Bone regeneration of biphasic calcium
phosphate with varying methods of material
preparation in rabbit calvarial defect
Kyeong-Taek Kim
The Graduate School
Yonsei University
Department of Dental Science
Bone regeneration of biphasic calcium
phosphate with varying methods of material
preparation in rabbit calvarial defect
Directed by Professor: Seong-Ho Choi
A Master's Thesis
submitted to the Department of Dentistry
the Graduate School of Yonsei University
in partial fulfillment of the requirements for the degree of
Master of Dental Science
Kyeong-Taek Kim
This certifies that the Master’s thesis
of Kyeong-Taek Kim is approved.
─────────────────
Thesis Supervisor : Seong-Ho Choi
─────────────────
Jung-Kiu Chai
─────────────────
Ui-Won Jung
The Graduate School
Yonsei University
감사의 글
이번 논문을 쓰기까지 훌륭하신 인격으로 하나하나 감수해 주시고,
해맑은 마음으로 아낌없이 지도 해 주신 최성호 지도교수님께 진정
으로 깊은 감사를 드립니다. 그리고 진심 어린 조언과 따뜻한 관심
으로 지켜봐 주신 채중규 교수님, 정의원 교수님, 이중석 교수님께
감사의 마음을 전합니다.
연구 내내 많은 도움을 준 치주과 의국원들과 장명란 연구원에게
도 고마움을 전합니다.
마지막으로 늘 저와 함께 해주고, 격려해주시고, 지지해준 부모님
과 형제에게 고마움과 기쁨을 전하고 싶습니다. 이 지면을 통해 인
사드리지 못한 보훈병원 박필규 부장님, 전문의 선생님들께도 진심
으로 감사드립니다. 항상 겸손한 사람이 되도록 하겠습니다.
2013년 6월
저자 씀
i
TABLE OF CONTENTS
List of figures and tables ···iii
Abstract (English) ··· iv
I. INTRODUCTION ··· 1
II. MATERIALS AND METHODS··· 4
1. Prepartaion of the experimental materials ··· 4
2. Anima ls ··· 5
3. Study des ign ··· 6
4. Surgical procedures ··· 6
5. XRD and SEM measurements ··· 7
6. Histologic processing and histometric measurements ··· 7
7. Ana lys is met hod ···8
8. Statist ical analys is ··· 8
III. RESULTS··· 10
1. Clinical observat ion··· 10
2. Histologic finding ··· 10
3. Histometric finding ··· 11
IV. DISCUSSION··· 13
V. CON CL US IO N· · · 17
R E FE R E N C E S · · · 1 8
LEGENDS ··· ··· ··· ··· ··· ··· ··· ··· 23
ii
FIGU RES· · · ·· · · · ·· · · · ·· · · ·· · · · ·· · · · ·· · · ·· · · · ·· · · ·· · · ·· · · · ·· · · · ·· · · ·· · · · ·· 25
TAB LES ··· ··· ··· ··· ··· ··· ··· ··· ··· 29
ABSTRACT (IN KOREAN) ··· 30
iii
List of Figures and Tables
Figure 1. Scheme of processing routes used for the production of
biphasic calcium phosphate(BCP)···25
Figure2. X-ray diffraction patterns profile of biphasic calcium
phosphate(BCP)··· 25
Figure 3. SEM photomicrograph of biphasic calcium
phosphate(BCP)··· 26
Figure 4. Clinical photographs of defect preparation in rabbit
calvaria ··· 26
Figure 5. Representative photomicrographs of defect sites receiving
the biphasic calcium phosphate(BCP) at 2 weeks
pos ts urgery ···· ··· ···· ···· ···· ···· ··· ···· ·· ··· ···· ···· ·27
Figure 6. Representative photomicrographs of defect sites receiving
the biphasic calcium phosphate(BCP) at 8 weeks
pos ts urgery ···· ··· ···· ···· ···· ···· ··· · ··· ·· ··· ···· ···· ·28
Table 1. Amounts of new bone, biphasic calcium phosphate(BCP)
as percentages of the augmented area at 2 and 8 weeks
pos ts urgery··· ··· ···29
iv
ABSTRACT
Bone regeneration of biphasic calcium phosphate with varying
methods of material preparation in rabbit calvarial defect
Kyeong-Taek Kim, D.D.S.
Department of Dentistry theGraduate School, Yonsei University
(Directed by Professor Seong-Ho Choi, D.D.S., M.S.D., PhD.)
The purpose of this study is to compare and evaluate the bone regeneration effect and histological result of BCP(biphasic calcium phosphate) with varying methods of material preparation in rabbit calvarial defect. Ten adult male New Zealand rabbits were used in the experiment. Four defects with diameter of 8mm each were formed at the rabbit calvaria and BCPs manufactured with each different material preparation methods were applied in three defects.
