27, p = 0.08 for Gleason score; β = 0.31, p = 0.04 for PSA level). Also education level and stress perception level show that opposite standard coefficient (β) value on each predicted pathology stage (Gleason pathology score and PSA level).
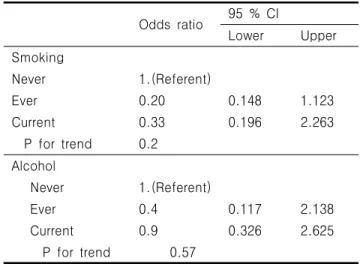
There is no statistical association of Smoking and alcohol consumption to incidence of prostate cancer by multiple regression analysis (p = 0.64 for smoking, p = 0.85 for alcohol consumption) also show similar result by binary regression model (Table 9), in case and control study.
Table 7. The effects of education level, physical activity, and stress on Gleason pathology score in prostate cancer patients (n = 55). Result from multiple regressions.
95% (CI) β Lower Upper p Education level 0.11 -0.259 0.540 0.481 Physical activity (MET score) 0.27 0.000 0.001 0.082 Stress perception -0.257 -0.744 0.062 0.095
Table 8. The effects of education level, physical activity, and stress on PSA level in prostate cancer patients (n = 55)
Result from multiple regressions.
95% (CI) β Lower Upper p Education level -0.18 -38.341 10.878 0.26 Physical activity (MET score) 0.31 -0.000 0.041 0.04 Stress perception 0.11 -15.25 34.427 0.44
Table 9. Odds ratios and 95% CI on prostate cancer risk in relation to smoking and alcohol consumption in all of subjects (n = 55)
Odds ratio 95 % CI Lower Upper Smoking Never Ever Current P for trend 1.(Referent) 0.20 0.33 0.2 0.148 0.196 1.123 2.263 Alcohol Never Ever Current P for trend 1.(Referent) 0.4 0.9 0.57 0.117 0.326 2.138 2.625
V. Discussions
These data presented that the population based, case-control study visited in the Korean national cancer center. Results from this support the hypothesis that abdominal fat ratio and specific nutrient intakes differentially affects the
development of prostate cancer. Although
moderate difference from control groups, the present findings of a prostate cancer patients are higher total calories with animal fat intakes, but lower dietary fat. Thus prostate cancer risks with increasing abdominal fat ratio are consistent in direction with previous studies6). This study
results suggest that prostate cancer patient shave more visceral fat compared withage –matched normal participant softhes ameage. There is
mechanism can explain thevisceral fat
accumulation effect on prostate can cerrisk. Adiposet issue is adepot of specific matters, containing a diponectin, resistin, leptin, and adipsin, correlated directly with C-reactive protein, tumor necrosis factor- and interleukin-6. Adiponectin, resistin, leptin, and adipsin levels are found to be lower in obese than in lean body subjects, therefore negatively correlated with
insulin resistance, and elevated in human obesity
7-9). Thus these higher level of hormones lead to
the growth of prostate can cerrisk and poorly clinical stage.
There is good evidence that Western diet and lifestyle play a significant role in the aetiology of prostate cancer comes from investigations in which incidence rate have been determined for migrants from Japan (low risk) to U.S (high risk). According to Shimizu’s study, prostate cancer is low incidence rate living on Japan (8.4 per 100,000), but when they migrate to the U.S, their incidence of prostate cancer (32.2 per 100,000) close to the average U.S risk as detailed in Table III-17. More tender age also at U.S migration on prostate cancer incidence was higher than for Japanese men in Japan10-11).
Table III-17. Comparison of age-adjusted annual incidence rates in Los Angeles County and homelands. Adapted from Shimizu et al., 1991. Incidence rates per 100,000 population in LA, U.S (1972-85) for migrants to LA; and rates in Miyagi, Japan (1973-81) for Japanese.
Prostate cancer
Area LA Homeland
Incidence rates 32.2 8.4
In addition, good evidence that along with Western dietary patterns, variation in incidence of prostate cancer in Korea. According to KNHANES between 1975 and 2001, Koran diet intake was from traditional gradual changed substantially western diet, despite the intake of total calories declined by 17.3%, with a great increase intake of animal products (from14.3 to 91.7 g) during this time (National Health and Nutrition Survey, 1975 and 2001) (Table III-18).
Table III-18. Changes in daily dietary intake of South Korea from 1975 to 2001. Adapted from Park et al., 2006
1975 year: National Health and Nutrition Survey and Kim, S. W. et al., 2001
1975 2001 % Change
Energy (kcal/day) 2,390 1,976 -17.3
Meat, poultry 14.3 91.7 541.3
% calories from fat 8.6 19.5 126.7
% of fat intake from
meat and meat products 6.0 28.4 373.4
Previous studies investigating risk of prostate cancer and dietary fats have been inconsistent. Case control studies have consistently reported on the positive relation between intake of animal fat and prostate cancer. In contrast, cohort studies no significant associations for animal fat12). The usual intake of a Western diet has characteristics of consume a high fat and low dietary fiber food. Shown results from this study also, prostate cancer patients were consumed typical Western diet type. That is prostate cancer patients were more intake of animal fat and lower intake of dietary fiber than those normal participants. As a result, there is showing a statistical significant difference in abdominal fat ratio between prostate cancer patients and normal participants. Prostate cancer patients were more intake of pork belly with high animal fat among animal products than those normal participants. Especially as more intake of pork pan broiling and chicken is more increased risk of prostate cancer. Pork belly, pork pan broiling, and chicken dishes were include high animal fat, which is promotes tumor progression. Prostate cancer risk is positive relation with amount of saturated fat intake also associations between diet associated and ethnic type. Asians is more associated with effect of animal fat intake on prostate cancer risk than
heterocyclicamines are contained higher amounts in fried orover cooked meats. Those amounts are positive association with cooking increase with increasing temperature and frying time 2). Generally preference for well-done red meat was much higher among Asians than White men preference for rare type. That reason is may be interpreted as inconsistent with associations between red meat intake and prostate cancer risk in Whites men.
Some healthy diet food alone was not significantly protective prostate cancer due to a lot of effect of factors on prostate cancer, but prostate cancer patients are lower intake of fruit and vegetables such as tomato, pear, cabbage soup, orange, grapes, and pepper leaves in this study.
Cruciferous vegetables such as cabbage,
broccoli, cauliflower, and mustard greens are known for specific protective effect on prostate cancer14). There are not include broccoli,
cauliflower, and must ardgreens among FFQ food items in this study due to not to find Korean people favorite food items. Kimchi is cruciferous vegetable family and them ostrep resentative of Korean food item. Intake of kimchi was not significant difference between prostate cancer patients and normal participants, but cabbage soup was shown moderate difference prostate cancer patients and normal participants. This result can be interpreted as not shown statistical difference due to most Korean people frequently intake kimchi, but cabbagesoup was shown moderate statistical difference due to selected according to preference.
Tomatoes are popular in Korea. Tomato products contain lycopene as phyto chemicals is a highly lipid-soluble chemical and the most abundant carotenoid, can reduce the risk of prostate cancer
15-16). Are levant study was reported then
oassociation or moderate beneficial between lycopene consumption and decreasing prostate
cancer, particularly in Asian countries13). However
according to relevant review studies, consuming a tomatoes-based product is strong correlation with lower prostate cancer risk16). Age damber and
orange is in cludenoly copene butthey are most
abundant of carotenoids provide inverse
association with respect to prostate cancer prevention16).
Likes breast cancer study, intake of pepper, including pepper leaves and pepper chilli, is statistical significant or mild difference between prostate cancer patients and normal participants. Still inconsistent with flavonoid, flavonol is also a major component of pepper, which may have a protective effect on prostate cancer risk in animal and epidemiologic studies17).
General biological system, function of adipose tissue in humans is to store energy in the form of fat in case of excessed energy Visceral adipocytes are more metabolically active than abdominal subcutaneous adipocyes, as they have high lypolytic activity and release large amounts of free fatty acids; so useful using measurements of adiposity would consider both the amount and the distribution of the adipose3). In this study,
there is a result show positive association between visceral distribution and prostate cancer risk. However visceral fat is no similar compared with BMI (r = 0.01; p = 0.5), but moderate correlate with waist circumference (r = 0.5; p = 0.01) in prostate cancer patients group. These
results suggest that the use of waist
circumference as a surrogate of abdominal
visceral fat than BMI for anthropometric
measurement tools in epidemiology study.
According to prostate cancer relevant studies, relationship between obesity and prostate cancer risk or Gleason score level have been inconsistent due to most of studies have identified obesity as BMI. BMI is limitation to characterization of body composition, which has metabolic development for steroid hormone balance8). In contrast othed raw
back so fusing BMI, abene fittomeasuring cross sectional body imaging such as MRI and CT is the ability to evaluate, independent of other as
pectsofbody composition. Therefore, MRI is
routinely performed in prostate cancer patients for clinical staging at our institution.