A BCP used in the first coating group was prepared by coating beta-tricalcium phosphate on HA scaffold surface manufactured with Replica method. The second BCP used in the sacrificial group was prepared by manufacturing biphasic scaffold with sacrificial template method and the third BCP in the foaming group by manufacturing biphasic scaffold with direct foaming method.
v
Four defects were classified as the followings. Group 1(control): bone grafts not applied, Group2 (Coating group): BCP preparation method was replica method and the ratio of hydroxyapatite/beta-tricalcium phosphate (HA/β-TCP) was 7:3. Group3 (Sacrificial group): BCP preparation method was Sacrificial template method and the ratio of HA/β-TCP was 3:7. Group4 (Foaming group): BCP preparation method was direct foaming method and the ratio of HA/β-TCP was 2:8. The animals used in the experiment were sacrificed at 2 week(N=5) and 8 week(N=5).
In the histological and histometric measurement results, BCPs used in the three groups showed high space maintenance ability and stability of particles. Compared to the coating group, the sacrificial group and foaming group showed significantly high bone graft resorption rate and especially in the foaming group the largest bone graft resorption rate was shown at 2 and 8 week period and bone regeneration was very even. However, no significant statistical difference in resorption rate and bone regeneration between sacrificial and foaming groups was shown.
Keywords: beta-tricalcium phosphate, biphasic calcium phosphate, bone regeneration,
1
Bone regeneration of biphasic calcium phosphate with varying
methods of material preparation in rabbit calvarial defect
Kyeong-Taek Kim, D.D.S.
Department of Dentistry theGraduate School, Yonsei University
(Directed by Professor Seong-Ho Choi, D.D.S., M.S.D., PhD.)
I. Introduction
Various procedures were introduced currently for regeneration of bone defects in implant and periodontal surgery area. In many procedures, bone grafts were used for acceleration of bone regeneration. (Becker & Becker, 1993; Cortellini, Pini Prato, Baldi, & Clauser, 1990; Greenstein & Caton, 1993; LeGeros, Lin, Rohanizadeh, Mijares, & LeGeros, 2003; Sculean et al., 1999)
As bone grafts, autograft, allograft, xenograft and synthetic graft are present. Among them, the autograft shows the highest ability of bone regeneration compared to other grafts, which makes it still “the Gold Standard”. (Nampo et al., 2010)However, various side effects such as limited donor sites when harvesting, post-operative pain and discomforts of patients and nerve injury may occur.(Raghoebar, Meijndert, Kalk, & Vissink, 2007)Therefore, recently, new synthetic bones similar to
2
autografts are under development. These grafts should have fine biocompatibility to minimize tissue reaction and high biodegradability to be replaced by newly formed bone. Also, they should be osteoconductive and osteoinductive. However, the bone
regeneration effect is unsatisfactory yet due to the deficiency of
osteoinductivity.(Jensen et al., 1996)
Initially, HA particles provided scaffold for new bone regeneration without causing infection. However, it failed to show evidence of bone regeneration when used alone according to various studies. On the other hands, β-TCP showed bone regeneration in the defect though unpredictable level of resorption occurred within body.(Froum, Kushner, Scopp, & Stahl, 1982; Jarcho, 1981; Moskow & Lubarr, 1983)Therefore, bone regeneration with fine predictability may be difficult to be shown in only HA and β-TCP.Biphasic calcium phosphate (BCP) have been known widely as synthetic bone grafts composed of hydroxyapatite (HA) and beta-tricalcium phosphate (β-TCP). (Monroe, Votava, Bass, & McMullen, 1971)Presently, many studies are reporting good results with BCPs in bone defect regeneration instead of other bone grafts.(Jung et al., 2006; LeGeros et al., 2003; Um et al., 2008)
BCPs are synthesized under the temperature of 700’C or above or manufactured by sintering apatite which is short of calcium biologically. The level of calcium deficiency is decided by manufacturing methods including pH reaction and temperature. The ratio of HA/β-TCP depends on sintering temperature and the level of calcium deficiency of unsintered apatite.(LeGeros, 1991)The biologic reaction of bone grafts is associated with chemical composition, its macro- and micro structural
3
characteristics such as pore size, porosity and interconnecity (LeGeros et al., 2003) and also the manufacturing method. Initially, LeGeros reported bioactivity could be controlled by changing the ratio of HA/β-TCP in a study comparing various ratio of HA/β-TCP in BCP. (Nery, LeGeros, Lynch, & Lee, 1992)There was also a study comparing degradation rate of the mechanically mixed BCP and HA/ β-TCP powder or apatite short of calcium manufactured in calcination methods.(Gauthier et al., 1999)In the other studies, bioactivity was compared by manufacturing BCP in different forms(particle and block). (Kim et al., 2011; Schwarz et al., 2008)
However, few studies showed the effect of BCP manufactured with different material preparation methods. The purpose of this study is to evaluate histological analysis and bone formation results in rabbit calvarial defects depending on the material preparation methods.