In previous studies that assessed the clinical significance of visceral fat as a risk factor on prostate cancer. The relative risk estimate for waist circumference was 1.03, showing relatively low risk4). However age matched case-control
study that measured abdominal fat distribution via CT showed that prostate can cerpatient shada significantly higher amount of visceral fatanda higher abdominal fat ratio, with an dodds ratio of4.6 (95%CI:2.6to8.2) for visceral fat and 6.0 (95%CI:2.3to11.0) for fat ratio6). In accordance
with previous study, here is positive association between waist circumference or abdominal fat ratio and prostate can cerriskin this study. That is, the odds ratio for higher waist circumference
an dabdominal fat ratio group was
2.24(95%CI:0.87to5.72) and 2.42(95%CI:1.05to5.61), when comparing with those lower group adjusted forage, smoking, alcohol, and MET score. However in analy sison Gleason score of prostate cancer as divided into two groups by Gleason score, no association with waist circumference, but strong positive association with abdominal fat ratio. Therefore I suggests abdominal fat ratio as a good biomarker for not only prostate cancer risk also Gleason score.
Several mechanisms can explain the effect of visceral fat accumulation on increased risk of prostate cancer. Visceral fat is the most metabolically active fat and secretes a variety of hormones and cytokines that affects prostate cancer, containing testosterone, oestrogen, sex hormone-binding globulin, insulin, insulin-like growth factor (IGF)-1, insulin like growth factor binding protein (IGFBP) interleukin-6, leptin and adiponectin6,16). There is evidence that visceral fat
accumulation is associated within sulinres is tance, result inginhyper in sulinemia. High caloricin take, promote the increased high plasmiaand decreased level sof IGFBPs-1and-2. Increased in sulin and decreased level sof IGFBPs -1 and-2 can lead to the development of several different celllines, such as prostate can cerand normal prostate cells, specifically in the early diagnosed prostate cancer18,19).
PSA levels and Gleason score are used to respectively predict pathological stage in prostate cancer patients. Since the stage of cancer differentiation has a profound influence on the expression of serum PSA, used to combine PSA and Gleason score with improved predicting pathologic stage in clinics because of PSA levels may negatively affected by increased BMI20,21).
Recent evidence suggests that PSAl evel was slightly lower among obese men than non obese men (Baillargeonetal.,2005). Because PSA level is regulated by and reogens, which lower PSA levels may result from decreased and rogenicactivity in obese men(Freedlandetal.,2006). The present study also sho wthat PSA levels are lower among overweight and obese men compared with thin men despite larger prostate sizes. Correlation between Gleason pathology score and PSA level is moderate positive relation (r = 0.39, p = 0.01), present correlate with predict pathological stage in prostate cancer. This result show PSA levels alone do not reflect cancer exactly. There are several mechanism can explain the effect of smoking on increased risk of prostate cancer. Smoking may increase bioavailable testosterone and decrease bioavailable estradiol in men, which may be promote cell proliferation in the prostate, in consequence could be associated with malignant transformation (Ferrini and Barrett. 1998). Similar to the testosterone, estrogens play a role on the
hypothalamic-pituitary-gonadal to restrain
excretion of gonadotropins, which may reduce testicular androgen production, and promote
development of prostate cancer (Schatzl et al., 2001). Although reasonable theoretical underlying effects of smoking on prostate cancer, most of outcomes of epidemiological study (23 cohort, 5 nested case-control, 1 retrospective cohort, and 36 case-control studies) found the lack of association between smoking and prostate cancer (Hickey et al., 2001). Result of this study also show that no association between smoking and prostate cancer risk in all subjects (β = 0.01 p = 0.84). The latest evidence suggests that smoking may increase risk of Gleason score, which approximately 30% increase in risk of aggressive prostate cancer when comparing with never smokers (Zu and Giovannucci, 2009). However smoking has still remained inconsistent with Gleason score. This study show a poor association between smoking and prostate cancer Gleason score, when comparing current (categorized as pack-year) with never smokers (β = 0.16 p = 0.25).
The meta-analysis suggests that there is lack of association between alcohol consumption and prostate cancer when identifying studies among articles published from 1976 to 1998, including 77 articles (Dennis, 2000). This study also shows no association between alcohol consumption and prostate cancer when comparing current with never alcohol consumption.