4
II. Materials & Methods
1. Preparation of the experimental materials
Three BCPswere used in this study.Three groups are as the following:
1. Coating group(OSTEON I, Genoss, CO., Ltd, Suwon, Korea);HA scaffold coated by β-TCP with a ratio of HA/β-TCP = 70/30, a pore size of 300 to 500µm and a porosity of 77%):HA scaffold is manufactured using replica method. To form porous ceramic structure, a copy should be made by impregnating cellular structure in the same form as the present porous sponge at the precursor solution or ceramic suspension. After that, β-TCP is coated on HA scaffold surface. [Fig. 1(a)](Soon-Ho Kwon, 2002)
2. Sacrificial group (OSTEON II, Genoss, CO., Ltd, Suwon, Korea); (BCP with a ratio of HA/β-TCP = 30/70, a pore size of 250 µm, and a porosity of 70%): Biphasic scaffold is manufactured usingsacrificial template method. Sacrificed material is dispersed into the same tissue through sacrificial procedure inside biphasic scaffold which has the solid or liquid form composed of continuous matrix of ceramic particles or ceramic precursors. After drying, through thermal decomposition and sintering procedure, porous structure is formed inside the microstructure by removal of sacrificed material. [Fig. 1( b)](Byung-Ho Yoon, 2007)
5
3. Foaming group (BCP with a ratio of HA/β-TCP = 20/80, a pore size of 200 to 400 µm, and a porosity of 80%): Biphasic scaffold is manufactured using direct foaming method.By incorporating gas into ceramic precursor or suspension in the form of liquid, porous structure is manufactured and through drying and sintering process, the structure formed by gas bubbles becomes fixed.[Fig. 1( c)](Andre R. Studart, 2006)
Fig.2 show typical XRD patterns of BCP respectively. Representative peaks of HA and β-TCP are marked with symbols. HA/β-TCP ratios for BCP were roughly (A) 70:30, (B) 30:70, and (C) 20:80 calculated by comparison of the highest peak of each phase (HA: 31.8°, β-TCP: 31.0°). Fig. 3 shows typical microstructures of BCP respectively.All the images show well-interconnected pore structure with different pore shape and size. Coating group BCP [Fig. 3(A)] made by replica method has relatively thicker strut and larger pore size of 300~500 μm. TCP70 group BCP [Fig. 3(B)] by sacrificial template method shows ellipsoidal pores of ~250 μm. TCP80 group BCP [Fig. 3(C)] by direct foaming method has large spherical concave structure with a pore size of 200 to 400 µm.
2. Animals
Ten adult male New Zealand white rabbits weighing 2.5 to 3.5 kg were used in this study. The animals were kept in individual cages and fed a standard diet. The animal
6
care, selection and preparation of surgical protocols were permitted by Institutional Animal Care and Use Committee, Yonsei Medical center, Seoul, Korea (2012-0030))
3. Study design
Four circular defects with diameter of 8mm were formed in rabbit calvaria and then three were filled with a BCP with different manufacturing method. The remaining defect was filled with a blood clot (Fig. 4).
1. Control group: defects were left unfilled.
2. Coating group: defects were filled with BCP with HA/β-TCP ratio 7:3 3. Sacrificial group: defects were filled with BCP with HA/β-TCP ratio 3:7 4. Foaming group: defects were filled with BCP with HA/β-TCP ratio 2:8
4. Surgical procedures
All animals were anesthetized using intramuscular injection of the mixture of ketamine hydrochloride (Ketalar, Yuhan, Seoul, Korea) and one from Rompun(Bayer Korea, Seoul, Korea).The surgical site was shaved and disinfected with
povidone-iodine before the operation, followed by local anesthesia with 2%
lidocaine(LidocaineHCl, Huons, Seoul, Korea). An incision was made along the media of the calvarium in each animal. After the anesthesia, a full layered flap was
7
evaluated and trephine bur was used to form circular bone defect with a diameter of 8mm under enough saline irrigation.Each of three of the defects was filled with BCP with different manufacturing method. And the control defect was left unfilled. (Fig. 4) (Sohn et al., 2010)The flaps were repositioned and sutured with resorbable suture material. The animals were sacrificed at 2 weeks and 8 weeks postsurgery.
5. XRD and SEM measurements
The crystalline phase of the BCP was analyzed by X-ray diffractometry (XRD, RigakuUltima III, Japan). XRD spectra were collected over the 2θ range of 20–60° by using monochromatic Cu Kα radiation (40 kV, 200mA). The intensity of main peak (HA: 31.8°, β-TCP: 31.0°) was used to calculate the HA/β-TCP content. The microstructure of the samples was analyzed by scanning electron microscopy (SEM, Tescan Vega II LSH, USA) at 20kV.
6. Histological processing and histometric measurements
Block sections of the surgical site were fixed in 10% formalin for 10 days. Then, the section were decalcified in 5% formic acid for 14 days and then embedded in paraffin. Serial 5- µm thick sections were cut through the center of the circular
8
calvarial defects. Each block was stained with hematoxylin and eosin (H&E) and histometric analysis was performed.
7.
Analysis method
Clinical findings; Visual observation were performed after 2 and 8 weeks of healingHistological Analysis; Histologic slides were examined using binocular microscope (Leica DM LB, Leica Microsystems, Wetzlat, Germany) equipped with camera (Leica DC300F, Leica Microsysytems, Heerbrugg, Switzerland) and photographed slide images were saved as JPEG file each.
Histometric Analysis; Image analysis computer program (Image-Pro Plus, Media Cybernetics, Sliver Spring, MD, USA) was used for histometric analysis in which augmented area and new bone area were measured.
8. Statistical analysis
Statistical analysis was performed using commercially available software(SPSS 15.0, SPSS, Chicago, IL) and means ± standard deviation (SD) of histometric measurement record per calvaria defect sample was measured.To compare significant difference between groups, Kruskal-Wallis test (P<0.05) analysis was used and the
9
Mann-Whitney test was also used to compare the difference between 2 week and 8 week period. The level of statistical significance was set at p<0.05
10
III. Results
1. Clinical observation
Healing was achieved without any side effects in all animals during the post-operation period.
2. Histologic finding
In the control group, the defect area was filled with some newly formed bone and loose connective tissue. On the margin of defect area, slight bone regeneration into the center was observed. A thin layer of bone formation was observed on the margins of all defects at 2 and 8 week group.[Fig. 5 (A) and 6 (A)]
In the coating group, relatively at the 2 week group, large particles of grafts were observed on the central area of defects. On the other hand, at the 8 week group, small particles of grafts were observed in the center and the defect area was replaced by resorption and newly formed bone to show more bone formation. Also, compared to the 2 week group, augmented area is observed to maintain. [Fig. 5 (C) and 6 (C)]
In the sacrificial group, connective tissue and newly formed bone are observed and at the 2 week group, a lot of capillaries are observed. At the 8 week group, more bone formation was shown than that at the 2 week group not only at the margin but
11
also on the center and newly formed bone are observed to surround the marginal area of bone grafts partly. Compared to the coating group, no difference in the size and resorption rate of particles of bone grafts located within the defect area seems to be shown. [Fig. 5 (E) and 6 (E)]
In the foaming group, relatively small particles of bone grafts are observed compared to those in other groups. Each particle is mostly surrounded by various amounts of newly formed bone. At the 2 week group, bone regeneration stopped on the margin, however, at the 8 week group, even bone regeneration was achieved in every defect area through remodeling process in which particles are combined with mature bone and become resorbed.[Fig. 5 (G) and 6 (G)]
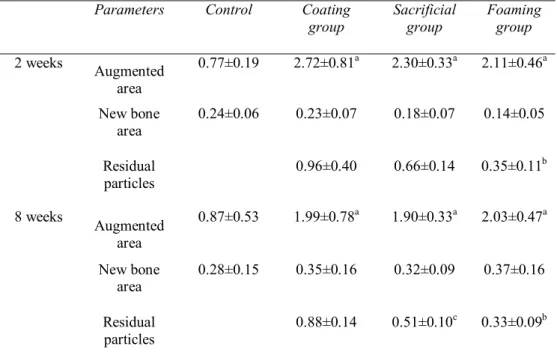
3. Histometric finding
Bone regeneration progressed from the margin into the central area and through osteoconduction process, it occurred from the present bone to the graft. Histometric analysis is shown in Table I. Bone area, residual particles, augmented total area were measured. Total augmented area including soft tissues, residual particles and augmented bone were all high in all the experimental groups, the coating, sacrificial and foaming group at 2 and 8 week period group compared to the control group.