Socioeconomic factors, including education level, leisure, and physical activity do not inverse influence the risk of developing prostate cancer directly with statistical significant in this study. According to previous study, higher education level was significantly inverse risk of prostate cancer (Mills et al 1989). However our study result show that no statistical significant relation between Gleason pathology score and educational attainment (r = - 0.1). In this study, evaluated the association lifestyle factor such as leisure and physical activity were not associated with risk of prostate cancer (β = - 0.1, p = 0.35). According
to review of epidemiologic studies on physical activity and prostate cancer (Friedenreich and Thune. 2001), reported six studies showing a no association and showing no clear relation by type of activity. However in occupational studies
review, job-related physical exertion was
beneficial effect on slight decrease in the risk of
developing prostate cancer than lower
occupational activity (Friedenreich and Orenstein. 2002). Inconsistency across different studies was observed and the magnitude of the effect of physical activity on prostate cancer risk. In this study, cancer patients (3 patients) who drive on the job (over 40 years career)despite a constant exercise and low animal food with high vegetable and fruit intake was higher Gleason score (2 patients: 9(4+5)). May be longtime sedentary life style effect on prostate cancer due to linked to insulin growth factor system (Gr nberg, 2003), although others presented inconsistent with prostate cancer risk (Zeeqers et al, 2004).
A previous related to study report that a positive association between incidence of prostate cancer and increase with age (above 55 years)(Rodriguez et al 2001). Youngest age among prostate cancer patients is 54 years also in this study and similarly age distribution related previous study. But linear regression analysis provide no significant result between Gleason pathological score and prostate cancer patients aging (r=0.18, p = 0.20).
Related with incidence of cancer study was healthy diet (higher fruit and vegetable intake than animal diet), physical activity, occupational life style, and family history alone was not significantly lower risk on prostate cancer
Men with a positive family history of prostate cancer have been definitely known for risk factor. First degree family history (brother or father) that men with prostate cancer have a 2 to 4 fold increased risk of developing prostate cancer and more Gleason score (Bloom et al 2006). Only one
man has first degree of family history among prostate cancer patients in this study. That reason, prostate cancer is unprecedented disease in Korea and may be a given the lack of knowledge about the relatively old patients’ family with prostate cancer. Thus impossible analysis related with family history in this study.
IV. Conclusions
I focused on prostate cancer because this cancers have the most prevalent cancer in Korea, similar good prognosis in the early diagnosis
stage, and hormonally dependent, while
differently expressed and degree of physical impairment (Korean National Cancer Information Center 2014). There are several mechanism can explain the rising incidence of cancers, but these cancer risks can vary over the 10 fold exposure by environment factors. In related evolution study indicate that the breast and prostate cancer appeared with development of mammals, and dietary adaptation to changing Western diet and sedentary life style pattern as evolution, there has been allow insufficient time to biological selection a proper defense for human biology system (Coffey, 2001). There has been an another evident that as people migrate from Asia to the United States, the low risks observed in their mother land begin to rise with spent time and subsequent generations toward those approached incidence level in the general United States population (Shimizu et al., 1991; Grover and Martin, 2002). Also incidence rates of breast and prostate cancer have been rising in South Korea, that factors may result with change in intake of high fat western diet, reproductive patterns, lack of physical activity, obesity, and rising stress level the main contributory factors (Antoni et al., 2006; Stewart et al., 2003; Boyle et al., 2008;
KNHANES 2010; Korean National Cancer
Information Center 2014).
References
1. Ahnmedin, J., Rebecca, S. & Jiaquan, Xu., and Elizabeth, W. 2010. Cancer statics, 2010. Cance r Journal for Clinicians, 60, 227-300.
2. Rodriguez, C., Patel, A. V., Calle, E. E. Jacob s, E. J., Chao, A. &Yhun, M. J. 2001. Body m ass index, height, and prostate cancer mortalit y in two large cohorts of adult men in the Uni ted States. Cancer Epidemiol. Biomark. Prev, 1 0, 345–53.
3. Calle, E. E. & Kaaks, Rudolf. 2004. Overweigh t, obesity and cancer: epidemiological evidence and proposed mechanisms. Nature Reviews Can cer, 4, 579-591.
4. Qu, Y. Y., Dai, B., Kong, Y. Y., Chang, K., Y e, D. W., Yao, X. D., Zhang, S. L., Zhang, H. L. & Yang, W. L. 2013. Influence of obesity on localized prostate cancer patients treated with radical prostatectomy. Asian J Androl, 15, 747 -52.
5. Partin, A. W., Yoo, J., Carter, H. B., Pearson, J. D., Chan, D. W., Epstein, J. I. & Walsh, P. C. 1993. The use of prostate specific antigen, c linical stage and Gleason score to predict patho logical stage in men with localized prostate can cer. J Urol, 150. 110-4.
6. von Hafe, P., Pina, F., Perez, A., Tavares, M. & Barros, H. 2004. Visceral fat accumulation a s a risk factor on prostate cancer. Obes Res, 1, 1930-5.
7. Kelesidis, I., Kelesidis, T. & Mantzoros, C. S. 2006. Adiponectin and cancer: a systematic rev iew. Br J Cancer, 94, 1221-5.
8. Chung, W. H. 2009. Relation of resistin to pro state cancer differentiation and aggressiveness. Korean J Urol, 50, 540-6.
9. Kim, H. J., Lee, Y. S., Won, E. H., Chang, I. H., Kim, T. H., Park, E. S., Kim, M . K., Ki
m, W. & Myung, S. C. 2011. Expression of resi stin in the prostate and its stimulatory effect on prostate cancer cell proliferation. Investigat ive Urology, 108, E77-83.
10. Shimizu, H., Ross, R. K., Bernstein, L., Yata ni, R., Henderson, B. E. & Mack, T. M. 1991. Cancers of the prostate and breast among Jap anese and white immigrants in Los Angeles Co unty, Br J Cancer, 63. 963-6.
11. Grover, P. L. & Martin, F. L. 2002. The initia tion of breast and prostate cancer. Carcinogen esis, 23. 1095-102.
12. Michaud, D. S., Augustsson, K., Rimm, E. B., Stampfer, M. J., Willet, W. C. & Giovannucci, E. 2001. A prospective study on intake of ani mal products and risk of prostate cancer. Can cer Causes Control, 12, 557-67.
13. Hayes, R. B., Zieqler, R. G., Gridley, G., Swa nson, C., Greenberg, R. S., Swanson, G. M., Schoenberg, J. B., Silverman, D. T., Brown, L. M., Pottern, L. M., Liff, J., Schwartz, A. G. Fraumeni, J. F Jr. & Hoover, R. N. 1999. Dietary factors and risks on prostate cancer a mong blacks and whites in the United States. Cancer Epidemiol Biomarkers Prev, 8. 25-34. 14. Cohen, J. H., Kristal, A. R. & Stanford, J. L.
2000. Fruit and vegetable intakes and prostate cancer risk. J Natl Cancer Inst, 92, 61-8. 15. Prakash, P., Russell, R. M. & Krinsky, N. I.
2001. In vitro inhibition of proliferation of estrogen-dependent and estrogen- independen t human breast cancer cells treated with carot enoids or retinoids. J Nutr, 131, 1574-1580. 16. Jian, L., Du, C. J., Lee, A. H. & Binns, C.
W. 2005. Do dietary l ycopene and other carot
enoids protect against prostate cancer?. Int J Cacner, 113, 1010-4.
17. Bosetti, C., Spertini, L., Parpinel, M., Gnagna rella, P., Lagjou, P, Negri, E., Franceschi, S., Montella, M., Peterson, J., Dwyer, J., Giacos a, A. & La, Vecchia. C. 2005. Flavonids and b reast cancer risk in Italy. Cancer Epidemiol Bi omarkers Prev, 14, 805-8.
18. Stattin, P., Bylund, A., Rinaldi, S. & Biessy, C. D chaud, H., Stenman, U. H., Egevad, L., Riboli. E., Hallmans, G. & Kaaks, R. 2000. Pl asma insulin-like growth factor-I, insulin-lik e growth factor-binding proteins, and prostat e cancer risk: a prospective study. J Natl Can cer Inst, 92, 1910-7.
19. Allen, N. E. & Key, T. J. 2001. Plasma insuli n like growth factor-1, insulin like growth fa ctor binding proteins, and prostate cancer ris k: a prospective study. J Natil Cancer Inst, 9 3, 649-51.
20. Freedland, S. J., Platz, E. A., Presti, J. C., Aronson, W. J., Amling, C. L., Kane, C. J. & Terris, M. K. 2006. Obesity, serum prostate s pecific antigen and prostate size: implications on prostate cancer detection. J Urol, 175, 500 -4.
21. Ba ez, L. L., Hamilton, R. J., Partin, A. W., Vollmer, R. T., Sun, L., Rodriguez, C., Wang, Y., Terris, M. K., Aronson, W. J., Presti, J. C Jr., Kane, C. J., Amling, C. L., Moul, J. W. & Freedland, S. J. Obesity-related plasma hemodilutin and PSA concentration among men with prostate cancer. JAMA, 298, 2275-80.