The size of newly formed bone area was larger at the 8 week period group than that at the 2 week group in all the experimental group and was significantly larger in the sacrificial and foaming group. In all the experimental groups, resorption of bone
12
grafts seems to occur since the size of residual particle area decreased at the 8 week period group compared to the 2 week period group. At the 2 week period group, resorption rate was significantly higher in the foaming group compared to that in the coating group and at the 8 week period group, the sacrificial and foaming groups showed significantly higher resorption rate than the coating group. No significant difference in graft resorption rate was shown between all sacrificial and foaming group at the 2 and 8 week period group(Table I).
13
IV. Discussion
The present study was designed to compare the bone formation effect and histological result of BCP with varying methods in rabbit calvarial defect. The three types of bone grafts used in the experimental group all had osteoconductive characteristics and showed direct contact between newly formed bone and the grafts. Even in other studies, BCP was reported to accelerate formation of new bone in the rabbit calvarial defects.(Park et al., 2009)
For evaluation of effect of newly developed biomaterials, rats, monkeys, rabbits and other various animals are in use and radius, mandible and cranium can be defect sites in which these materials can be applied. Among them, a rabbit calvarial defect is widely used in evaluation of bone regeneration effect.(Sohn et al., 2010)In many studies, various critical size defect(CSD) are suggested, (Schmitz & Hollinger, 1986; Shand, Heggie, Holmes, & Holmes, 2002)however, in this present study, the defect with the size of 8mm was used.The defect of 8mm is suggested to be enough size for evaluation of bone regeneration effect of bone grafts though it is smaller than CSD which is known as 10-15mm presently.(Sohn et al., 2010)Also, tissue pattern is observed differently depending on healing time period. A two week period is appropriate for evaluation of initial stage of healing reaction such as host reaction or bone graft stability and a 8 week period is for evaluation of post- stage reaction such as bone graft resorption, bone remodeling. Therefore, comparison analysis was performed with 2 and 8 week period groups.
14
Histologic and histometric results showed that all the three types of BCP maintain the space better than that in the control group. In the control group where no treatment was done, the defect area was shown to be compressed. On the other hand, in the experimental group, augmented volume for 2 and 8 weeks maintained. Histometrically, even, the total augmentation area including soft tissue and newly formed bone was significantly higher.
At the 2 week period group, the resorption rate of graft particles in the foaming group was significantly higher than that in the coating group. At the 8 week group, the resorption rates of the foaming and sacrificial group were significantly higher compared to that in the coating group. This result may be due to low solubility of porous HA, high resorption rate of β-TCP, (Jung et al., 2006)and each different material preparation methods. The bone grafts in the foaming group showed more rapid resorption rate even from the initial stage of healing reaction.The bone quality may be low due to residual particles, however, the residual particles and soft tissue are reported to affect cell differentiation, mature, revascularization and bone regeneration.(Um et al., 2008)Previous studies found that at the initial stage where tissue remodeling occurs after extraction, immature bone and provisional connective tissue are replaced by bone marrow and lamellar bone as time goes.(Cardaropoli, Araujo, & Lindhe, 2003; Lindhe, Cecchinato, Donati, Tomasi, & Liljenberg, 2013)For evaluation of above experimental results, the long-term period study and observation is considered to be necessary.
15
Though no significant statistical difference among resorption rates of the foaming and sacrificial group, and among augmented amounts of newly formed bone were shown, histologically, relatively small particles were observed in the foaming group compared to the sacrificial group and due to its high resorption rate and high porosity, bone grafts were observed to be surrounded by various newly formed bone. Also, even bone regeneration was observed in all area of defects.
In studies where the amount of bone grafts was large in implant surgeries, BCP manufactured with chemical composition similar to bone apatite biologically showed fine bone reconstruction result. Also, in many animal and human clinical tests, the effect of bone grafts is being approved. (Jung et al., 2006; Lee, Jung, Kim, Choi, & Cho, 2006)In other studies, unpredictable bone resorption results were shown when HA or β-TCP was used alone.(LeGeros et al., 2003)however, HA/β-TCP composites showed a little better bioactivity.Though there are reported studies evaluating bioactivity and resorption rates by controlling HA/β-TCP ratio, (LeGeros, 1991)the ratio for an ideal osteoconductivity is controversial. (Ebrahimi, Pripatnanont, Monmaturapoj, & Suttapreyasri, 2012)Yet, BCPs with many other preparation methods have not been introduced. LeGeros et al compared degradation of a group where calcium-deficient apatite was manufactured in calcination methods and a BCP group where the BCP with the same HA/β-TCP and porosity was mechanically mixed at the rabbit calvaria. In the group manufactured in calcination method, better resorption rate was observed by difference in biphasic structure and the presence of impurities since it went through elaboration process.(Gauthier et al., 1999)
16
This study showed how the ratio of HA/β-TCP and various preparation methods affect biologic reaction of bone grafts. BCPs within bone defect area had fine biocompatibility and had a good ability to maintain augmented area. Bone grafts in the foaming group showed relatively higher rate of resorption compared to other experimental groups and showed histologically even bone regeneration. Though some limits in the experimental results exist due to the difference in the ratio of HA/β-TCP between sacrificial and foaming groups, difference in porosity depending on material preparation methods of the grafts may be considered to affect the resorption ability of the material and bone regeneration. Further studies using BCPs of the same ratio of HA/β-TCP, manufactured in different preparation methods are considered to be necessary to evaluate the most proper preparation methods which maximize biocompatibility and osteoconductivity of BCP.
17
V. Conclusion
BCPs used in the three groups showed high space maintenance ability and stability of particles. Compared to the coating group, the sacrificial group and foaming group showed significantly high bone graft resorption rate and especially in the foaming group the largest bone graft resorption rate was shown at 2 and 8 week period and bone regeneration was very even. However, no significant statistical difference in resorption rate and bone regeneration between sacrificial and foaming groups was shown
18
References
Andre R. Studart, U. T. G., Elena Tervoort, Ludwig J. Gauskler. (2006). Processing routes to macroporous ceramics: A review. Journal of the american ceramic
society, 89(6), 1771-1789.
Becker, W., & Becker, B. E. (1993). Clinical applications of guided tissue regeneration: surgical considerations. Periodontol 2000, 1, 46-53.
Byung-Ho Yoon, Y.-H. K., Chee-Sung Park, Hyoun-Ee Kim. (2007). Generation of large pore channels for bone tissue engineering using camphene-based freeze casting. Journal of the american ceramic society, 90(6), 1744-1752.
Cardaropoli, G., Araujo, M., & Lindhe, J. (2003). Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J Clin Periodontol,
30(9), 809-818.
Cortellini, P., Pini Prato, G., Baldi, C., & Clauser, C. (1990). Guided tissue regeneration with different materials. Int J Periodontics Restorative Dent,
10(2), 136-151.
Ebrahimi, M., Pripatnanont, P., Monmaturapoj, N., & Suttapreyasri, S. (2012). Fabrication and characterization of novel nano hydroxyapatite/beta-tricalcium phosphate scaffolds in three different composition ratios. J Biomed Mater Res
19
Froum, S. J., Kushner, L., Scopp, I. W., & Stahl, S. S. (1982). Human clinical and histologic responses to Durapatite implants in intraosseous lesions. Case reports. J Periodontol, 53(12), 719-725.
Gauthier, O., Bouler, J. M., Aguado, E., Legeros, R. Z., Pilet, P., & Daculsi, G. (1999). Elaboration conditions influence physicochemical properties and in vivo bioactivity of macroporous biphasic calcium phosphate ceramics. J
Mater Sci Mater Med, 10(4), 199-204.
Greenstein, G., & Caton, J. G. (1993). Biodegradable barriers and guided tissue regeneration. Periodontol 2000, 1, 36-45.
Jarcho, M. (1981). Calcium phosphate ceramics as hard tissue prosthetics. Clin
Orthop Relat Res(157), 259-278.
Jensen, S. S., Aaboe, M., Pinholt, E. M., Hjorting-Hansen, E., Melsen, F., & Ruyter, I. E. (1996). Tissue reaction and material characteristics of four bone substitutes.
Int J Oral Maxillofac Implants, 11(1), 55-66.
Jung, U. W., Choi, S. Y., Pang, E. K., Kim, C. S., Choi, S. H., & Cho, K. S. (2006). The effect of varying the particle size of beta tricalcium phosphate carrier of recombinant human bone morphogenetic protein-4 on bone formation in rat
calvarial defects. J Periodontol, 77(5), 765-772. doi:
10.1902/jop.2006.050268
Kim, J. W., Choi, K. H., Yun, J. H., Jung, U. W., Kim, C. S., Choi, S. H., & Cho, K. S. (2011). Bone formation of block and particulated biphasic calcium phosphate lyophilized with Escherichia coli-derived recombinant human bone morphogenetic protein 2 in rat calvarial defects. Oral Surg Oral Med Oral
20
Pathol Oral Radiol Endod, 112(3), 298-306. doi:
10.1016/j.tripleo.2010.10.025
Lee, J. H., Jung, U. W., Kim, C. S., Choi, S. H., & Cho, K. S. (2006). Maxillary Sinus
Augmentation Using Macroporous Biphasic Calcium Phosphate
(MBCP(TM)): Three Case Report With Histologic Evaluation. J Korean
Acad Periodontol, 36(2), 567-577.
LeGeros, R. Z. (1991). Calcium phosphates in oral biology and medicine. Monogr
Oral Sci, 15, 1-201.
LeGeros, R. Z., Lin, S., Rohanizadeh, R., Mijares, D., & LeGeros, J. P. (2003). Biphasic calcium phosphate bioceramics: preparation, properties and applications. J Mater Sci Mater Med, 14(3), 201-209.
Lindhe, J., Cecchinato, D., Donati, M., Tomasi, C., & Liljenberg, B. (2013). Ridge preservation with the use of deproteinized bovine bone mineral. Clin Oral
Implants Res. doi: 10.1111/clr.12170
Monroe, E. A., Votava, W., Bass, D. B., & McMullen, J. (1971). New calcium phosphate ceramic material for bone and tooth implants. J Dent Res, 50(4), 860-861.
Moskow, B. S., & Lubarr, A. (1983). Histological assessment of human periodontal defect after durapatite ceramic implant. Report of a case. J Periodontol, 54(8), 455-462.
Nampo, T., Watahiki, J., Enomoto, A., Taguchi, T., Ono, M., Nakano, H., . . . Maki, K. (2010). A new method for alveolar bone repair using extracted teeth for
21
the graft material. J Periodontol, 81(9), 1264-1272. doi:
10.1902/jop.2010.100016
Nery, E. B., LeGeros, R. Z., Lynch, K. L., & Lee, K. (1992). Tissue response to biphasic calcium phosphate ceramic with different ratios of HA/beta TCP in periodontal osseous defects. J Periodontol, 63(9), 729-735.
Park, J. C., Lim, H. C., Sohn, J. Y., Yun, J. H., Jung, U. W., Kim, C. S., . . . Choi, S. H. (2009). Bone regeneration capacity of two different macroporous biphasic calcium materials in rabbit calvarial defect. J Korean Acad Periodontol,
39(Suppl), 223-230. doi: 10.5051/jkape.2009.39.S.223
Raghoebar, G. M., Meijndert, L., Kalk, W. W., & Vissink, A. (2007). Morbidity of mandibular bone harvesting: a comparative study. Int J Oral Maxillofac
Implants, 22(3), 359-365.
Schmitz, J. P., & Hollinger, J. O. (1986). The critical size defect as an experimental model for craniomandibulofacial nonunions. Clin Orthop Relat Res(205), 299-308.
Schwarz, F., Rothamel, D., Herten, M., Ferrari, D., Sager, M., & Becker, J. (2008). Lateral ridge augmentation using particulated or block bone substitutes biocoated with rhGDF-5 and rhBMP-2: an immunohistochemical study in dogs. Clin Oral Implants Res, 19(7), 642-652. doi: 10.1111/j.1600-0501.2008.01537.x
Sculean, A., Donos, N., Windisch, P., Brecx, M., Gera, I., Reich, E., & Karring, T. (1999). Healing of human intrabony defects following treatment with enamel matrix proteins or guided tissue regeneration. J Periodontal Res, 34(6), 310-322.
22
Shand, J. M., Heggie, A. A., Holmes, A. D., & Holmes, W. (2002). Allogeneic bone grafting of calvarial defects: an experimental study in the rabbit. Int J Oral
Maxillofac Surg, 31(5), 525-531. doi: 10.1054/ijom.2002.0281
Sohn, J. Y., Park, J. C., Um, Y. J., Jung, U. W., Kim, C. S., Cho, K. S., & Choi, S. H. (2010). Spontaneous healing capacity of rabbit cranial defects of various sizes.
J Periodontal Implant Sci, 40(4), 180-187. doi: 10.5051/jpis.2010.40.4.180
Soon-Ho Kwon, Y.-K. J., Seong-Hyeon Hong, In-Seop Lee, Hyoun-Ee Kim, Ye Yeon Won. (2002). Calcium phosphate bioceramics with various porosities and dissolution rates. Journal of the american ceramic society, 85(12), 3129-3131.
Um, Y. J., Hong, J. Y., Kim, S. T., Lee, Y. H., Park, S. H., Park, S. H., . . . Choi, S. H. (2008). Bone formation of newly developed biphasic calcium phosphate in rabbit calvarial defect model: A pilot study. J Korean Acad Periodontol,
23
Legends
Figure 1. Scheme of possible processing routes used for the production of
macroporous ceramics. The figure is reproduced from (Andre R. Studart, 2006), with permission from the American Ceramic Society.
Figure 2. X-ray diffraction patterns profile: (A) BCP, mixture of HA and β-TCP
(HA/β-TCP=80/20), obtained by replica method. (B) BCP, mixture of HA and β-TCP (HA/β-TCP=70/30), obtained by sacrificial template method. (C) BCP, mixture of HA and β-TCP (HA/β-TCP=20/80), obtained by direct foaming method
Figure 3. SEM photomicrograph of BCP: (A) Coating group (B) Sacrificial group(C)
Foaming group
Figure 4. Clinical photographs of defect preparation (A) Four 8-mm-diameter defects
were made in rabbit calvaria. (B) BCP with different manufacturing method (1) Coating group (2) Sacrificial group (3) Foaming group
Figure 5. Representative photomicrographs obtained at 2-weeks postsurgery. (A,B)
24
Foaming group. (H&E stain; original magnification: x40. [A,C,E,G] original magnification: x100. [B,D,F,H])
Figure 6. Representative photomicrographs obtained at 8-weeks postsurgery. (A,B)
Control group; (C,D) Coating group; (E,F) Sacrificial group; (G,H) Foaming group. (H&E stain; original magnification: x40. [A,C,E,G] original magnification: x100. [B,D,F,H])
25
Figures
Figure 1
26 Figure 3
27 Figure 5 A B C D E F H G NB OB OB OB NB NB NB
28 Figure 6 A E C G D F H B OB NB NB NB NB
29
Tables
Table I. Histometric results after 2 and 8weeks of healing. (n=5) (Mean ±
Standard Deviation values; n= number of specimens)
Parameters Control Coating
group Sacrificial group Foaming group 2 weeks Augmented area 0.77±0.19 2.72±0.81a 2.30±0.33a 2.11±0.46a New bone area 0.24±0.06 0.23±0.07 0.18±0.07 0.14±0.05 Residual particles 0.96±0.40 0.66±0.14 0.35±0.11b 8 weeks Augmented area 0.87±0.53 1.99±0.78a 1.90±0.33a 2.03±0.47a New bone area 0.28±0.15 0.35±0.16 0.32±0.09 0.37±0.16 Residual particles 0.88±0.14 0.51±0.10c 0.33±0.09b a
Statistically significant difference compared to corresponding control group (p<0.05) b
Statistically significant difference compared to Foaming group (P<0.05) c
30 국문요약
백서 두개골 결손부에서 Biphasic Calcium Phosphate 제작방법에
따른 골 형성 효과 비교
<지도교수 최성호>
연세대학교 대학원 치의학과
김경택
이상칼슘 포스페이트는 골이식재로서 그 효과가 이미 입증되어있다. 그러나 칼슘 포스페이트 제작방법에 따른 효과를 비교한 연구는 많지 않다. 이 연구의 목적은 다양한 제작 방법을 이용한 이상 칼슘 포스페이트를 백서 두개골에 적용하여 골 형성 효과와 조직학적 결과를 평가하는 것이다. 총 10 마리의 백서를 4 군으로 나누어 실험을 시행하였으며, 모든 동물에서 두개골 부위 직경 8mm 의 골결손부를 형성하였다. 각각의 군은다음과 같으며 (1) Control group, (2) Coating group, (3) Sacrificial group (4) Foaming group, 2 주와 8 주의 치유 기간 후 희생하여 조직학적 및 조직계측학적 정량분석을 시행하였다.Coating 군에 적용한 칼슘 포스페이트는인회석(hydroxyapatite) 비계를
31
포스페이트는 희생 형판 방식(Sacrificial template method), Foaming 군의 칼슘 포스페이트는 직접 거품 방식(Direct foaming method)를 적용하였다.
모든 실험군에서 칼슘 포스페이트는 대조군에 비해 증가된 공간을 안정적으로 더 잘 유지하였다. Coating 군과 비교해서 Sacrificial 군과 Foaming 군은 높은 흡수율을 보여주었다. Sacrificial 군과 Foaming 군간 흡수율에 있어 통계적 유의적 차이점은 없었으나 높은 다공성을 보이는 Foaming 군의 이식재는 2 주와 8 주에서 가장 많은 흡수율을 보였다. 조직학적으로 Foaming 군 이식재가 상대적으로 작은 입자와 결손부내 고른 골재생을 보였다. 이 연구를 통해, 칼슘 포스페이트는 제조 방식에 의해서도 골재생 및 흡수율을 조절할 수 있음을 보여주었다. 부가적으로 하이드록시아파타이트와 트리칼슘포스페이트의 비율을 일정하게 하여 다양한 방식에 의해 제작된 칼슘 포스페이트의 생체 적합성, 골전도성을 비교하는 장기간 후속 연구가 필요하다. 핵심되는말 : 골재생; 칼슘 포스페이트; 토끼 두개골; 골대채제; 제작방법